EBQ:Sgarbossa Criteria Study
PubMed Full text PDF
Contents
Clinical Question
How can we diagnose Acute Myocardial Infarction in patients with a Left Bundle Branch Block?
Conclusion
Sgarbossa's Criteria is a validated clinical prediction rule based on ECG criteria to diagnose Acute Myocardial Infarction in patients with a Left Bundle Branch Block. It has good specificity, but poor sensitivity.
Major Points
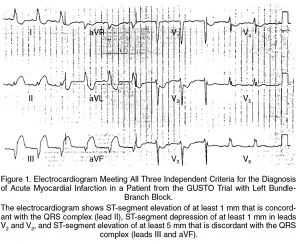
The Sgarbossa Criteria:
- ST-segment Elevation of at least 1 mm with concordance with the QRS complex with a score of 5
- ST-segment depression in leads V1, V2 or V3 with a score of 3
- ST-segment Elevation of atleast 5 mm with discordance with the QRS complex with a score of 2
With a score >3 90% of those with positive criteria will have STEMI (Good Specificity) But with negative criteria it doesn't help that much (Low sensitivity)
ECGs of patients with confirmed MIs from the GUSTO-1 trial were blindly compared with ECGs of control patients with LBBB from the Duke Databank for Cardiovascular Disease. The ECG criteria for MI in the presence of LBB was then tested against patients with chest pain and acute LBBB.
Criteria
Original Criteria
- ST elevation ≥1 mm in a lead with upward (concordant) QRS complex - 5 points
- ST depression ≥1 mm in lead V1, V2, or V3 - 3 points
- ST elevation ≥5 mm in a lead with downward (discordant) QRS complex - 2 points
- Least specific of criteria, see Smith's modification
Smith's modification
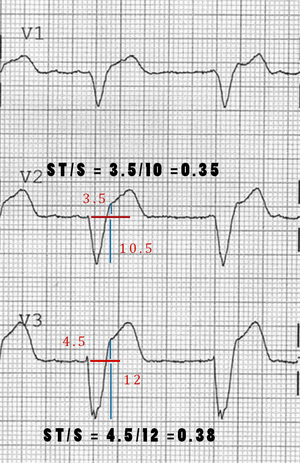
- Changes the 3rd rule of original Sgarbossa's Criteria to be ST depression OR elevation discordant w/ the QRS complex and w/ a magnitude of at least 25% of the QRS increases Sn from 52% to 91% at the expense of reducing Sp from 98% to 90%[2]
Population
Patient Demographics
- Median Age: 68 years
- Males: 64% in study group and 60% in experimental group
- Left Axis Deviation: 28% Vs. 48%
- Previous MI: 26% Vs. 59%
Inclusion Criteria
- Experiment: Patients with LBBB and Acute myocardial infarction (GUSTO-1 trial population)[3]
- Control: Patients with normal documented angiography with LBBB Randomly selected from Duke data bank for cardiovascular disease[4]
- Validation Segment: 22 patients with elevated CKMB and 23 patients with unstable angina (control patients)
Exclusion Criteria
Patients without LBBB
Outcomes
- Using univariate analysis the ods rations for the individual criteria for STEMI in the presence of LBBB were:
| Criteria | Odds Ratio | Score |
| ST-segment elevation ≥ 1mm and concordant with QRS complex | 25.2 (11.6-54.7) | 5 |
| ST-segment depression ≥ 1mm in lead V1, V2, V3 | 6.0 (1.9-19.3) | 3 |
| ST-segment elevation ≥ 5mm and discordant with QRS complex | 4.3 (1.8-10.6) | 2 |
- Validation Segment for Sgarbosa Score ≥3 to determine prescience of a STEMI
Derivation sample vs Validation Sample
- Sensitivity: 78% vs 36%
- Specificity: 90% vs 96%
- Pos. Likelihood ratio: 7.8 vs. 9.0
- Neg. Likelihood ratio: 0.2 vs 0.7
Primary Outcome
Criticisms & Further Discussion
- The Sgarbossa criteria have not been incorporated into the AHA STEMI guidelines and new LBBB has been removed from the current AHA recommendations for activation of PCI.[5]
- Although the criteria is highly specific it lacks sensitivity and can result in false positive catheterization lab activation.[6]
Funding
Grant from Bayer, Genentech, CIBA–Corning, ICI Pharmaceuticals, and Sanofi Pharmaceuticals.
See Also
References
- ↑ Sgarbossa E. et al.. "Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators". NEJM. 1996. 334(8):481-7
- ↑ Smith, S. et al. Diagnosis of ST-Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block With the ST-Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. 60(6). 766-776
- ↑ The GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med 1993;329:673-82
- ↑ Pryor DB, Califf RM, Harrell FE Jr, et al. Clinical data bases: accomplishments and unrealized potential. Med Care 1985;23:623-647
- ↑ Q. Cai, N. Mehta, E.B. Sgarbossa, S.L. Pinski, G.S. Wagner, R.M. Califf, and A. Barbagelata, "The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: from falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time?", American heart journal, 2013.PDF
- ↑ D.M. Larson, K.M. Menssen, S.W. Sharkey, S. Duval, R.S. Schwartz, J. Harris, J.T. Meland, B.T. Unger, and T.D. Henry, ""False-positive" cardiac catheterization laboratory activation among patients with suspected ST-segment elevation myocardial infarction.", JAMA : the journal of the American Medical Association, 2007