EBQ:Canadian C-spine Rule Study
PubMed Full text PDF
Contents
Clinical Question
Can a clinical decision rule be used to evaluate the cervical spine in alert and stable trauma patients?
Conclusion
The Canadian C-spine rule is a highly sensitive decision rule for evaluate of clinically significant cervical spine injuries in trauma patients.
Major Points
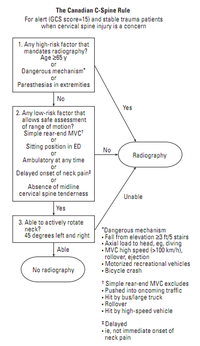
Three Main Questions:
- Is there any high-risk factor that mandates radiography?
- Is there any low-risk factor that allows safe assessment of ROM?
- Is pt able to actively rotate neck 45° to the left and right?
Rule had 100% sensitivity and 42.5% specificity for identifying 151 clinically important C-spine injuries.
Study Design
Prospective cohort study of blunt trauma patients from 10 Canadian EDs (community and university hospitals), where each pt was evaluated for 20 standardized clinical findings before radiographs (3 views). Flex/Ex views and CT C-spine underwent at discretion of treating physician. Subset of patients were also assessed by second EM physician independently. Additional 5 demographic variables obtained by study RNs from hospital records. Clinical decision rule derived using statistical means (see article for more detail)
Clinically important C-spine injury (fx, dislocation or ligamentous instability on imaging) was the primary outcome measure, which requires stabilization or specialized follow-up. The following injuries were not considered clinically important:
- Isolated avulsion fx of osteophyte
- Isolated transverse process fx involving facet joint
- Isolated spinous process fx not involving lamina
- Simple compression fx (<25% vertebral body height)
Inclusion Criteria
- Patients sustaining acute blunt trauma to head/neck, who were at risk for C-spine injury, which is defined as the following:
- Neck pain based on mechanism of injury
- No neck pain w/ some visible injury above clavicles, non-ambulatory before, and sustained dangerous mechanism
- Patient had to be alert (GCS 15) and stable (nl VS = SBP>90 and RR 10-24/min)
Exclusion Criteria
- Age <16 years old
- Minor injuries (ie simple laceration) and did not meet inclusion criteria
- GCS<15
- Grossly abnl VS
- Injured >48hrs previously
- Penetrating trauma
- Acute paralysis
- Known vertebral disease (ie RA, spine stenosis, previous C-spine injury, anklyosing spondylitis)
- Returned for reassessment of same injury
- Pregnant
Baseline Characteristics
- Mean age: 37 years old
- Sex: 51.5% male
- Neck pain: 91.5%
- Mechanism of Injury: MVA (67%) and Fall (14.3%)
- Imaging performed: Radiographs (68.9%) and CT (4.9%)
- Clinically important C-spine injury: Fx (1.6%) > Dislocation (0.3%) > Ligamentous instability (0.1%)
- Stabilizing Tx: Rigid collar (0.7%) > Halo (0.6%) > Internal fixation (0.3%) > Brace (0.2%)
- Admission: 8.1%
Outcome
n=8924 adults enrolled and assessed
Primary Outcomes
151 (1.7%) had clinically important C-spine injury
Criticisms & Further Discussion
- Complicated algorithm
- Low rate of x-rays performed
- How does it compare to the NEXUS criteria?
Funding
Peer-reviewed grants from the Medical Research Council of Canada and the Ontario Ministry of Health Emergency Health Services Committee