We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Fingertip laceration
From WikEM
(Redirected from Fingertip Laceration)
Contents
Background
- Consult hand surgeon for all patients with Amputation proximal to the lunula (crescent-shaped whitish area)
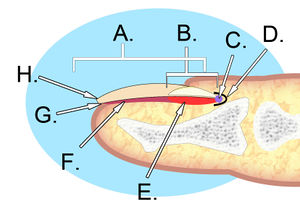
Anatomy
- The perinychium includes the nail, the nailbed, and the surrounding tissue.
- The paronychia is the lateral nail folds
- The hyponychium is the palmar surface skin distal to the nail.
- The lunula is that white semi-moon shaped proximal portion of the nail.
- The sterile matrix is deep to the nail, adheres to it and is distal to the lunule.
- The germinal portion is proximal to the matrix and is responsible for nail growth.
Clinical Features
Differential Diagnosis
Hand and finger injuries
- Radiograph positive
- Radiograph negative
- Dupeytren contracture
- Boutonniere deformity
- Hand and finger tendon injuries
- Ganglion cyst
- De Quervain tenosynovitis
- Intersection syndrome
- Drummer's wrist
- Extensor digitorum tenosynovitis
- Vaughn Jackson syndrome
- Snapping Extensor Carpi Ulnaris
- Compressive neuropathy, "bracelet syndrome"
- Scaphoid fracture
- Osteoarthritis
- Infiltrative tenosynovitis
- Gout
- Rheumatoid arthritis
- Trigger finger
- Mallet finger
- Jersey finger
- Jammed finger
- Subungual hematoma
- Fingertip laceration
- Metacarpophalangeal (MCP) ulnar ligament rupture (Gamekeeper's thumb)
- Nail avulsion
- High-pressure injection injury
Evaluation
Fingertip Zones
- Zone I - Distal to tip of phalanx
- Zone II - Between tip of phalanx and lunule
- Zone III - Proximal to lunule
Management
No exposed bone or nail bed involvement
- Zone I injuries - treat conservatively with serial dressing changes alone
- Cover wound with non-adherent dressing
- Instruct patient to soak fingertip in antibacterial soap-added water for 10min QD and then reapply non-adherent dressing
- Follow up with primary care provider in 2d
- Most will have epithelialization in approximately 1 month[1]
Exposed Bone
- Zone II injuries
- Consider hand surgery consult
- Rongeur bone if bony protuberance
- Wound closure with flap
- Follow up with hand surgery in 3-5d
- Healing time 3-6wks
- Zone III injuries
- Consult hand surgery if available
- May require distal phalanx amputation
- Consider treating like Zone II
- Healing time 3-6wks[2]
References
- ↑ Lamon, RP, et al. Open treatment of fingertip amputations. Ann Emerg Med. 1983; 12(6):358-360.
- ↑ Lamon, RP, et al. Open treatment of fingertip amputations. Ann Emerg Med. 1983; 12(6):358-360.