We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Capnography
From WikEM
(Redirected from End-Tidal CO2 Monitoring)
Contents
Background
- End-tidal CO2 monitors can be qualitative or quantitative
- Qualitative include calorimety devices (CO2 = blue, No CO2 = yellow)
- Quantitative include devices that give numeric values
- Mainstream (or inline) CO2 monitors are placed within the closed circuit of the ventilator (or BVM)
- Sidestream CO2 monitors use special NC to detect CO2
Basics
- Capnography measures the amount of exhaled CO2
- ETCO2 of 35-45mmHg is considered normal
- <35mmHg = Hypocapnia or Hyperventilation
- >45mmHg = Hypercapnia or Hypoventilation
- Directly measure the function of ventilation (not oxygenation)
- ETCO2 ≥ PCO2
- Indirectly measures overall metabolism (or lack there of in cardiac arrest)
Capnogram Overview
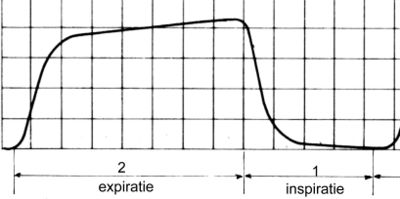
- Exhalation will first expel dead space air (Phase I)
- Then a rapid rise in CO2 rich air is noted (Phase II)
- This is followed by a more gradual increase in CO2 (Phase III)
- The curve peaks at the end of Phase III which is noted as the End-Tidal CO2 measurement
- Inhalation follows (Phase 0 or IV)
Airway Monitoring
- Ensure adequate BVM ventilation
- Assess for ETT placement using presents of measurable ETCO2 and waveform
- In out of hospital use, this had SN 1.0 and SP 1.0 in detected good placement[1]
Cardiac Arrest Monitoring
Ensure adequate chest compressions
- ETCO2 10-20mmHg signifies high quality chest compressions[2]
ROSC
- Attaining ROSC is associated with an ETCO2 jump 10mmHg with ROSC (13.5 on average)[3]
- 10mHg has a sensitivity of 33% and a specificity of 97% for ROSC[4]
- 20mHg has a sensitivity of 20% and a specificity of 99% for ROSC
- CPR does not have to be stopped for pulse checks
- Loss of ROSC can be determined by a significant drop signifies drop in ETCO2
Prognosis
Procedural Sedation Monitoring
- Pulse-ox has a lag time of sec to mins
- Capnography will show real-time respiratory changes and apnea
- ETCO2 monitoring detects clinically signifcant respiratory events before SPO2 or clinically noted apnea/hypoventilation[7]
DKA
- Adults with BG>550[8]
- ETCO2>35 mmHg has a sensitivity 100%, ETCO2<26 mmHg has specificity of 96%
- Adults with BG>250[9]
- ETCO2>24.5 mmHg has sensitivity of 90%, ETCO2<24.5 mmHg has specificity of 90%
See Also
External Links
References
- ↑ Silvestri, S, et al. The effectiveness of out-of-hospital use of continuous end-tidal carbon dioxide monitoring on the rate of unrecognized misplaced intubation within a regional emergency medical services system. Ann Emerg Med. 2005; 45(5):497-503.
- ↑ Kodali, BS, et al. Capnography during cardiopulmonary resuscitation: Current evidence and future directions. J Emerg Trauma Shock. 2014; 7(4):332–340.
- ↑ Grmec, S, et al.Utstein style analysis of out-of-hospital cardiac arrest--bystander CPR and end expired carbon dioxide. Resuscitation. 2007; 72(3):404-14.
- ↑ Tat LC, Ming PK, Leung TK. Abrupt rise of end tidal carbon dioxide level was a specific but non sensitive marker of return of spontaneous circulation in patient with out-of-hospital cardiac arrest. Resuscitation. 2016; 104:53–58.
- ↑ Eckstein, M, et al. End-Tidal CO2 as a Predictor of Survival in Out-of-Hospital Cardiac Arrest. Prehospital and Disaster Medicine. 2011; 26(3):148-150.
- ↑ Levine, R, End-tidal Carbon Dioxide and Outcome of Out-of-Hospital Cardiac Arrest. NEJM.1997. 337(5):301-6.
- ↑ Burton, JH, et al. Does End-Tidal Carbon Dioxide Monitoring Detect Respiratory Events Prior to Current Sedation Monitoring Practices. Academic Emergency Medicine. 2006; 13:500–504.
- ↑ Bou Chebl R, Madden B, Belsky J, Harmouche E, Yessayan L. Diagnostic value of end tidal capnography in patients with hyperglycemia in the emergency department. BMC Emerg Med. 2016 Jan 29;16:7.
- ↑ Soleimanpour H, Taghizadieh A, Niafar M, Rahmani F, Golzari SE, Esfanjani RM. Predictive value of capnography for suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013 Nov;14(6):590-4. doi: 10.5811/westjem.2013.4.14296.