

Emergency Department Visits Related to Schizophrenia Among Adults Aged 18–64: United States, 2009–2011
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- Data from the National Hospital Ambulatory Medical Care Survey, 2009–2011
- Did ED visit rates related to schizophrenia vary by age and sex?
- Did the patient’s place of residence differ for those with ED visits related to schizophrenia compared with other ED visits?
- What was the most common primary expected source of payment for ED visits related to schizophrenia? Did this differ from other ED visits?
- What percentage of ED visits related to schizophrenia led to a hospitalization or a transfer to another hospital? Did this differ from ED visits not related to schizophrenia?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 215, September 2015
PDF Version (738 KB)
Michael Albert, M.D., M.P.H.; and Linda F. McCaig, M.P.H.
Key findings
Data from the National Hospital Ambulatory Medical Care Survey, 2009–2011
- During 2009–2011, an estimated 382,000 emergency department (ED) visits related to schizophrenia occurred each year among adults aged 18–64, with an overall ED visit rate of 20.1 per 10,000 adults.
- The overall rate for ED visits related to schizophrenia for men (26.5 per 10,000) was approximately double the rate for women (13.8 per 10,000).
- Public insurance (Medicaid, Medicare, or dual Medicare and Medicaid) was used more frequently at ED visits related to schizophrenia compared with ED visits not related to schizophrenia.
- About one-half of ED visits related to schizophrenia led to either a hospital admission (32.7%) or a transfer to a psychiatric hospital (16.7%); these percentages were higher than for ED visits not related to schizophrenia.
Schizophrenia is a severe brain disorder with clinical manifestations that may include hallucinations, delusions, and thought and movement disorders (1,2). This report describes the rate and characteristics of emergency department (ED) visits related to schizophrenia among adults aged 18–64. Visits with an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) code of 295 for any of the up to three diagnoses listed as being related to the visit were included in this analysis to broadly describe ED visits related to schizophrenia (3).
Keywords: mental health, health care utilization, National Hospital Ambulatory Medical Care Survey
Did ED visit rates related to schizophrenia vary by age and sex?
- During 2009–2011, an estimated 382,000 ED visits related to schizophrenia occurred each year among adults aged 18–64. The overall visit rate for this age group was 20.1 per 10,000 adults (Figure 1).
- The overall rate for ED visits related to schizophrenia for men (26.5 per 10,000) was approximately double the rate for women (13.8 per 10,000). Rates were higher for men compared with women for all age groups, except 50–64.
- The overall visit rates were higher among persons aged 30–39 and 40–49 compared with those aged 18–29. Beyond ages 40–49, the rate declined, with the rate for adults aged 50–64 similar to the rate for those aged 18–29.
- The visit rate for men declined after ages 40–49. The observed lower visit rates for both men and women aged 18–29 compared with those aged 30–39 and 40–49 did not reach statistical significance.
Figure 1. Schizophrenia-related emergency department visit rates for adults aged 18–64, by age and sex: United States, 2009–2011

1Visit rate is significantly different (p < 0.05) for men compared with women of the same age group, based on a two-tailed t test.
2Visit rate is significantly different (p < 0.05) compared with all persons aged 18–29, based on a two-tailed t test.
3Visit rate is significantly different (p < 0.05) compared with men aged 50–64, based on a two-tailed t test.
4Visit rate is significantly different (p < 0.05) compared with all persons aged 50–64, based on a two-tailed t test.
NOTES: Figure is based on 3-year averages. Emergency department visits related to schizophrenia are defined as code 295 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the up to three collected visit diagnoses. Data are based on a sample of 551 emergency department visits related to schizophrenia made during 2009–2011, representing an average weighted total of 382,000 visits per year. Visit rates are based on the set of estimates of the civilian noninstitutionalized population of the United States, as developed by the U.S. Census Bureau’s Population Division.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2009–2011.
Did the patient’s place of residence differ for those with ED visits related to schizophrenia compared with other ED visits?
- ED visits related to schizophrenia were less frequently made by patients living in a private residence (69.2%) than ED visits not related to schizophrenia (92.3%) (Figure 2).
- A total of 7.5% of ED visits related to schizophrenia were made by homeless persons compared with 0.9% of ED visits not related to schizophrenia.
- ED visits related to schizophrenia were more frequently made by patients living in an “other” type of residence (17.2%) than ED visits not related to schizophrenia (1.9%). This category included nursing homes, psychiatric hospitals, group homes for the mentally or physically disabled, assisted-living centers, prisons, hotels, and college dormitories.
Figure 2. Patient residence for emergency department visits made by adults aged 18–64, by schizophrenia diagnosis: United States, 2009–2011
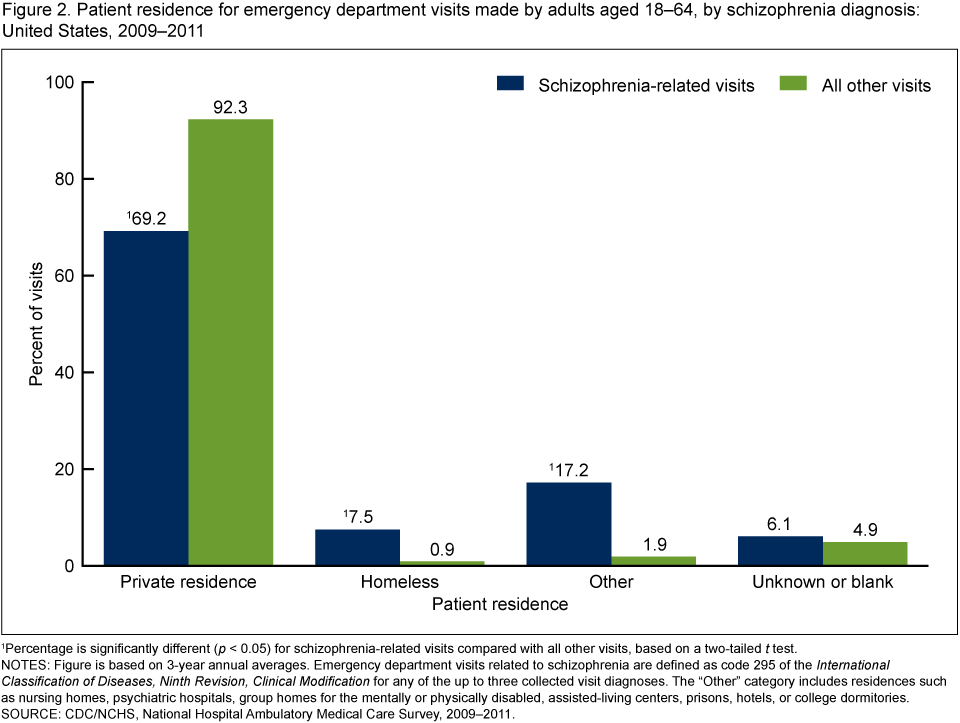
1Percentage is significantly different (p < 0.05) for schizophrenia-related visits compared with all other visits, based on a two-tailed t test.
NOTES: Figure is based on 3-year annual averages. Emergency department visits related to schizophrenia are defined as code 295 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the up to three collected visit diagnoses. The “Other” category includes residences such as nursing homes, psychiatric hospitals, group homes for the mentally or physically disabled, assisted-living centers, prisons, hotels, or college dormitories.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2009–2011.
What was the most common primary expected source of payment for ED visits related to schizophrenia? Did this differ from other ED visits?
- The most common primary expected source of payment for ED visits related to schizophrenia by adults aged 18–64 was Medicaid (40.2%). This percentage was higher compared with ED visits not related to schizophrenia (23.2%) (Figure 3).
- ED visits related to schizophrenia more frequently had dual Medicare and Medicaid (14.5%) or Medicare (15.0%) as the primary expected source of payment than ED visits not related to schizophrenia (3.5% and 5.2%, respectively).
- The number of visits related to schizophrenia with a primary expected source of payment of private insurance was too small to make a reliable estimate. By contrast, 34.3% of visits not related to schizophrenia had private insurance as the primary expected payment source.
Figure 3. Primary expected source of payment for emergency department visits made by adults aged 18–64, by schizophrenia diagnosis: United States, 2009–2011

* Figure does not meet standards of reliability or precision.
1Percentage is significantly different (p < 0.05) for schizophrenia-related visits compared with all other visits, based on a two-tailed t test.
NOTES: Figure is based on 3-year annual averages. Emergency department visits related to schizophrenia are defined as code 295 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the up to three collected visit diagnoses. Medicaid includes the Children’s Health Insurance Program. “Other or unknown” includes workers’ compensation, other source of payment, and unknown or blank.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2009–2011.
What percentage of ED visits related to schizophrenia led to a hospitalization or a transfer to another hospital? Did this differ from ED visits not related to schizophrenia?
- The percentage of ED visits related to schizophrenia that resulted in a hospital admission (32.7%) was higher compared with ED visits not related to schizophrenia (10.3%)
(Figure 4). - An additional 16.7% of ED visits related to schizophrenia resulted in a transfer to a psychiatric hospital. This was higher than the percentage of ED visits not related to schizophrenia (0.7%).
Figure 4. Selected dispositions of emergency department visits made by adults aged 18–64, by schizophrenia diagnosis: United States, 2009–2011
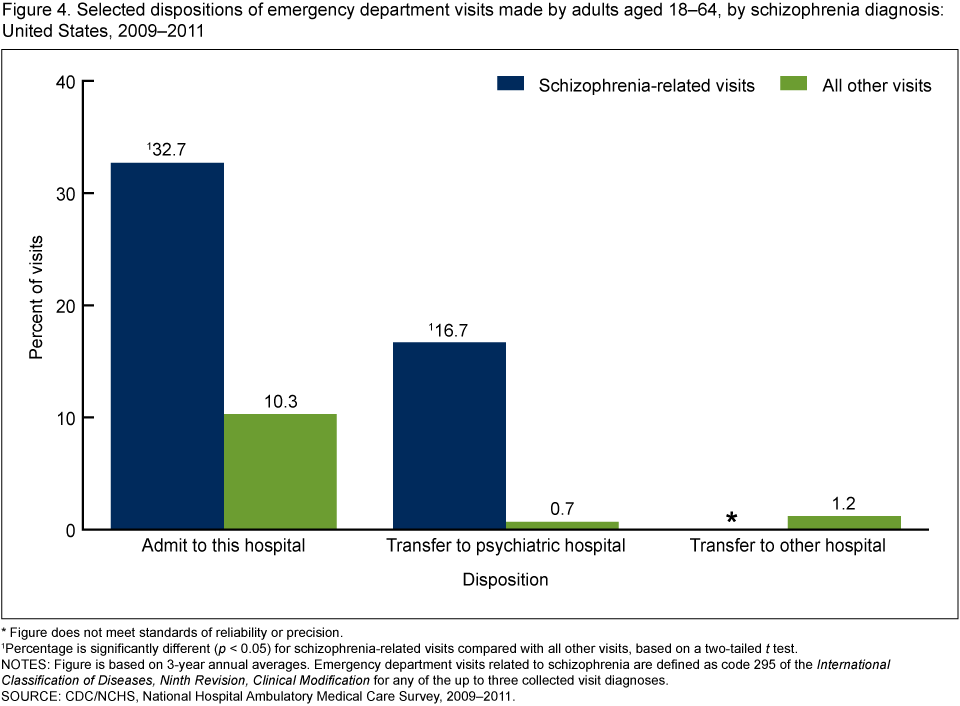
* Figure does not meet standards of reliability or precision.
1Percentage is significantly different (p < 0.05) for schizophrenia-related visits compared with all other visits, based on a two-tailed t test.
NOTES: Figure is based on 3-year annual averages. Emergency department visits related to schizophrenia are defined as code 295 of the International Classification of Diseases, Ninth Revision, Clinical Modification for any of the up to three collected visit diagnoses.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2009–2011.
Summary
ED care is important for the treatment of acute presentations of schizophrenia and may serve as a safety net for schizophrenic patients not otherwise receiving care (4,5). This analysis of National Hospital Ambulatory Medical Care Survey (NHAMCS) data indicates that during 2009–2011, an average of 382,000 ED visits related to schizophrenia occurred each year among adults aged 18–64, corresponding to an overall visit rate of 20.1 per 10,000 adults. A visit having a first-, second-, or third-listed diagnosis of schizophrenia (i.e., whether the visit was directly or indirectly related to schizophrenia) was included in the analysis to provide a broader description of ED use by these patients. The distribution of the primary diagnosis of visits related to schizophrenia was: schizophrenia (58.8%), another mental disorder (15.4%), and a nonmental health disorder (25.7%) (data not shown).
Among adults aged 18–64, the rate for ED visits related to schizophrenia was about twice as high for men as for women. Public insurance (Medicaid, Medicare, or dual Medicare and Medicaid) was more frequently the primary expected source of payment for ED visits related to schizophrenia compared with ED visits not related to schizophrenia. ED visits related to schizophrenia were more frequently made by patients who were homeless compared with ED visits not related to schizophrenia. About one-third of ED visits related to schizophrenia resulted in a hospital admission, and another 16.7% resulted in a transfer to a psychiatric hospital—both higher than the percentages for ED visits not related to schizophrenia.
One of the goals of Healthy People 2020 is to improve mental health through prevention and by ensuring access to appropriate, quality mental health services (6). National data on the rates and characteristics of ED visits related to schizophrenia will help policymakers and practitioners address disparities and meet this goal.
Definitions
Medicaid: Visits with Medicaid as the expected payment source included those covered by a Medicaid-sponsored prepaid plan, and for those under age 19, may have included charges covered under the Children’s Health Insurance Program.
No insurance: A visit having self-pay, no charge, or charity as the expected payment source.
Primary expected source of payment: More than one source of expected payment may have been reported per visit. The primary expected source of payment was determined using the following hierarchy: dual Medicare and Medicaid, Medicare, Medicaid, private insurance, workers’ compensation, self-pay, no charge or charity, other, and unknown.
Visit related to schizophrenia: A visit having a first-, second-, or third-listed diagnosis of code 295 using the ICD–9–CM coding system (3). Up to three diagnoses related to each ED visit are collected, including chronic conditions.
Data source and methods
Data are from the 2009–2011 NHAMCS, a nationally representative survey of nonfederal, general, and short-stay hospitals that is conducted annually by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics. NHAMCS uses a multistage probability design with samples of geographic primary sampling units (PSUs), hospitals within PSUs, and patient visits within EDs. Data were collected on approximately 35,000 ED visits in both 2009 and 2010, and 31,000 visits in 2011. More details about the design of NHAMCS are available online (7,8).
The analysis was restricted to visits by patients aged 18–64 because of the small number of visits related to schizophrenia by patients outside of this age range. Data were imputed for patient birth year and sex. The category “Other” for patient residence in Figure 3 included the options of “Nursing home” and “Other residence.” Other residence could include a psychiatric hospital, group home for the mentally or physically disabled, assisted-living center, prison, hotel, or college dormitory. A small number of visits (less than 1%) were listed as having more than one of the dispositions shown in Figure 4, and these visits were excluded from the analysis for that figure.
Data analyses were performed using the statistical packages SAS, version 9.3 (SAS Institute, Cary, N.C.) and SAS-callable SUDAAN, version 11.0 (RTI International, Research Triangle Park, N.C.). Differences among subgroups were evaluated using a two-tailed t test ( p < 0.05). Estimates based on fewer than 30 sample records are not presented.
About the authors
Michael Albert and Linda F. McCaig are with CDC’s National Center for Health Statistics, Division of Health Care Statistics.
References
- Substance Abuse and Mental Health Services Administration. Mental disorders.
- National Institute of Mental Health. Health & education: Schizophrenia.
- Centers for Disease Control and Prevention, National Center for Health Statistics. Centers for Medicare & Medicaid Services. International classification of diseases, ninth revision, clinical modification, 6th ed. DHHS Pub No. (PHS) 06–1260. 2006.
- Marco CA, Vaughan J. Emergency management of agitation in schizophrenia. Am J Emerg Med 23(6):767–76. 2005.
- Mojtabai R, Cullen B, Everett A, Nugent KL, Sawa A, Sharifi V, et al. Reasons for not seeking general medical care among individuals with serious mental illness. Psychiatr Serv 65(6):818–21. 2014.
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020 topics and objectives: Mental health and mental disorders. Washington, DC.
- National Center for Health Statistics. 2010 NHAMCS micro-data file documentation. 2010.
- National Center for Health Statistics. 2009 NHAMCS micro-data file documentation. 2009.
Suggested citation
Albert M, McCaig LF. Emergency department visits related to schizophrenia among adults aged 18–64: United States, 2009–2011. NCHS data brief, no 215. Hyattsville, MD: National Center for Health Statistics. 2015.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: September 23, 2015
- Content source: