 ShareCompartir
ShareCompartir

DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/babesiosis.
Babesiosis
[Babesia divergens] [Babesia duncani] [Babesia microti] [Babesia MO-1]
Laboratory Diagnosis
Diagnosis can be made by microscopic examination of thick and thin blood smears stained with Giemsa. Repeated smears may be needed.
Antibody Detection
Diagnosis of Babesia infection should be made by detection of parasites in patients' blood smears. However, antibody detection tests are useful for detecting infected individuals with very low levels of parasitemia (such as asymptomatic blood donors in transfusion-associated cases), for diagnosis after infection is cleared by therapy, and for discrimination between Plasmodium falciparum and Babesia infection in patients whose blood smear examinations are inconclusive and whose travel histories cannot exclude either parasite.
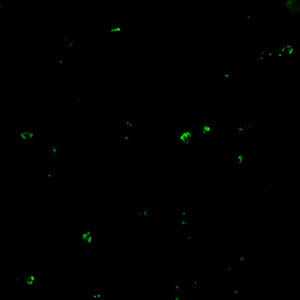
The indirect fluorescent antibody test (IFA) using B. microti parasites as antigen detects antibodies in 88-96% of patients with B. microti infection. IFA antigen slides are prepared using washed, parasitized erythrocytes produced in hamsters. Patients' titers generally rise to ≥1:1024 during the first weeks of illness and decline gradually over 6 months to titers of 1:16 to 1:256 but may remain detectable at low levels for a year or more. Specificity is 100% in patients with other tick-borne diseases or persons not exposed to the parasite. Cross-reactions may occur in serum specimens from patients with malaria infections, but generally titers are highest with the homologous antigen.
The extent of cross-reactivity between Babesia species is variable. A negative result with B. microti antigen for a patient exposed on the West Coast may be a false-negative reaction for Babesia infection. Individuals whose exposure could have occurred on the West Coast should be tested also for antibodies to the Babesia duncani, because of the lack of cross-reactivity with B. microti.
Reference:
Krause PJ, Telford S RI, Ryan R, et al. Diagnosis of babesiosis: Evaluation of a serologic test for the detection of Babesia microti antibody. J Infect Dis 1994;169:923-926.
Molecular diagnosis
In some infections with intraerythrocytic parasites, the morphologic characteristics observed on microscopic examination of blood smears do not allow an unambiguous differentiation between Babesia and Plasmodium. Moreover, potential blood donors may have subclinical symptoms and very low parasitemia, undetectable in blood smears. In such cases, the diagnosis can be derived from molecular techniques, such as PCR. In addition, molecular approaches are very valuable in investigations of new Babesia variants (or species) observed in recent human infections in the United States and in Europe.
References:
1. Hojgaard A, Lukacik G, Piesman J. Detection of Borrelia burgdorferi, Anaplasma phagocytophilum and Babesia microti, with two different multiplex PCR assays. Ticks and Tick-borne Diseases 2014 (5):349–351.
2. Bonnet S, Jouglin M, Malandrin L, Becker C, A. Agoulon A, L’Hostis M, Chauvin A. Transstadial and transovarial persistence of Babesia divergens DNA in Ixodes ricinus ticks fed on infected blood in a new skin-feeding technique. Parasitol 2007;134:197–207.
