


Overview and Evidence to Support Stewardship
 ShareCompartir
ShareCompartir
 CDC Medscape Commentary: Taking an Antibiotic Timeout [ 4:54 ]
CDC Medscape Commentary: Taking an Antibiotic Timeout [ 4:54 ]
November 15, 2010
Overview
Get Smart for Healthcare is focused on improving antibiotic use in inpatient healthcare settings such as acute-care facilities through the implementation of antibiotic stewardship programs designed to ensure that hospitalized patients receive the right antibiotic, at the right dose, at the right time, and for the right duration.
Antimicrobial stewardship interventions have been proven to improve individual patient outcomes, reduce the overall burden of antibiotic resistance, and save healthcare dollars. If everyone — healthcare providers, hospital administrators, policy makers, and patients — works together to employ effective antibiotic stewardship programs, we can improve patient care, more effectively combat antibiotic resistance and ultimately save lives.
Fast Facts
- Antibiotics are a shared resource – and becoming a scarce resource.
- 30-50% of antibiotic use in hospitals is unnecessary or inappropriate.
- Antibiotic overuse contributes to the growing problems of Clostridium difficile infection and antibiotic resistance in healthcare facilities.
- Reducing unnecessary antibiotic use can decrease antibiotic resistance, Clostridium difficile infections, and healthcare costs, and improve patient outcomes.
- Interventions to improve antibiotic use can be implemented in any healthcare setting—from the smallest to the largest.
- Improving antibiotic use is a medication-safety and patient-safety issue.
Antimicrobial Stewardship Fact Sheets
- Making Health Care Safer – Antibiotic Rx in Hospitals: Proceed with Caution [PDF – 1.4 MB]
- For additional Antimicrobial Stewardship Fact Sheets, please see: https://www.cdc.gov/getsmart/week/promotional-materials/print-products.html.
- Percent of Hospitals with Antibiotic Stewardship Programs by State, 2014 [PDF – 473K]
Slide Sets
Training Slide Sets
Antimicrobial Resistance Across the Continuum of Care
 Antimicrobial Resistance Across the Continuum of Care: Winning the War One Battle at a Time (Note: CME has expired)
Antimicrobial Resistance Across the Continuum of Care: Winning the War One Battle at a Time (Note: CME has expired)
Antimicrobial Stewardship for the Community Hospital: Practical Tools & Techniques for Implementation
This educational initiative was designed to overcome and address the barriers to facilitate practical implementation of Antimicrobial Stewardship Programs in the community hospital setting led by the hospital pharmacist and infectious disease specialist in conjunction with other collaborating physician specialties. These sessions were recorded during a scientific roundtable meeting that was presented by the Centers for Disease Control and Prevention and titled “Antimicrobial Stewardship for the Community Hospital: Practical Tools & Techniques for Implementation,” which took place on August 24, 2010, in Atlanta, Georgia. Cooperating organizations for this initiative include the American Medical Association, the Association for Professionals in Infection Control and Epidemiology, the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the Society of Hospital Medicine, and the Society of Infectious Diseases Pharmacists.
-
 Addressing the Rising Tide of Antimicrobial Resistance: Why Something Must Be Done
Addressing the Rising Tide of Antimicrobial Resistance: Why Something Must Be Done
John G. Bartlett, MD (29:15) -
The Proven Benefits of Antimicrobial Stewardship
Christopher A. Ohl, MD (41:12)
-
Assessing the Current Status of Antimicrobial Stewardship in Your Hospital
Edward J. Septimus, MD, FIDSA, FACP, FSHEA (38:44)
-
Management of Asymptomatic Bacteriuria in Hospitalized Patients: Room for Improvement
Sara E. Cosgrove, MD, MS, FSHEA (36:31) -
The CMS Core (Performance) Measures for Community-Acquired Pneumonia (CAP): Relating to Antimicrobial Stewardship
Thomas M. File Jr, MD, MSc, MACP, FIDSA, FCCP (41:11) -
Antimicrobial Prophylaxis in the Surgical Setting: Practical Application in Smaller Hospitals
Joseph S. Solomkin, MD, FACS, FIDSA (25:25) -
The Face of Stewardship in Community Hospitals Today
Elizabeth Dodds Ashley, PharmD, MHS, BCPS (29:00)
-
Implementing an Antimicrobial Stewardship Program: The Pivotal Role of the Hospital Pharmacist
Robert C. Owens Jr, PharmD (36:39) -
Appropriate Antibiotic Usage and Public Health: The Perspective From the CDC
Arjun Srinivasan, MD, FSHEA (19:11)
Faculty
-
Arjun Srinivasan, MD, FSHEA (Co-chair)
CDR, USPHS
Associate Director for Healthcare Associated Infection Prevention Programs
Medical Director, Get Smart for Healthcare
Division of Healthcare Quality Promotion
Centers for Disease Control and Prevention
Atlanta, GA -
Christopher A. Ohl, MD
Associate Professor of Medicine
Section on Infectious Diseases
Wake Forest University School of Medicine
Winston-Salem, NC -
Edward J. Septimus, MD, FIDSA, FACP, FSHEAClinical Professor of Internal Medicine
Texas A&M Health Science Center
Medical Director
Infection Prevention and Epidemiology
HCA Healthcare System
Houston, TX -
Elizabeth S. Dodds Ashley, PharmD, MHS, BCPS
Associate Director of Clinical Pharmacy Services
University of Rochester Medical Center
Rochester, NY -
John G. Bartlett, MD
Professor of Medicine and Epidemiology
Johns Hopkins University School of Medicine
Baltimore, MD
-
Robert C. Owens Jr., PharmD (Co-chair)
Co-Director, Antimicrobial Stewardship Program
Clinical Pharmacy Specialist, Infectious Diseases
Department of Pharmacy Services and Division of Infectious Diseases
Maine Medical Center
Portland, ME -
Joseph S. Solomkin, MD, FACS, FIDSA
Professor Emeritus of Surgery
Department of Surgery
University of Cincinnati College of Medicine
Cincinnati, OH -
Sara E. Cosgrove, MD, MS, FSHEA
Associate Professor of Medicine
Division of Infectious Diseases
Director, Antibiotic Management Program
Associate Hospital Epidemiologist
Johns Hopkins Medical Institutions
Baltimore, MD -
Thomas M. File Jr., MD, MSc, MACP, FIDSA, FCCP
Professor, Internal Medicine
Head of Infectious Disease Section
Northeastern Ohio Universities
Colleges of Medicine & Pharmacy
Rootstown, OH
Chief, Infectious Disease Service
Summa Health System, Akron, OH
The faculty reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:
John G. Bartlett, MD: Advisory Board: Tibotec, Salient, Optimer; Honoraria: Abbott, Merck
Sara Cosgrove, MD, MS, FSHEA: Advisory Board: Forest, Rib-X; Consultant: Merck; Grant Recipient: Cubist, Astellas, Advan-Dx
Elizabeth S. Dodds Ashley, PharmD, MHS, BCPS: Consultant: Pfizer; Speakers Bureau: Merck
Thomas M. File Jr., MD, MSc, MACP, FIDSA, FCCP: Advisory Board: GlaxoSmithKline, Pfizer, Merck, Novartis, Cerexa, Forest, Protez, Nabriva, Tetraphase; Research Grant Recipient: Cerexa, Forest, Pfizer, Boehringer Ingelheim, Gilead, Tibotec
Christopher A. Ohl, MD: Advisory Board: Johnson & Johnson; Consultant: Johnson & Johnson; Speakers Bureau: Pfizer, Cubist
Robert C. Owens Jr., PharmD: Consultant: TheraDoc, Premiere
Edward J. Septimus, MD, FIDSA, FACP, FSHEA: Grant Recipient: AHRQ/CDC; Speakers Bureau: Cubicin, Merck, Sage
Joseph S. Solomkin, MD, FACS, FIDSA: Advisory Board: Johnson & Johnson, Merck, Optimer; Consultant: Cubist; Grant Recipient: Pfizer
CDR Arjun Srinivasan, MD, FSHEA: Nothing to Disclose
Non-faculty content contributors and/or reviewers reported the following relevant financial relationships that they or their spouse/partner have with commercial interests:
Otto Ratz, MD; Josh Paul; Bradley Pine; Blair St. Amand; Jay Katz; Kay Weigand; Paula Larson; Nothing to Disclose
References to Support Stewardship
There is a plethora of evidence to support the case for antibiotic stewardship interventions. Here are a few that highlight impact on costs, reduction of Clostridium difficile infections, use, and more.
Vital Signs: Improving Antibiotic Use Among Hospitalized Patients
PDF version [PDF – 357 KB]
Vital Signs Technical Appendix:
Estimating the Potential Reductions in Clostridium difficile Infection (CDI) among Patients when Antibiotic Use is Improved.
Antibiotic Stewardship Program Data
All of the following graphics are provided as a digital image (.jpg or .png formats) at a resolution that is acceptable for electronic and office print use.
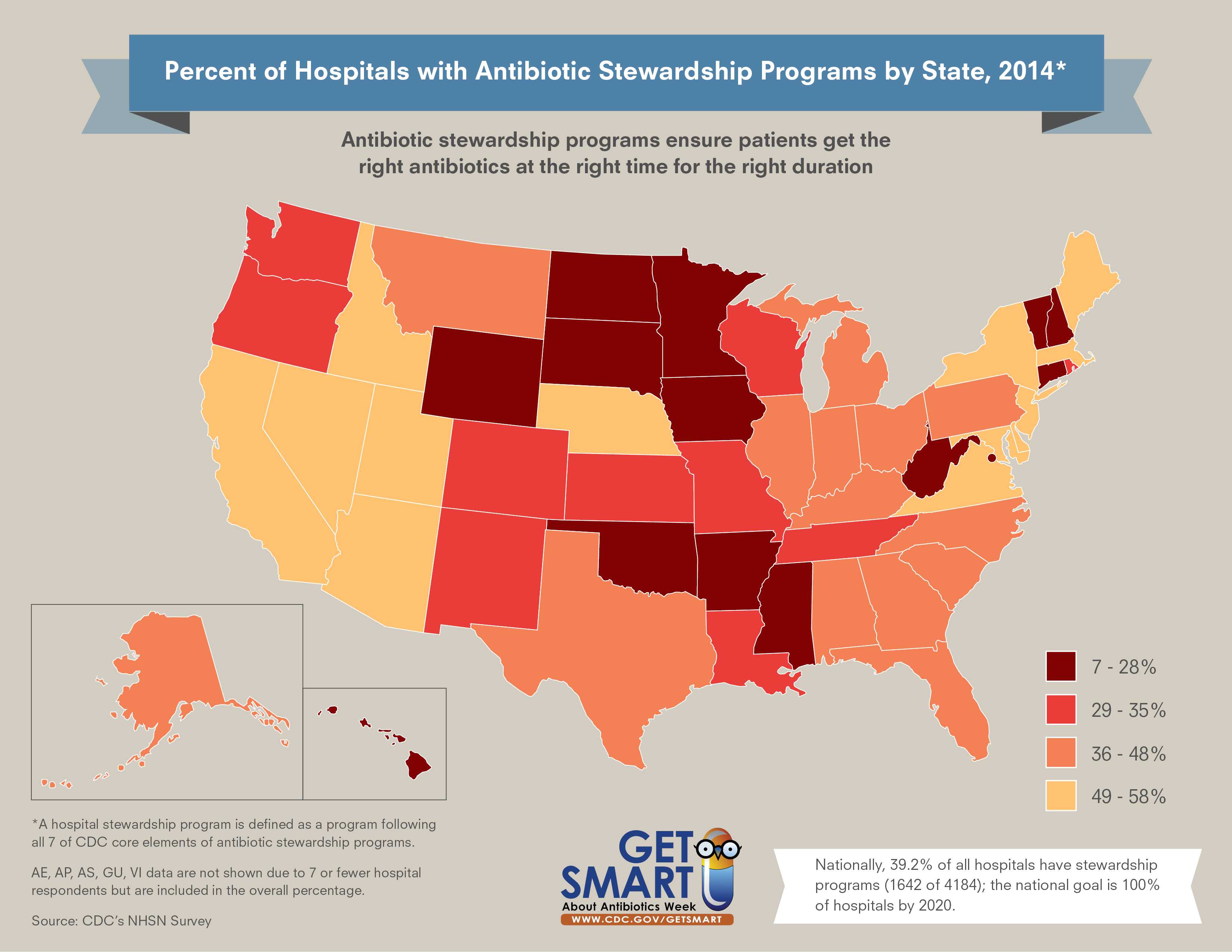
The map shows the percentage of antibiotic stewardship programs in US hospitals by state. Antibiotic stewardship programs ensure patients get the right antibiotics at the right time for the right duration.
2015

Target Audience: General public and healthcare professionals
Download or print this graphic (300 dpi resolution)
{kind=link}

Download or print this graphic (300 dpi resolution)
{kind=link}
2014

Download or print this graphic (300 dpi resolution)
{kind=link}
View outpatient antibiotic prescription data from QuintilesIMS (formerly IMS Health) Xponent data and U.S. Census files in an interactive database, CDC’s Antibiotic Resistance Patient Safety Atlas.
![]()
- Page last reviewed: February 17, 2017
- Page last updated: February 17, 2017
- Content source: