

Access and Utilization of Selected Preventive Health Services Among Adolescents Aged 10–17
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- How has adolescents’ preventive health care service utilization changed over time in the United States?
- Does the utilization of preventive care services change over the course of adolescence?
- Are race and ethnicity, poverty status, and insurance coverage status related to having a usual place for preventive care for adolescents?
- Are race and ethnicity, poverty status, and insurance coverage status related to having a well-child checkup in the past 12 months for adolescents?
- Are race and ethnicity, poverty status, and insurance coverage status related to having a dental visit in the past 12 months for adolescents?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 246, May 2016
PDF Version (353 KB)
Lindsey I. Black, M.P.H.; Colleen N. Nugent, Ph.D.; and Anjel Vahratian, Ph.D.
Key findings
Data from the National Health Interview Survey
- The percentages of adolescents aged 10–17 who did not have a usual place for preventive care, did not receive a well-child checkup in the past 12 months, or did not have a dental visit in the past 12 months decreased from 2008 to 2014.
- In 2014, 2% of adolescents aged 10–17 did not have a usual place for preventive care, 21% did not receive a well-child checkup, and 12% did not have a dental visit in the past 12 months.
- In 2014, the percentages of adolescents not having a usual place for preventive care, not receiving a well-child checkup, and not having a dental visit were higher for those aged 16–17 compared with those in younger age groups. These percentages also varied by race and ethnicity, poverty status, and insurance status.
Adolescence is a critical period for health promotion, disease prevention, and the development of healthy habits (1). Regular preventive health care visits during this period are recommended to promote health and quality of life (2). This report examines recent trends and demographic differences in the percentages of adolescents with a usual place for preventive care; those who had a well-child checkup in the past 12 months; and those who had a dental visit in the past 12 months.
Keywords: teens, wellness, medical care, National Health Interview Survey
How has adolescents’ preventive health care service utilization changed over time in the United States?
From 2008 to 2014, the percentages of adolescents aged 10–17 who did not have a usual place for preventive care, did not receive a well-child checkup in the past 12 months, or did not visit the dentist in the past 12 months decreased (Figure 1). For all years, the percentage with no well-child checkup was higher than the percentage with no dental visits. Additionally, the percentage with no dental visits was higher than the percentage with no usual place for preventive care. The percentage of adolescents without a usual place for preventive care decreased from 4.5% in 2008 to 2.3% in 2014. A decrease was also observed in the percentage of adolescents who did not have a dental visit in the past 12 months, from 15.6% in 2008 to 12.1% in 2014. The highest percentage point difference was observed in the percentage of adolescents who did not receive a well-child checkup in the past 12 months, from 31.3% to 21.2% during the same time period.
Figure 1. Percentage of adolescents aged 10–17 who did not have a usual place for preventive care, did not receive a well-child checkup, or did not have a dental visit, by year: United States, 2008–2014

NOTES: Linear decrease from 2008 to 2014 is statistically significant at p < 0.05 level for all measures shown. All percentage differences by year and measure are statistically significant (p < 0.05). Access data table for Figure 1.
SOURCE: NCHS, National Health Interview Survey, 2008–2014.
Does the utilization of preventive care services change over the course of adolescence?
The percentage of adolescents who did not have a usual place for preventive care increased as age increased. About 1.4% of those aged 10–11, 1.7% of those 12–13, 2.7% of those 14–15, and 3.5% of those 16–17 did not have a usual place for preventive care in 2014 (Figure 2). The percentage of adolescents without a dental visit in the past 12 months also increased with advancing age, with 9.2% of those aged 10–11, 11.3% of those 12–13, 12.7% of those 14–15, and 15.3% of those 16–17 not having a dental visit in the past 12 months. The percentage of adolescents with no well-child checkup in the past 12 months was approximately the same for those aged 10–11 (20.3%) through 14–15 (19.2%), but was higher for adolescents aged 16–17 (27.1%).
Figure 2. Percentage of adolescents aged 10–17 who did not have a usual place for preventive care, did not receive a well-child checkup, or did not have a dental visit, by age group: United States, 2014

NOTES: Linear increase across age is statistically significant at p < 0.05 level for no usual place for preventive care and no dental visit, past 12 months. Quadratic trend is significant at p < 0.05 for no well-child checkup, past 12 months. Access data table for Figure 2.
SOURCE: NCHS, National Health Interview Survey, 2014.
Are race and ethnicity, poverty status, and insurance coverage status related to having a usual place for preventive care for adolescents?
Of the three race and ethnicity groups, Hispanic adolescents (4.2%) were more likely than both non-Hispanic white (1.5%) and non-Hispanic black (2.0%) adolescents to not have a usual place for preventive care (Figure 3). Adolescents with family income less than or equal to 138% of the federal poverty level (FPL) were more likely than those with income greater than 138% FPL to not have a usual place for preventive care. Uninsured adolescents (18.4%) were more likely to not have a usual place for preventive care compared with those having private (1.1%) or public (1.6%) health coverage.
Figure 3. Percentage of adolescents aged 10–17 who did not have a usual place for preventive care, by race and Hispanic origin, poverty status, and health insurance coverage: United States, 2014

1Significantly different from Hispanic adolescents.
2Significantly different from those with income greater than 138% FPL.
3Significantly different from uninsured adolescents.
NOTES: FPL is federal poverty level. Access data table for Figure 3.
SOURCE: NCHS, National Health Interview Survey, 2014.
Are race and ethnicity, poverty status, and insurance coverage status related to having a well-child checkup in the past 12 months for adolescents?
Of the three race and ethnicity groups, Hispanic adolescents (27.8%) were more likely than non-Hispanic white (19.7%) and non-Hispanic black (18.0%) adolescents to not receive a well-child checkup in the past 12 months (Figure 4). Adolescents with family income of 138% FPL or less (24.4%) were more likely to not receive a well-child checkup compared with those having family income greater than 138% FPL (19.8%). Adolescents who were uninsured were more likely to have not received a well-child checkup (54.2%), compared with those having private (18.8%) or public (19.4%) health coverage.
Figure 4. Percentage of adolescents aged 10–17 who did not receive a well-child checkup in the past 12 months, by race and Hispanic origin, poverty status, and health insurance coverage: United States, 2014

1Significantly different from Hispanic adolescents.
2Significantly different from those with income greater than 138% FPL.
3Significantly different from uninsured adolescents.
NOTES: FPL is federal poverty level. Access data table for Figure 4.
SOURCE: NCHS, National Health Interview Survey, 2014.
Are race and ethnicity, poverty status, and insurance coverage status related to having a dental visit in the past 12 months for adolescents?
Of the three race and ethnicity groups, a lower percentage of non-Hispanic white adolescents (9.5%) did not have a dental visit in the past 12 months, compared with non-Hispanic black (14.1%) and Hispanic (16.9%) adolescents (Figure 5). Those with family income of 138% FPL or less (19.1%) were more likely than those with family income greater than 138% FPL (9.1%) to have not visited the dentist in the past 12 months. Adolescents who were uninsured (41.7%) were the most likely to have not visited the dentist in the past 12 months, followed by those with public (15.6%) and private (7.3%) health coverage.
Figure 5. Percentage of adolescents aged 10–17 without a dental visit in the past 12 months, by race and Hispanic origin, poverty status, and health insurance coverage: United States, 2014
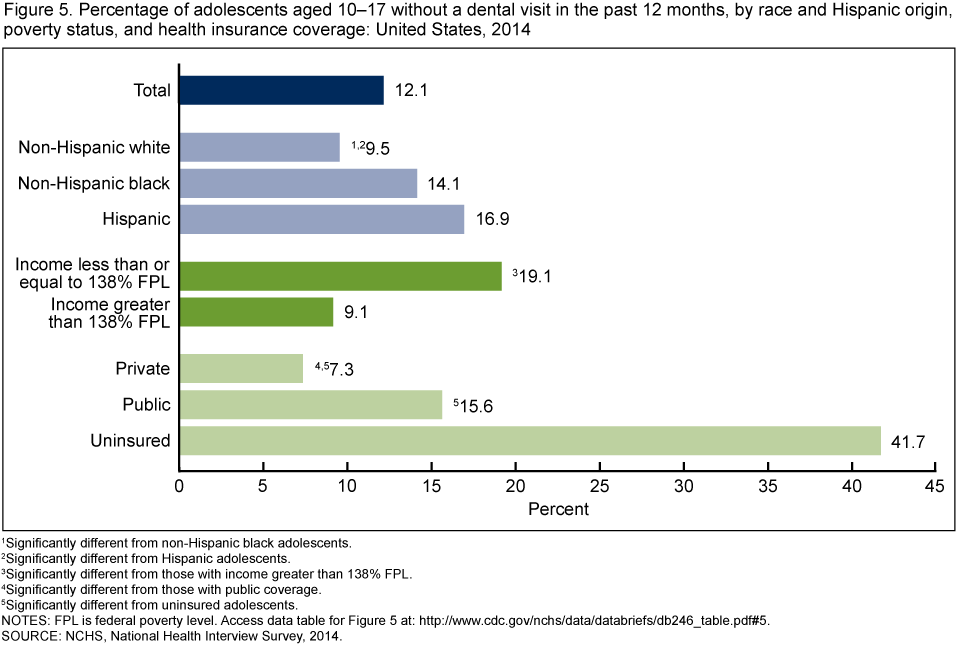
1Significantly different from non-Hispanic black adolescents.
2Significantly different from Hispanic adolescents.
3Significantly different from those with income greater than 138% FPL.
4Significantly different from those with public coverage.
5Significantly different from uninsured adolescents.
NOTES: FPL is federal poverty level. Access data table for Figure 5.
SOURCE: NCHS, National Health Interview Survey, 2014.
Summary
Overall, the percentages of adolescents aged 10–17 without a usual place for preventive care or who did not receive a well-child checkup or visit the dentist in the past 12 months have decreased since 2008. Access and utilization of these selected preventive care services declined with increasing age. Further, racial and socioeconomic disparities were seen in the populations that did not use these selected preventive care services. Adolescents who were Hispanic, poor, or uninsured consistently had higher rates of nonreceipt of preventive health care compared with those who were non-Hispanic white, non-Hispanic black, not poor, or with health care coverage. Because adolescence is a dynamic stage of human development, access to and utilization of preventive care is an important step in preparing adolescents for lifelong health and wellness as they transition from childhood to adulthood.
Definitions
Usual place for preventive care: Based on a series of survey questions that determine if there is a usual place of sick and preventive care and the type of places that are visited. Estimates presented are strictly based on responses to questions about the place the child usually goes to when he or she needs routine or preventive care, such as a physical examination or well-child checkup. Children whose usual place for preventive care was an emergency room were considered not to have a usual place for preventive care.
Well-child checkup: Based on the response to the survey question, “During the past 12 months did [sample child name] receive a well-child checkup—that is, a general checkup when [he/she] was not sick or injured?”
Dental visit: Based on the response to the survey question, “About how long has it been since [sample child name] last saw a dentist? Include all types of dentists, such as orthodontists, oral surgeons, and all other dental specialists, as well as dental hygienists.”
Health insurance coverage type: Based on the status of health insurance coverage at the time of interview. Private health insurance includes children with comprehensive private insurance plans obtained through a parent’s or caregiver’s employer, purchased directly, purchased through local or community programs, or purchased through the Health Insurance Marketplace or a state-based exchange. Public health insurance includes children with Medicaid, Children’s Health Insurance Program, or other state-sponsored health plan. Uninsured children includes those who were not reported to have been covered at the time of interview or those who were covered only by Indian Health Service or had only a single service plan (e.g., dental care only). Children with more than one type of health insurance were assigned to the first appropriate category in the following mutually exclusive hierarchy: private coverage, public coverage, other coverage (data not shown), or uninsured.
Data source and methods
Data from the 2008–2014 National Health Interview Survey (NHIS) were used for this analysis. NHIS is a nationally representative survey of the civilian noninstitutionalized U.S. population. It is conducted continuously throughout the year by the National Center for Health Statistics (NCHS). NHIS is an in-person interview conducted in the respondent’s home. In some instances, follow-up to complete the interview is via telephone. The survey consists of (a) a Family Core component, with questions asked about all members of the family; (b) a Sample Adult component, which collects additional information from one randomly selected adult per family; and (c) a Sample Child component, which collects additional information about one randomly selected child per family. Data for this analysis come from the Sample Child and Family Core components of NHIS. For more information, visit the NHIS website.
NHIS is designed to yield a nationally representative sample, and these analyses used weights to produce national estimates. The sample design is described in more detail elsewhere (3). Point estimates and the corresponding variances for this analysis were calculated using SUDAAN software (4) to account for the complex sample design of NHIS. The Taylor series linearization method was used for variance estimation. All estimates shown meet the NCHS standard for reliability (having a relative standard error less than or equal to 30%). Linear and quadratic trends were tested in SUDAAN PROC DESCRIPT using the POLY option. Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. All differences reported are significant unless stated otherwise.
For 2014, approximately 20% of NHIS respondents were missing data on family income and personal earnings. To analyze associations with poverty status, NHIS’ imputed personal earning and income files were used (5).
About the authors
Lindsey I. Black, Colleen N. Nugent, and Anjel Vahratian are with the National Center for Health Statistics, Division of Health Interview Statistics.
References
- National Research Council and Institute of Medicine: Committee on Adolescent Health Care Services and Models of Care for Treatment, Prevention, and Healthy Development. Adolescent health services: Missing opportunities. Washington, DC: National Academies Press. 2009.
- American Academy of Pediatrics. Recommendations for preventive pediatric health care. 2016.
- Parsons VL, Moriarity C, Jonas K, et al. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
- RTI International. SUDAAN (Release 11.0.0) [computer software]. 2012.
- Schenker N, Raghunathan TE, Chiu PL, et al. Multiple imputation of family income and personal earnings in the National Health Interview Survey: Methods and examples. National Center for Health Statistics. 2010.
Suggested citation
Black LI, Nugent CN, Vahratian A. Access and utilization of selected preventive health services among adolescents aged 10–17. NCHS data brief, no 246. Hyattsville, MD: National Center for Health Statistics. 2016.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Nathaniel Schenker, Ph.D., Deputy Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Interview Statistics
Marcie L. Cynamon, Director
Stephen J. Blumberg, Ph.D., Associate Director for Science
- Page last reviewed: May 10, 2016
- Page last updated: May 10, 2016
- Content source: