


Case #247 - March, 2009
 ShareCompartir
ShareCompartir
A patient, originally from Ethiopia but living in the United States for the past five years, presented to her primary care provider with complaints of abdominal pain. A computed tomography (CT) scan was performed, and cysts were observed in the liver. Serologic testing for Hepatitis B Virus, amebiasis, and echinococcosis were all negative. An aspirate from one of the cysts was drawn, and sent to a pathology laboratory for work-up. Slides made from the specimen were eventually forwarded to the CDC-DPDx for diagnostic assistance. The following images show was what observed on a Papanicolaou-stained (PAP) slide of the specimen. Figures A, B, C and E were taken at 500x magnification; Figures D and F were taken at 1000x magnification. What is your diagnosis? Based on what criteria? What other testing, if any, would you recommend?
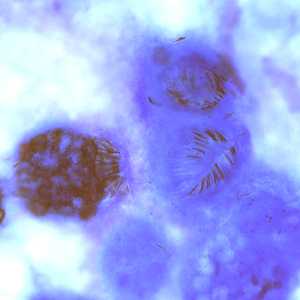
Figure A
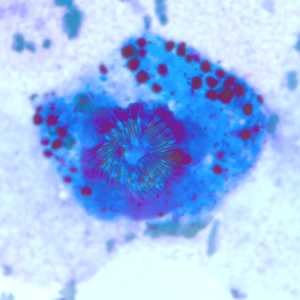
Figure B
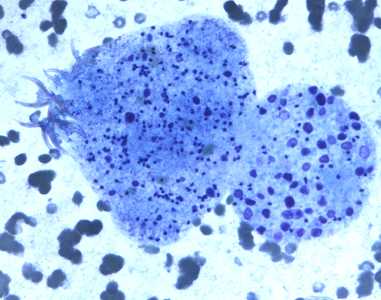
Figure C
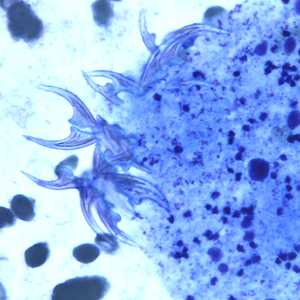
Figure D
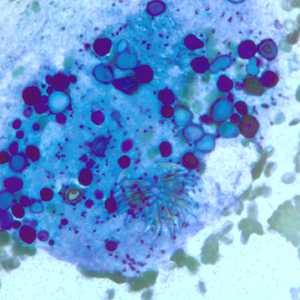
Figure E
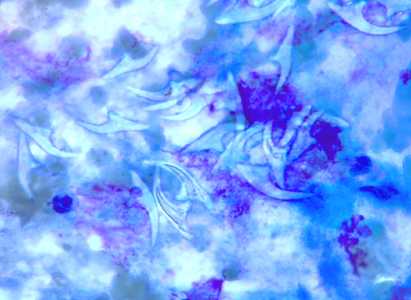
Figure F
Case Answer
This was a case of echinococcosis, caused by a tapeworm in the genus, Echinococcus. Diagnostic features included:
- the presence of multiple protoscoleces in the hydatid cyst (Figure A).
- the presence of evaginated protoscoleces (Figure C).
- the presence of hooklets consistent with those of the Taeniidae.
- the presence of calcareous corpuscles.
Many of the protoscoleces observed in this specimen were in a state of degeneration, resulting in the liberation of free calcareous corpuscles and hooklets (best seen in Figures E and F, respectively). The term used to describe the particulate matter within a hydatid cyst, including degenerating protoscoleces, hooklets, calcareous corpuscles and daughter cysts, is ‘hydatid sand.' Although the species was not identified in this case, the travel history best supports E. granulosus.
The DPDx Team also recommended sending another serum specimen for reference testing at the CDC. Testing on the follow-up serum specimen was positive for echinococcosis using the CDC immunoblot. If a parasitic disease is suspected, but serology results are equivocal or inconsistent with the clinical diagnosis, repeat testing at a reference laboratory is recommended.
More on: Echinococcosis
This case was kindly provided by CellNetix Pathology in Seattle, WA.
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: August 24, 2016
- Page last updated: August 24, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: