We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Ingested foreign body
From WikEM
(Redirected from Esophageal Foreign Body)
Contents
Background
- Esophageal impaction can result in airway obstruction, stricture, or perforation. Perforation can be due to multiple mechanisms but is generally either mechanical (e.g. ingested bones) or via chemical corrosion (e.g. button battery)[1]
- Esophageal irritation can be perceived as foreign body (globus sensation)
- Once the object has traversed the pylorus, it usually passes without issue
- Exceptions: Irregular or sharp edges, particularly wide (>2.5cm) or long (>6cm) objects
- Common foreign bodies:
- Most common in children: coins
- Most common in adults: food bolus
- Site of obstruction:
Clinical Features
Adults
- Retrosternal pain
- Dysphagia
- Vomiting
- Choking
- Coughing/aspiration (if secretions pool proximal to the obstruction)
Children
Differential Diagnosis
Tracheal/lung aspiration of foreign body
Dysphagia
- Achalasia
- Esophageal foreign body
- Schatzki Ring
- Esophageal web
Pediatric stridor
<6mo
- Laryngotracheomalacia
- Vocal cord paralysis (weak cry)
- Subglottic stenosis (previous intubation)
- Airway hemangioma (usually regresses by age 5)
- Vascular ring/sling
>6mo
- Croup
- Epiglottitis
- Bacterial tracheitis
- Foreign body (sudden onset)
- Retropharyngeal abscess (muffled voice, fever)
Evaluation

Body-packing with multiple foreign bodies ("balls" of hashish) on KUB
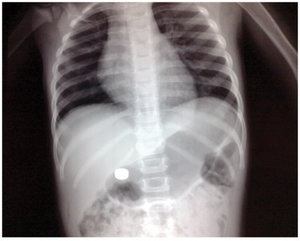
Button battery in stomach on KUB.

Imaging
- May not be needed in settings such as a known food bolus
- CXR PA and lateral
- Coins in esophagus present their face on AP view
- Coins in trachea present their face on lateral view
- Bones can only be visualized <50% of time
- Button batteries may present with "double-ring sign"
- CT chest
- Endoscopy
- Barium Swallow is not recommended due to risk of aspiration, mediastinitis, and barrium coating mucosa (makes endoscopy more difficult)
Management
Indications for Urgent Endscopy
- Complete obstruction of esophagus (pooling, risk of aspiration)[5]
- Ingestion of button batteries[6]
- Ingestion of sharp or elongated objects (toothpicks, soda can tabs)
- Ingestion of multiple foreign bodies
- Evidence of perforation
- Coin at the level of the cricopharyngeus muscle in a child
- Airway compromise
- Presence of foreign body for >24hr
- Multiple magnets (can trap bowel)
- Objects >6cm in length
Food Impaction
Uncomplicated food impaction (no bones, incomplete obstruction) can be managed expectantly but do not allow food bolus to remain impacted for >12-24hr. It is reasonable to consider therapies such as glucagon or a carbonated beverage
- Glucagon 1-2mg IV/IM (adults) to relax LES - may cause severe nausea/vomiting
- Only one RCT of glucagon with 24 patients compared glucagon to diazepam and found no difference in the need for endoscopy[7]
- The major side effect of glucagon is vomiting and can increase the risk for esophageal perforation or aspiration
- Carbonated beverage (effervescents) may be effective for small impactions (carbonation dilates esophagus)[2]
- Calcium channel blockers (nifedipine) / Benzos / Nitrates / papain (meat tenderizer) no longer recommended given low success and higher side effect profile[2]
Coin Ingestion
- Can attempt removal with a foley catheter under fluoroscopy, though not recommended as risk for aspiration or perforation
- Should be admitted to ICU and removed by GI endoscopy within 24 hours
Button Battery
- Call the National Button Battery Ingestion Hotline: 202-625-3333 (24/7) [8]
- True emergency if located in esophagus
- Perforation can occur within 6hr of ingestion
- via direct pressure or electrical conduction leading to liquefactive necrosis
- Mercury toxicity
- Obtain urgent endoscopic removal
- Perforation can occur within 6hr of ingestion
- Batteries past the esophagus can be managed expectantly with 24hr follow up
Sharp Objects
- Intestinal perforation from objects distal to stomach is common (up to 35%)
- Require immediate removal (even if located in stomach or duodenum)
- If object is distal to duodenum and patient is asymptomatic document passage with daily films
- If object is distal to duodenum and patient symptomatic obtain immediate surgery consult
Narcotics Ingestion (i.e. Body Packing)
- Multiple packets inserted in latex bags, ingested to cross borders
- Each packet potentially toxic if bag bursts
- Consider whole-bowel irrigation
- Endoscopy contraindicated (high % leakage/rupture of packets)
- Surgical removal indicated if evidence of systemic toxicity
- Do not discharge until all packets removed or 3 packet-free stools
Disposition
- Will need GI follow up as majority of the time there is a structural abnormality that may lead to recurrence (esophageal web, stricture, tumor, etc)
Complications
- Airway compromise
- Aspiration pneumonia
- Esophageal perforation/necrosis
- Mediastinitis
- Aortic perforation
- Vocal cord paralysis
- Bowel perforation/necrosis, fistulas, obstruction
- Stricture
- Infection
External Links
See Also
Video
References
- ↑ Arugula R, Dorofaeff T. Oesophageal button battery injuries: think again. Emerg Med Australas. 2011 Apr;23(2):220-3.
- ↑ 2.0 2.1 2.2 2.3 2.4 Leopard D et al. The management of oesophageal soft food bolus obstruction: a systematic review. Ann R Coll Surg Engl 2011;93:441–4. PMID: 21929913
- ↑ Loh WS, Eu DK, Loh SR, Chao SS. Efficacy of computed tomography scans in the evaluation of patients with esophageal foeign bodies. Ann Otol Rhino Laryngol. Oct 2012; 121 (10) 678- 681
- ↑ Liu YC, Zhou SH, Ling L. Value of helial computed tomography in the early diagnosis of esophageal foreign bodies in adults. Am J Emerg Med. Sep 2013;31(9),1328-32
- ↑ Ikenberry SO et al. Management of ingested foreign bodies and food impactions. Gastrointest ends 2011; 73(6): 1085-91. PMID: 21628009
- ↑ Panella NJ et al. Disk battery ingestion: case series with assessment of clinical and financial impact of a preventable disease. Pediatr Emerg Care 2013; 29(2): 165-9. PMID: 23364381
- ↑ Tibbling L et al. Effect of spasmolytic drugs on esophageal foreign bodies. Dysphagia 1995; 10(2): 126-7. PMID: 7600855
- ↑ http://www.poison.org/battery