

Use of Electronic Health Records in Residential Care Communities
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 128, September 2013
On This Page
- Key findings
- Most residential care communities did not use electronic health records in 2010, and use varied by facility characteristics.
- Residential care communities that used electronic health records varied in the types of information captured in their computerized systems.
- Less than one-half of residential care communities that used electronic health records had a computerized system that supported exchange of electronic health information with other service providers.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (607 KB)
Christine Caffrey, Ph.D., and Eunice Park-Lee, Ph.D.
Key findings
- In 2010, only 17% of residential care communities in the United States used electronic health records.
- Residential care communities that used electronic health records were more likely to be larger, not-for-profit, chain-affiliated, colocated with another care setting, and in a nonmetropolitan statistical area.
- The types of information most commonly tracked electronically by residential care communities that used electronic health records were medical provider information, resident demographics, individual service plans, and lists of residents' medications and active medication allergies.
- Four in 10 residential care communities that used electronic health records also had support for electronic exchange of health information with service providers; nearly 25% could exchange with pharmacies, and 17% could exchange with physicians.
The ability to record and exchange health information electronically is believed to improve the quality and efficiency of health care (1–4). It also has the potential to increase coordination of care across a continuum of providers, decrease duplication of testing (5), and allow providers timely access to necessary health information. Although research has been done in other health care settings (6–9), little has been focused on residential care communities' use of electronic health records and their support for electronic exchange of resident health information (10). This report provides baseline findings using data from the 2010 National Survey of Residential Care Facilities (NSRCF).
Keywords: long-term care, health information technology, National Survey of Residential Care Facilities
Most residential care communities did not use electronic health records in 2010, and use varied by facility characteristics.
Figure 1. Percentages of residential care communities using electronic health records, by selected community characteristics: United States, 2010

NOTES: For all characteristics, differences were significant at p < 0.05. Figure excludes cases with missing data; see “Data source and methods ” section for details.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
- In 2010, only 17% of residential care communities used electronic health records (Figure 1).
- One-quarter of larger residential care communities (those with 26 or more beds) used electronic health records, compared with 14% of smaller communities (4–25 beds).
- Not-for-profit (26%) and chain-affiliated (23%) residential care communities were more likely to use electronic health records than for-profit (16%) and nonchain (14%) communities.
- Residential care communities colocated with another care setting (29%) and located in a nonmetropolitan statistical area (22%) were more likely than those not colocated (14%) and in a metropolitan statistical area (16%) to use electronic health records.
Residential care communities that used electronic health records varied in the types of information captured in their computerized systems.
Figure 2. Percentages of residential care communities using electronic health records that tracked selected types of resident health information in a computerized system: United States, 2010
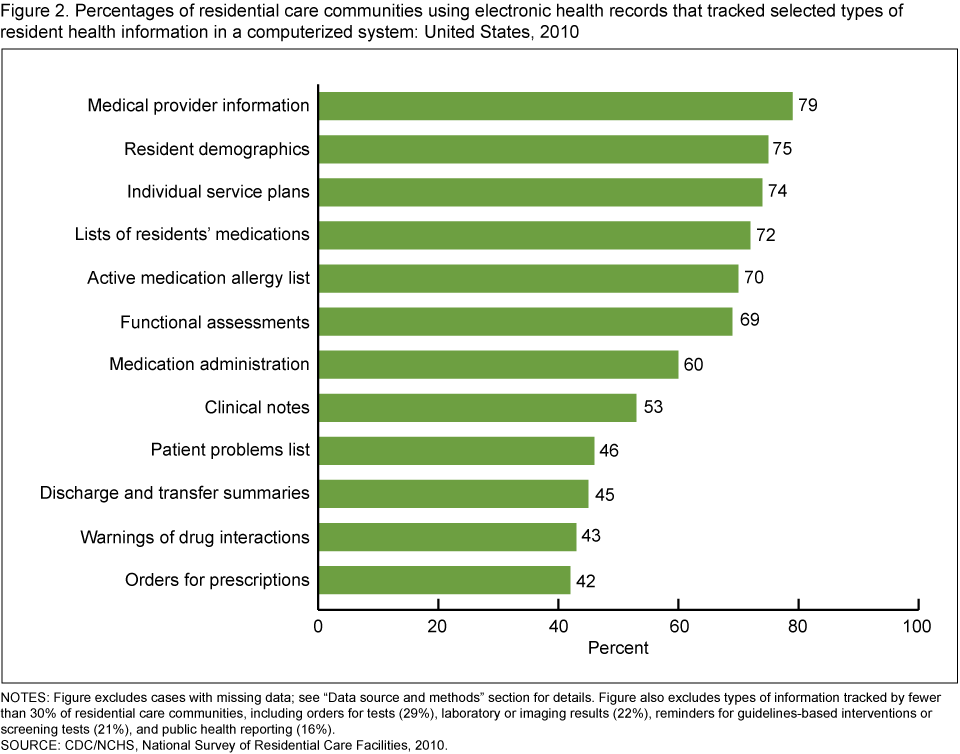
NOTES: Figure excludes cases with missing data; see “Data source and methods ” section for details. Figure also excludes types of information tracked by fewer than 30% of residential care communities, including orders for tests (29%), laboratory or imaging results (22%), reminders for guidelines-based interventions or screening tests (21%), and public health reporting (16%).
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
- At least 7 in 10 residential care communities that used electronic health records also tracked medical provider information (79%), resident demographics (75%), individual service plans (74%), and lists of residents' medications (72%) and active medication allergies (70%) using a computerized system.
- More than one-half of residential care communities that used electronic health records tracked functional assessments (69%), medication administration (60%), and clinical notes (53%).
- About 4 in 10 residential care communities that used electronic health records tracked patient problems (46%), discharge and transfer summaries (45%), warnings of drug interactions or contraindications (43%), and orders for prescriptions (42%) (Figure 2).
- Less than one-third of residential care communities that used electronic health records tracked orders for tests (29%), laboratory or imaging results (22%), reminders for guidelines-based interventions or screening tests (21%), and public health reporting (16%).
Less than one-half of residential care communities that used electronic health records had a computerized system that supported exchange of electronic health information with other service providers.
Figure 3. Percentages of residential care communities using electronic health records that had a computerized system to support electronic health information exchange with other providers, by provider type: United States, 2010

1Includes hospitals, nursing homes, and other long-term care providers.
2Includes laboratories, residents’ personal health records, and public health reporting.
NOTE: Figure excludes cases with missing data; see “Data source and methods ” section for details.
SOURCE: CDC/NCHS, National Survey of Residential Care Facilities, 2010.
- Among residential care communities that used electronic health records, 23% had computerized systems for electronic health information exchange with pharmacies, and 17% could exchange with physicians (Figure 3).
- One-fifth of residential care communities that used electronic health records had computerized support to electronically exchange health information with other health or long-term care providers, such as hospitals and nursing homes.
Summary
In 2010, 17% of residential care communities reported that they used electronic health records. These communities had different characteristics than those without electronic health records. Communities that had electronic health records were more likely to be larger, to have not-for-profit ownership, to be colocated with other care settings, and to be in a nonmetropolitan statistical area. Medical provider information, resident demographics, individual service plans, and lists of residents' medications and active medication allergies were the most common categories of resident health information recorded using a computerized system. Forty percent of residential care communities that used electronic health records had a computerized system that supported electronic health information exchange with one or more types of service providers. Almost one-quarter had computerized support for exchanging electronic health information with pharmacies.
This report has provided baseline findings on the use of electronic health record and electronic health information exchange systems by residential care communities. This information should be relevant to discussions on the role of residential care communities; the effective transition from hospitals to residential care communities or other long-term care settings; avoidable rehospitalizations; and helping persons who live with multiple chronic conditions better manage their health care.
Definitions
Residential care communities: Includes assisted-living facilities and similar residential care communities (e.g., personal care homes, adult care homes, board care homes, and adult foster care) that meet the study eligibility criteria described in the "Data source and methods " section.
Electronic health records: Use was identified based on provider self-report in response to the question, "Other than for accounting or billing purposes, does this facility use electronic health records? This is a computerized version of the resident's health and personal information used in the management of the resident's health care." All providers were asked this question.
Computerized resident health information: Use was identified based on provider self-report in response to the question, "Which of the following computerized capabilities does this facility have?" Included were 16 types of computerized resident health information: resident demographics, medical provider information, functional assessments, individual service plans, clinical notes, patient problems list, medication administration, lists of residents' medications and active medication allergies, orders for prescriptions, warning of drug interactions or contraindications, orders for tests, laboratory and imaging results, reminders for guidelines-based interventions or screening tests, discharge and transfer summaries, and public health reporting. All providers were asked this question.
Electronic health information exchange system: Use was identified based on provider self-report in response to the question, "Does this facility's computerized system support electronic health information exchange with any of the following?" Nine different types of service providers were included: physician, nursing home, hospital, pharmacy, laboratories, other health or long-term care provider, residents' personal health record, public health reporting, and corporate office. To be asked this question, residential care communities had to have a computerized system for tracking at least 1 of the 16 different types of resident health information. Residential care communities that did not track any of these types of information were coded as not having a computerized system that supported electronic health information exchange with other service providers. Four percent of residential care communities with electronic health records reported that they did not track any of these types of resident health information in a computerized system.
Size: Categorized into two sizes based on the number of licensed, registered, or certified beds (occupied and unoccupied) in a residential care community: 4–25 beds and 26 or more beds.
Ownership type: Categorized into two ownership types: private, for-profit; and not-for-profit. The private, for-profit category included publicly traded facilities. Not-for-profit included private nonprofit, as well as state, county, or local government ownership.
Chain affiliation: Having more than one community under common ownership or management. This may include communities in-state or across multiple states. If communties were owned by a chain, group, or multifacility system, they were coded as chain-affiliated.
Colocation with another care setting: Determined based on provider self-report in response to the question, "Are any of the following types of places on the same property or at this same location?" Four types of places were included: independent living; nursing home; rehabilitation, subacute, or postacute unit in a nursing home; and hospital. Residential care communities were considered to be colocated with another care setting if they had one or more of these places on the same property or at the same location.
Metropolitan statistical area: Refers to a county or group of contiguous counties that contain at least one urbanized area with a population of 50,000 or more. A metropolitan statistical area may contain other counties that are economically and socially integrated with the central county, as measured by commuting.
Data source and methods
Facility data from the 2010 NSRCF, conducted by the Centers for Disease Control and Prevention's (CDC) National Center for Health Statistics (NCHS), were used for these analyses. To be eligible for the study, residential care communities must (a) have been licensed, registered, listed, certified, or otherwise regulated by the state and have four or more licensed, certified, or registered beds; (b) have at least one resident currently living in the community; and (c) provide room and board with at least two meals a day, around-the-clock onsite supervision, and help with personal care such as bathing and dressing or health-related services such as medication management. These communities served a predominantly adult population. Communities licensed to serve severely mentally ill or intellectually or developmentally disabled populations exclusively were excluded. Nursing homes were also excluded unless they had a unit or wing that met the above definition and residents could be enumerated separately.
The 2010 NSRCF used a stratified two-stage probability sampling design. The first stage was the selection of residential care communities from the sampling frame representing the universe of residential care communities in the United States. For the 2010 NSRCF, 3,605 residential care communities were sampled with probability proportional to size. Interviews were completed with 2,302 residential care communities, for a first-stage community unweighted response rate of 79% and a weighted response rate (for differential probabilities of selection) of 81%. The second stage involved the selection of current residents; details on this stage, and on other aspects of sampling design and data collection, are available elsewhere (11).
Differences among subgroups were evaluated using chi-square and t tests. All significance tests were two-sided, using p < 0.05 as the level of significance. The difference between any two estimates is mentioned in the text only if it is statistically significant. Data analyses were performed using SAS-callable SUDAAN (12,13). Cases with missing data were excluded from the analyses on a variable-by-variable basis: 0.10% for electronic health records, 0.14% for computerized records of resident health information, and 0.13% for electronic health information exchange. Because estimates were rounded, individual estimates may not sum to totals.
About the authors
Christine Caffrey and Eunice Park-Lee are with CDC's National Center for Health Statistics, Division of Health Care Statistics.
References
- Kuperman GJ. Health-information exchange: Why are we doing it, and what are we doing? J Am Med Inform Assoc 18(5):678–82. 2011.
- Brailer DJ. Interoperability: The key to the future health care system. Health Aff (Millwood) (suppl Web exclusives):W5-19–W5-21. 2005.
- Bipartisan Policy Center, Task Force on Delivery System Reform and Health IT. Transforming health care: The role of health IT. 2012.
- Resnick HE, Manard BB, Stone RI, Alwan M. Use of electronic information systems in nursing homes: United States, 2004. J Am Med Inform Assoc 16(2):179–86. 2009.
- Stewart BA, Fernandes S, Rodriguez-Huertas E, Landzberg M. A preliminary look at duplicate testing associated with lack of electronic health record interoperability for transferred patients. J Am Med Inform Assoc 17(3):341–4. 2010.
- Bercovitz A, Sengupta M, Jamison P. Electronic medical record adoption and use in home health and hospice [PDF 993 KB]. NCHS data brief, no 45. Hyattsville, MD: National Center for Health Statistics. 2010.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices [PDF 38 KB]. NCHS data brief, no 111. Hyattsville, MD: National Center for Health Statistics. 2012.
- Jha AK, DesRoches CM, Campbell EG, Donelan K, Rao SR, Ferris TG, et al. Use of electronic health records in U.S. hospitals. N Engl J Med 360(16):1628–38. 2009.
- Pearson WS, Bercovitz AR. Use of computerized medical records in home health and hospice agencies : United States, 2000 [PDF 1.64 MB]. Vital Health Stat 13(161). 2006.
- Hamann DJ, Bezboruah KC. Utilization of technology by long-term care providers: Comparisons between for-profit and nonprofit institutions. J Aging Health 25(4):535–54. 2013.
- Moss AJ, Harris-Kojetin LD, Sengupta M, et al. Design and operation of the 2010 National Survey of Residential Care Facilities [PDF 2.10 MB]. Vital Health Stat 1(54). 2011.
- SAS, release 9.2 [computer software]. Cary, NC: SAS Institute. 2008.
- SUDAAN, release 10.0 [computer software]. Research Triangle Park, NC: RTI International. 2008.
Suggested citation
Caffrey C, Park-Lee E. Use of electronic health records in residential care communities. NCHS data brief, no 128. Hyattsville, MD: National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., Acting Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: September 10, 2013
- Content source: