We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Tuberculosis
From WikEM
(Redirected from TB)
Contents
Background
- Over 1/3 of world's population is infected
Infection Types
- Primary Infection
- Usually contained by body via formation of tubercles
- Hematogenous spread limited to areas with high O2 or blood flow (apical lung, vertebrae)
- PPD positive
- Reactivation Infection
- More common in immunocompromised patients (AIDS, malignancy, DM, immunosupressive medications)
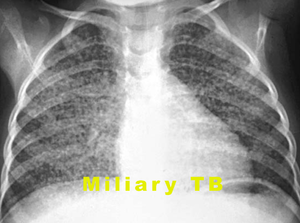
- Miliary Tuberculosis
- Disseminated tuberculosis
- Looks like millet seeds
- Seen in patients with comorbid AIDS
- Check HIV in patients suspected of TB
- PPD is positive in only 50% of cases
Special Populations
- AIDS
- TB is 200-500x more common in AIDS population than general population
- CD4 count
- Increased risk when <500
- Determines the clinical and radiographic presentations of TB
- Pediatric
- More likely to progress early to active disease
- Presentation more commonly that of primary TB
- >5yr - classic symptoms
- <5yr - milliary TB, meningitis, cervical lymphadenitis, pneumonia that does not respond to usual antibiotics
- Children are usually not infectious due to their weak cough
- More likely to progress early to active disease
Tuberculin Skin Test
- Used for population screening, but not for rule-out in patients with concern for active disease
Reaction considered positive in following situations:
- >5 mm
- HIV positive
- Close contact with active TB patient
- Nodular or fibrotic changes on CXR
- Immunosuppressed (TNF-alpha inhibitor, chemo, organ transplant)
- >10 mm
- Children < 4 yrs old
- Healthcare/lab/prison employees and residents
- Co-morbid conditions (dialysis, DM, blood/head/neck/lung malignancy, IV drug users)
- People from high prevalence areas
- >15 mm
- Persons with no known risk factors for TB
Clinical Features
Primary Tuberculosis
- Usually asymptomatic (only identified by positive PPD/quantiferon gold)
- May be rapidly progressive and fatal in immunocompromised patients
- Fever, malaise, weight loss, chest pain
- Tuberculous pleural effusion may occur if subpleural node ruptures into the pleura
- Pleuritic chest pain
- Exudative fluid
- Organisms may not be visible on acid-fast staining (need pleural biopsy)


Reactivation Tuberculosis
- Pulmonary: Productive cough, hemoptysis, dyspnea, pleuritic chest pain
- Systemic: Fever, night sweats, malaise, fatigue, wt loss
- Extrapulmonary
- Painless lymphadenopathy/scrofula (most common extrapulmonary manifestation)
- Pericarditis
- Peritonitis
- Meningitis
- Adrenal insufficiency
- Think about in the patient presenting in shock with TB risk factors
- Arthritis
- Osteomyelitis
- Pott's disease, usually in thoracic spione
Differential Diagnosis
HIV associated conditions
- HIV neurologic complications
- HIV pulmonary complications
- Ophthalmologic complications
- Other
- HAART medication side effects[1]
- Lactic acidosis
- Neuropyschiatric effects
- Hepatic toxicity
- Renal toxicity
- Steven-Johnson's
- Cytopenias
- GI symptoms
- Endocrine abnormalities
Evaluation
CXR

- Primary infection
- Infiltrates in any area of the lung
- Isolated hilar or mediastinal adenopathy may be only finding
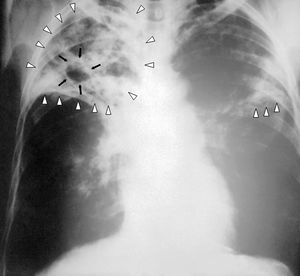
- Reactivation infection
- cavitary/noncavitary lesions in upper lobe or superior segment of lower lobe
- Latent infection
- Upper lobe or hilar nodules and fibrotic lesions
- Ghon foci, areas of scarring, calcification
- Miliary TB
- Looks like millet seeds on CXR
- Immunocompromised patients less likely to have classic lesions and may have normal CXR
PCR Sputum Assay
- Rapidly detects TB in sputum specimens (as well as rifampin resistance)
- Use to rule-out patients for active TB
- Need two sputum specimens (expectorated or induced) at least 8 hours apart (including at least one early morning specimen)
Management
Active TB
- Isoniazid + rifampin + pyrazinamide + ethambutol x 8wk followed by INH/rifampin x18wk
- 2 drug continuation treatment x 18-31wk
Latent TB
- Isoniazid x 9 months
- Consider treatment for:
- Recent conversion to PPD-positive
- close contact with active TB
- immunocompromised patients (or plan to start immunosupressive medications)
Disposition
Discharge
- Otherwise healthy
- Contact public health services before discharge
- Instructions for home isolation and follow up at appropriate clinic to receive meds
- Do not start TB meds in ED unless specifically instructed by public health
- Contact public health services before discharge
Admit
- Ill-appearing
- Diagnosis is uncertain
- Patient is treatment non-adherent
References
- ↑ Gutteridge, David L MD, MPH, Egan, Daniel J. MD. The HIV-Infected Adult Patient in The Emergency Department: The Changing Landscape of the Disease. Emergency Medicine Practice: An Evidence-Based Approach to Emergency Medicine. Vol 18, Num 2. Feb 2016.