


Pediculosis
 ShareCompartir
ShareCompartir
[Pediculus humanus capitis] [Pediculus humanus humanus]
Causal Agent
Pediculosis is infestation with the human head-and-body louse, Pediculus humanus. There are two subspecies, the head louse (P. h. capitis) and the body louse (P. h. humanus). They are ectoparasites whose only known hosts are humans. Recent molecular data suggest that the two subspecies are ecotypes of the same species and that evolution between the two populations take place continually.
Reference: Veracz A, Raoult D. 2012. Biology and genetics of human head and body lice. Trends in Parasitology. 28: 563-571.
Life Cycle

The life cycle of the head louse has three stages: egg, nymph, and adult.
Eggs: Nits are head lice eggs. They are hard to see and are often confused for dandruff or hair spray droplets. Nits are laid by the adult female and are cemented at the base of the hair shaft nearest the scalp  . They are 0.8 mm by 0.3 mm, oval and usually yellow to white. Nits take about 1 week to hatch (range 6 to 9 days). Viable eggs are usually located within 6 mm of the scalp.
. They are 0.8 mm by 0.3 mm, oval and usually yellow to white. Nits take about 1 week to hatch (range 6 to 9 days). Viable eggs are usually located within 6 mm of the scalp.
Nymphs: The egg hatches to release a nymph  . The nit shell then becomes a more visible dull yellow and remains attached to the hair shaft. The nymph looks like an adult head louse, but is about the size of a pinhead. Nymphs mature after three molts (
. The nit shell then becomes a more visible dull yellow and remains attached to the hair shaft. The nymph looks like an adult head louse, but is about the size of a pinhead. Nymphs mature after three molts ( ,
,  ) and become adults about 7 days after hatching.
) and become adults about 7 days after hatching.
Adults: The adult louse is about the size of a sesame seed, has 6 legs (each with claws), and is tan to grayish-white  . In persons with dark hair, the adult louse will appear darker. Females are usually larger than males and can lay up to 8 nits per day. Adult lice can live up to 30 days on a person's head. To live, adult lice need to feed on blood several times daily. Without blood meals, the louse will die within 1 to 2 days off the host.
. In persons with dark hair, the adult louse will appear darker. Females are usually larger than males and can lay up to 8 nits per day. Adult lice can live up to 30 days on a person's head. To live, adult lice need to feed on blood several times daily. Without blood meals, the louse will die within 1 to 2 days off the host.
Body lice: Body lice are morphologically similar to head lice. They have a different life cycle, whereas body lice reside on and lay their eggs on the clothing and fomites of infected individuals and migrate to the human body to feed.
Geographic Distribution
Head lice infestation is very common and is distributed worldwide. Preschool and elementary-age children, 3 to 11 years of age are infested most often. Females are infested more often than males, probably due to more frequent head to head contact. Body lice are also cosmopolitan but are less common and usually seen in settings of poverty, war, and homelessness.
Clinical Presentation
The majority of head lice infestations are asymptomatic. When symptoms are noted they may include a tickling feeling of something moving in the hair, itching, caused by an allergic reaction to louse saliva, and irritability. Secondary bacterial infection may be a complication. Body lice can serve as vectors for Rickettsia prowazekii (epidemic typhus), Bartonella quintana (trench fever), and Borrelia recurrentis (louse-borne relapsing fever).
Modes of Transmission:
The main mode of transmission of head lice is contact with a person who is already infested (i.e., head-to-head contact). Contact is common during play (sports activities, playgrounds, at camp, and slumber parties) at school and at home.
Less commonly, transmission via fomites may occur with regards to head lice (more common with body lice). Wearing clothing, such as hats, scarves, coats, sports uniforms, or hair ribbons worn by an infested person; using infested combs, brushes or towels; or lying on a bed, couch, pillow, carpet, or stuffed animal that has recently been in contact with an infested person may result in transmission. Of note, both nymph and adult lice forms need to feed on blood to live. If an adult louse does not have a blood meal, it can die in 2 days.
Head and Body Lice adults.

Figure A: Adult of P. humanus capitis.
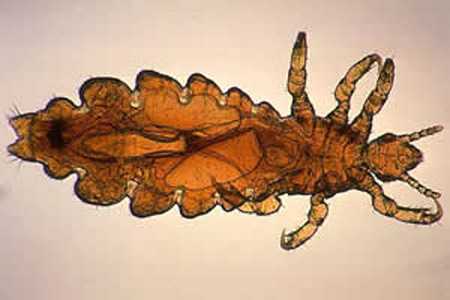
Figure B: Adult female of P. humanus capitis. In this specimen, eggs can be observed in the abdomen.

Figure C: Adult of P. humanus.
Head and Body Lice nits.

Figure A: Egg ('nit') of P. humanus capitis, with a first-instar nymph starting to hatch out.

Figure B: Empty shell of the nit in Figure A, the nymph having left.
Diagnostic Findings
The diagnosis of pediculosis is best made by finding a live nymph or adult louse on the scalp or in the hair of a person. Finding numerous nits within 6 mm of the scalp is highly suggestive of active infestation. Finding nits only more than 6 mm from the scalp is only indicative of previous infestation.
Treatment Information
- Both over-the-counter and prescription medications are available for treatment of head lice infestations.
- Treatment for head lice is recommended for persons diagnosed with an active infestation. All household members and other close contacts should be checked; those persons with evidence of an active infestation should be treated. Some experts believe prophylactic treatment is prudent for persons who share the same bed with actively-infested individuals. All infested persons (household members and close contacts) and their bedmates should be treated at the same time.
- Retreatment of head lice usually is recommended because no approved pediculicide is completely ovicidal. To be most effective, retreatment should occur after all eggs have hatched but before before new eggs are produced. The retreatment schedule can vary depending on the pediculicide used.
- Removal of all nits after successful treatment with a pediculicide is not necessary to prevent further spread. Removal of nits after treatment with a pediculicide may be done for aesthetic reasons, or to reduce diagnostic confusion and the chance of unnecessary retreatment. Because pediculicides are not 100% ovicidal (i.e. do not kill all the egg stages), some experts recommend the manual removal of nits that are attached within ¼ inch of the base of the hair shaft.
- Treatments for head lice are generally safe and effective when used correctly. Some treatments may cause an itching or a mild burning sensation caused by inflammation of the skin on the scalp. Most products used to treat head lice are pesticides that can be absorbed through the skin. Therefore, all medicines used for the treatment of lice should be used with care and only as directed.
- When treating head lice, supplemental measures can be combined with recommended medicine (pharmacologic treatment); however, such additional (non-pharmacologic) measures generally are not required to eliminate a head lice infestation. For example, hats, scarves, pillow cases, bedding, clothing, and towels worn or used by the infested person in the 2-day period just before treatment is started can be machine washed and dried using the hot water and hot air cycles because lice and eggs are killed by exposure for 5 minutes to temperatures greater than 53.5°C (128.3°F). Items that cannot be laundered may be dry-cleaned or sealed in a plastic bag for two weeks. Items such as hats, grooming aids, and towels that come in contact with the hair of an infested person should not be shared. Vacuuming furniture and floors can remove an infested person’s hairs that might have viable nits attached.
- Ivermectin has been used successfully to treat lice; however, ivermectin currently has not been approved by the U.S. Food and Drug Administration (FDA) for treatment of lice.
DPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: May 3, 2016
- Page last updated: May 3, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: