

Basics of Parasitic/Amebic Keratitis
 ShareCompartir
ShareCompartir
Acanthamoeba Keratitis (AK)
What is Acanthamoeba keratitis?
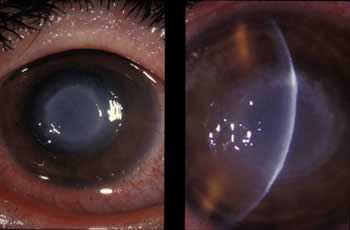
Eye infection from Acanthamoeba.
Acanthamoeba keratitis, or AK, is a rare but serious infection of the eye that can cause permanent vision loss or blindness 1. This infection is caused by a tiny ameba (single-celled living organism) called Acanthamoeba. Acanthamoeba causes Acanthamoeba keratitis when it infects the cornea, the clear dome that covers the colored part of the eye 1.
What are the symptoms of Acanthamoeba keratitis?
Symptoms of AK include: 2
- Sensation of something in the eye
- Eye pain
- Eye redness
- Blurred vision
- Sensitivity to light
- Excessive tearing
If you experience any of these symptoms, remove your contact lenses (if you wear them) and call your eye doctor right away. AK is a rare condition, but if left untreated it can result in vision loss or blindness 3.
Where is Acanthamoeba found?
Acanthamoeba is very common in nature and can be found in bodies of water (for example, lakes and oceans) and soil 4. It can also be found in tap water, heating, ventilating, and air conditioning units, and whirlpools 4. Infection of the eye occurs when the Acanthamoeba organisms contained in water or contact lens solution enter the eye through small scrapes that can be caused by contact lens wear or other minor eye injuries 5, 6. The Acanthamoeba organism has to make contact directly with the eyes in order to cause AK, so this type of corneal infection cannot occur from drinking or inhaling water that has this ameba in it 5-7. AK cannot be spread from person to person.
What puts people at risk for Acanthamoeba keratitis?
In the United States, an estimated 85% of AK cases occur in contact lens wearers 8, 9. For people who wear contact lenses, the risk of getting Acanthamoeba keratitis is higher if they:
- Do not store or handle contact lenses properly. This can include not washing hands before touching contact lenses, not rubbing and rinsing lenses after taking them out, and not storing them in the recommended contact lens solution 10, 11.
- Do not disinfect contact lenses properly. This can include using tap water to clean the lenses or lens case, or adding fresh solution to existing used solution in the case instead of using only fresh solution when storing contact lenses 9, 11-13.
- Swim, use a hot tub, or shower while wearing lenses 14-16.
- Have a history of trauma to the cornea, such as a previous eye injury 7, 17.
In 2007, CDC investigated a nationwide outbreak of Acanthamoeba keratitis which led to the recall of a specific type of contact lens solution from the market 11, 13. Another nationwide outbreak in 2011 pointed to inadequate hygiene among contact lens wearers, in addition to water exposure and "topping off"—adding fresh solution to old solution—in the contact case.
How is Acanthamoeba keratitis diagnosed?
Early diagnosis is important because early treatment can prevent AK infections from becoming more severe 3. The infection is usually diagnosed by an eye doctor based on symptoms, lab results from a scraping of the eye, and/or through a close-up eye exam that allows the eye doctor to see the ameba 2.
How is Acanthamoeba keratitis treated?
How do you prevent Acanthamoeba keratitis?
Follow these tips to keep your eyes healthy while wearing contact lenses. Your daily habits, your contact lenses and supplies, and your eye doctor are all important.
More Information
- CDC. Acanthamoeba
- Prevent Blindness. Acanthamoeba keratitis and contact lenses
- Animal Planet. Monsters Inside Me: The Eye-Eating Parasite
References
- Page MA, Mathers WD. Acanthamoeba keratitis: a 12-year experience covering a wide spectrum of presentations, diagnoses, and outcomes. J Ophthalmol. 2013;670242.
- Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: diagnosis and treatment update 2009. Am J Ophthalmol. 2009;148(4):487-99e2.
- Tu EY, Joslin CE, Sugar J, Shoff ME, Booton GC. Prognostic factors affecting visual outcome in Acanthamoeba keratitis. Ophthalmology. 2008;115(11):1998-2003.
- Visvesvara GS, Moura H, and Schuster FL. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunol Med Microbiol. 2007;50(1):1-26.
- He YG, McCulley JP, Alizadeh H, Pidherney M, Mellon J, Ubelaker JE, Stewart GL, Silvany RE, Niederkorn JY. A pig model of Acanthamoeba keratitis: transmission via contaminated contact lenses. Invest Ophthalmol Vis Sci. 1992;33(1):126-33.
- van Klink F, Alizadeh H, He Y, Mellon JA, Silvany RE, McCulley JP, Niederkorn JY. The role of contact lenses, trauma, and Langerhans cells in a Chinese hamster model of Acanthamoeba keratitis. Invest Ophthalmol Vis Sci. 1993;34(6):1937-44.
- Auran JD, Starr MB, Jakobiec FA. Acanthamoeba keratitis. A review of the literature. Cornea. 1987;6(1):2-26.
- Patel A, Hammersmith K. Contact lens-related microbial keratitis: recent outbreaks. Curr Opin Ophthalmol. 2008;19(4):302-6.
- Stehr-Green JK, Bailey TM, Visvesvara GS. The epidemiology of Acanthamoeba keratitis in the United States. Am J Ophthalmol. 1989;107(4):331-6.
- Pens CJ, da Costa M, Fadanelli C, Caumo K, Rott M. Acanthamoeba spp. and bacterial contamination in contact lens storage cases and the relationship to user profiles. Parasitol Res. 2008;103(6):1241-5.
- Joslin CE, Tu EY, Shoff ME, Booton GC, Fuerst PA, McMahon TT, Anderson RJ, Dworkin MS, Sugar J, Davis FG, Stayner LT. The association of contact lens solution use and Acanthamoeba keratitis. Am J Ophthalmol. 2007;144(2):169-80.
- Kilvington S, Shovlin J, Nikolic M. Identification and susceptibility to multipurpose disinfectant solutions of bacteria isolated from contact lens storage cases of patients with corneal infiltrative events. Cont Lens Anterior Eye. 2013;36(6):294-8.
- Verani JR, Lorick SA, Yoder JS, Beach MJ, Braden CR, Roberts JM, Conover CS, Chen S, McConnell KA, Chang DC, Park BJ, Jones DB, Visvesvara GS, Roy SL. National outbreak of Acanthamoeba keratitis associated with use of a contact lens solution, United States. Emerg Infect Dis. 2009;15(8):1236-42.
- Samples JR, Binder PS, Luibel FJ, Font RL, Visvesvara GS, Peter CR. Acanthamoeba keratitis possibly acquired from a hot tub. Arch Ophthalmol. 1984;102(5):707-10.
- Kaji Y, Hu B, Kawana K, Oshika T. Swimming with soft contact lenses: danger of Acanthamoeba keratitis. Lancet Infect Dis. 2005;5(6):392.
- Stockman LJ, Wright CJ, Visvesvara GS, Fields BS, Beach MJ. Prevalence of Acanthamoeba spp. and other free-living amoebae in household water, Ohio, USA--1990-1992. Parasitol Res. 2011;108(3):621-7.
- Sharma S, Garg P, Rao GN. Patient characteristics, diagnosis, and treatment of non-contact lens related Acanthamoeba keratitis. Br J Ophthalmol. 2000;84(10):1103-8.
- Ross J, Roy SL, Mathers WD, Ritterband DC, Yoder JS, Ayers T, Shah RD, Samper ME, Shih CY, Schmitz A, Brown AC. Clinical characteristics of Acanthamoeba keratitis infections in 28 States, 2008 to 2011. Cornea. 2014;33(2):161-8.
- Page last reviewed: November 17, 2014
- Page last updated: January 27, 2015
- Content source: