

Increases in Medically Attended Nonfatal Injury Episodes Among Females in the United States
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- From 2005–2008 to 2011–2014, the rate of medically attended nonfatal injury episodes among females increased 16%, while the rate for males did not change.
- The rate of medically attended nonfatal injury episodes among females aged 45–64 increased significantly from 2005–2008 to 2011–2014.
- From 2005–2008 to 2011–2014, the rate of medically attended nonfatal injury episodes among non-Hispanic white females increased.
- Among females, the nonfatal injury rates for major causes of injury did not change from 2005–2008 to 2011–2014.
- In both 2005–2008 and 2011–2014, the place where females were most frequently injured was inside the home.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 255, July 2016
PDF Version (171 KB)
Yahtyng Sheu, M.P.H., Ph.D., and Holly Hedegaard, M.D., M.S.P.H.
Key findings
Data from the National Health Interview Survey
- From 2005–2008 to 2011–2014, the nonfatal injury rate increased for females but remained unchanged for males.
- In 2005–2008, males had a higher nonfatal injury rate than females; however, in 2011–2014, the rates for males and females were similar.
- From 2005–2008 to 2011–2014, the nonfatal injury rate increased significantly for women aged 45–64 and for non-Hispanic white females.
- The increase in the nonfatal injury rate among females over time could not be attributed to a specific cause or place of injury occurrence.
Analysis of mortality and emergency department (ED) data have historically shown higher injury rates among males than females. In 2014, the injury-related death rate was 85.5 per 100,000 population for males and 36.3 for females (1). In 2013, 10,746 injury-related ED visits were made per 100,000 population for males and 8,957 for females (2). The National Health Interview Survey (NHIS) collects information on medically attended nonfatal injury episodes, providing national estimates beyond deaths and ED visits. This report describes changes in injury episodes in the female population, comparing estimates in 2005–2008 and 2011–2014 by age group, race and ethnicity, cause of injury, and location of injury.
Keyword: National Health Interview Survey
From 2005–2008 to 2011–2014, the rate of medically attended nonfatal injury episodes among females increased 16%, while the rate for males did not change.
- In 2005–2008, the age-adjusted injury rate was higher for males (121.3 episodes per 1,000 population) than for females (105.4) (Figure 1).
- From 2005–2008 to 2011–2014, the injury rate among females increased 16%, from 105.4 to 122.0 episodes per 1,000 population, while the rate among males did not change.
- The increase in the nonfatal injury rate among females in 2011–2014 resulted in a narrowing of the difference in rates between the sexes, with similar rates seen for males (126.5 episodes per 1,000 population) and females (122.0) in the later time period.
Figure 1. Age-adjusted rate of nonfatal injury episodes, by sex: United States,
2005–2008 and 2011–2014
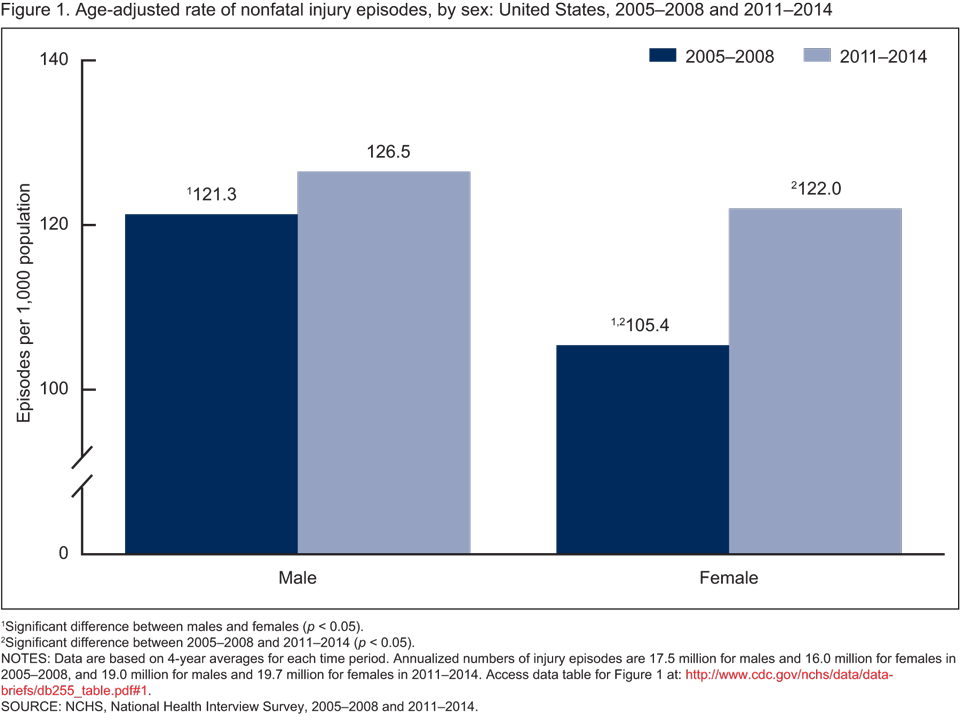
1Significant difference between males and females (p < 0.05).
2Significant difference between 2005–2008 and 2011–2014 (p < 0.05).
NOTES: Data are based on 4-year averages for each time period. Annualized numbers of injury episodes are 17.5 million for males and 16.0 million for females in 2005–2008, and 19.0 million for males and 19.7 million for females in 2011–2014. Access data table for Figure 1.
SOURCE: NCHS, National Health Interview Survey, 2005–2008 and 2011–2014.
The rate of medically attended nonfatal injury episodes among females aged 45–64 increased significantly from 2005–2008 to 2011–2014.
- Among all age groups, women aged 65 and over had the highest nonfatal injury rate in both 2005–2008 and 2011–2014 (151.6 and 163.7 episodes per 1,000 population, respectively) (Figure 2).
- From 2005–2008 to 2011–2014, a significant increase in the rate of injury episodes was observed for the 45–64 age group. For women aged 45–64, the rate increased 32%, from 103.4 episodes per 1,000 population in 2005–2008 to 136.4 in 2011–2014. The change in rates for other age groups was not statistically significant.
Figure 2. Rate of nonfatal injury episodes for females, by age group: United States,
2005–2008 and 2011–2014
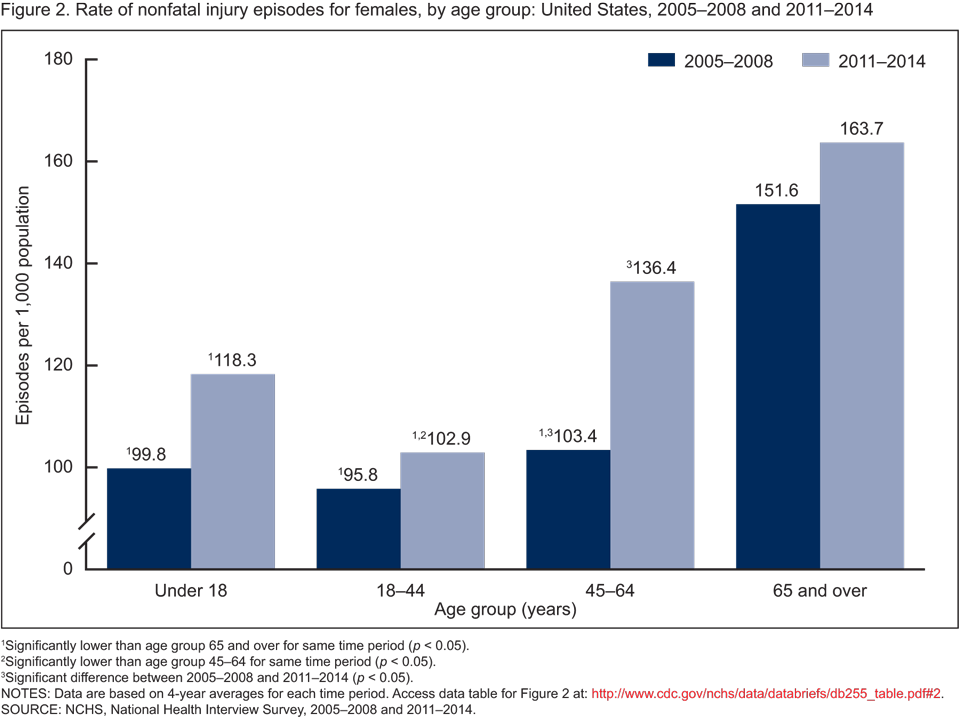
1Significantly lower than age group 65 and over for same time period (p < 0.05).
2Significantly lower than age group 45–64 for same time period (p < 0.05).
3Significant difference between 2005–2008 and 2011–2014 (p < 0.05).
NOTES: Data are based on 4-year averages for each time period. Access data table for Figure 2.
SOURCE: NCHS, National Health Interview Survey, 2005–2008 and 2011–2014.
From 2005–2008 to 2011–2014, the rate of medically attended nonfatal injury episodes among non-Hispanic white females increased.
- In 2005–2008, the age-adjusted nonfatal injury rate was highest among non-Hispanic white females (123.6 episodes per 1,000 population), while lower rates were observed for Hispanic and non-Hispanic black females (62.2 and 78.1 episodes per 1,000, respectively) (Figure 3).
- In 2011–2014, the rate continued to be highest among non-Hispanic white females (144.8 episodes per 1,000 population), however, the rate among non-Hispanic black females was significantly higher than the rate among Hispanic females.
- For both time periods, the injury rate among non-Hispanic white females was twice that of Hispanic females.
- From 2005–2008 to 2011–2014, increases in injury rates were observed for females of all race and ethnicity groups, however, the increase was significantly higher only for non-Hispanic white females (17% increase).
Figure 3. Age-adjusted rate of nonfatal injury episodes for females, by race and ethnicity: United States, 2005–2008 and 2011–2014
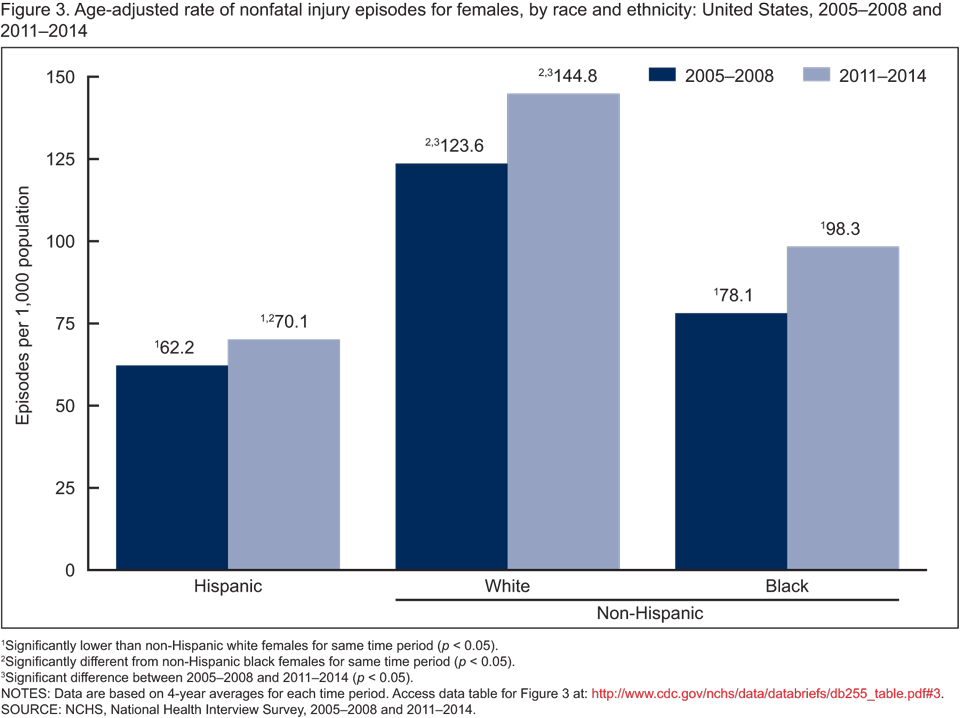
1Significantly lower than non-Hispanic white females for same time period (p < 0.05).
2Significantly different from non-Hispanic black females for same time period (p < 0.05).
3Significant difference between 2005–2008 and 2011–2014 (p < 0.05).
NOTES: Data are based on 4-year averages for each time period. Access data table for Figure 3.
SOURCE: NCHS, National Health Interview Survey, 2005–2008 and 2011–2014.
Among females, the nonfatal injury rates for major causes of injury did not change from 2005–2008 to 2011–2014.
- Falls were the leading cause of nonfatal injury among females in both 2005–2008 and 2011–2014. During both time periods, the rate of injury episodes from falls was approximately four times higher than the rates for causes such as being struck by or hitting against an object or person; injuries resulting from land, water, or air transportation; and overexertion (Figure 4).
- No significant changes were seen in injury rates from 2005–2008 to 2011–2014 for falls; being struck by or hitting against an object or person; injuries resulting from land, water, or air transportation; overexertion; cutting or piercing by sharp objects; and other specified injury causes (poisoning, fire and burn, animal and insect bites, and accidents from use of machinery).
Figure 4. Age-adjusted rate of nonfatal injury episodes for females, by cause of injury: United States, 2005–2008 and 2011–2014

1Significantly higher than all other causes for same time period (p < 0.05).
NOTES: Data are based on 4-year averages for each time period. Transportation includes injuries involving motor and nonmotor land transport vehicles, watercraft, or aircraft. Other specified includes poisoning, fire and burn, animal and insect bites, and accidents from use of machinery. Access data table for Figure 4.
SOURCE: NCHS, National Health Interview Survey, 2005–2008 and 2011–2014.
In both 2005–2008 and 2011–2014, the place where females were most frequently injured was inside the home.
- Inside the home was the leading place of nonfatal injury occurrence in both 2005–2008 (37.2% of injury episodes) and 2011–2014 (38.4%), followed by outside the home, street, recreation area, school, and commercial area (Figure 5).
- From 2005–2008 to 2011–2014, no significant change was seen in the distribution of place of injury occurrence among females.
Figure 5. Percent distribution of injury episodes among females, by place of occurrence: United States, 2005–2008 and 2011–2014
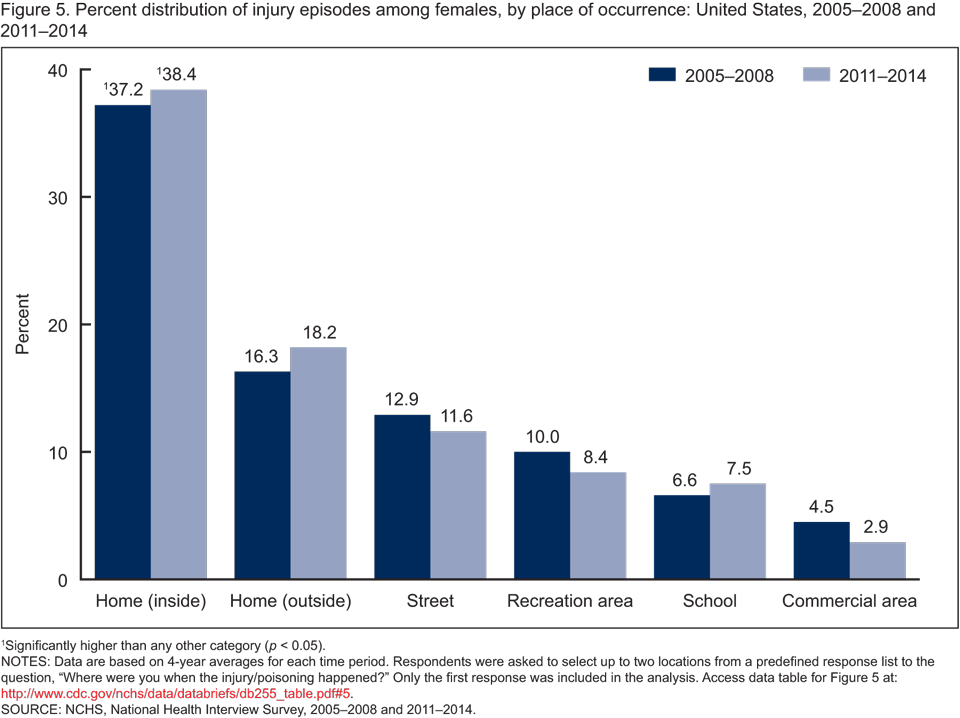
1Significantly higher than any other category (p < 0.05).
NOTES: Data are based on 4-year averages for each time period. Respondents were asked to select up to two locations from a predefined response list to the question, “Where were you when the injury/poisoning happened?” Only the first response was included in the analysis. Access data table for Figure 5.
SOURCE: NCHS, National Health Interview Survey, 2005–2008 and 2011–2014.
Summary
NHIS provides self- or proxy-reported information on medically attended injury episodes, including calls to medical care providers; treatment at the scene by emergency personnel; visits to a medical provider’s office, school nurse, or other clinic; ED visits; and hospitalizations. Unlike other sources of information on nonfatal injury episodes, such as data from EDs, the injury episodes reported in NHIS reflect all levels of injury severity.
Analysis of NHIS data shows a recent narrowing in the disparity in rates of nonfatal injury episodes among males and females. In 2005–2008, the age-adjusted nonfatal injury rate was higher among males than females. In contrast, during 2011–2014, the rate and number of nonfatal injury episodes for males and females did not differ. This change resulted from a 16% increase in the nonfatal injury rate among females, while the rate among males remained stable.
From 2005–2008 to 2011–2014, a significant increase in the nonfatal injury rate was seen among females aged 45–64 (32%) and non-Hispanic white females (17%). Injury rates for major causes such as falls; being struck by or hitting against an object or person; injuries resulting from land, water, or air transportation; overexertion; and cutting or piercing by sharp objects did not change. In addition, from 2005–2008 to 2011–2014, no change was seen in the distribution of injury episodes by place of injury.
Definitions
Cause of injury: The external force that resulted in physical or physiological harm. Examples of causes of injury include falling; being struck by or hitting against an object or person; injuries resulting from land, water, or air transportation; overexertion; cutting or piercing by sharp objects; fire and burn; animal or insect bite; and poisoning.
Injury episode: An event in which a person was 1) nonfatally injured from an external cause (e.g., a fall or a motor vehicle traffic accident), or 2) nonfatally poisoned from ingestion, inhalation, or contact with a harmful substance, including overdose or wrongful use of a drug or medication.
Medically attended: An injury episode for which a trained health care professional was contacted for advice or treatment. This advice or treatment may be given over the phone, at the scene or in an informal setting, or in a formal office setting, emergency department, or hospital. A trained health care professional includes such providers as a medical doctor, nurse, emergency medical technician, physical or occupational therapist, homoeopath, dentist, or specialist.
Data source and methods
Injury estimates in this report are based on NHIS data from 2005–2008 and 2011–2014. NHIS is a nationally representative, cross-sectional household interview survey that is fielded continuously by the National Center for Health Statistics (NCHS) and produces annual estimates of the health of the U.S. civilian noninstitutionalized population. Interviews are conducted in respondents’ homes, with occasional follow-up by telephone to complete an interview. Information on sample design and data weighting procedures can be found elsewhere (3).
Injury-related information is captured from questions in the Family Core section (4). These questions ask about medically attended nonfatal injuries that occurred for any family member within 3 months prior to the interview. For this analysis, a reference period of 5 weeks was used to provide national estimates, based on earlier findings demonstrating that a shorter reference period provided a better estimation of the annual total number for all injuries and for less severe injuries (5). An injury episode must have been assigned at least one International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) nature of injury code of 800–909.2, 909.9, 910–994.9, 995–995.59, or 998.80–995.85, and one external cause of injury code of E800–E848, E850–E869.9, E880–E929.9, or E950–E999.
NHIS is designed to provide national estimates by applying weights to a nationally representative sample. Point estimates and the corresponding variances for this analysis were calculated using SUDAAN software (6) to account for the complex sample design of NHIS. The Taylor series linearization method was used for variance estimation. All estimates shown meet the current NCHS standard for reliability (i.e., having a relative standard error less than or equal to 30%). Differences between percentages were evaluated using two-sided significance tests at the 0.05 level. All differences reported are statistically significant unless stated otherwise. All estimates are based on 4-year averages for each time period. In 2005–2008, a sample of 1,617 injury episodes for males and 1,563 injury episodes for females were included in the analysis. In 2011–2014, a sample of 2,438 injury episodes for males and 2,600 injury episodes for females were included in the analysis.
About the authors
Yahtyng Sheu and Holly Hedegaard are with the National Center for Health Statistics, Office of Analysis and Epidemiology.
References
- National Center for Health Statistics. CDC WONDER: About multiple cause of death, 1999–2014. 2015.
- National Center for Injury Prevention and Control. Injury prevention & control: Data & statistics (WISQARS).
- Parsons VL, Moriarity C, Jonas K, et al. Design and estimation for the National Health Interview Survey, 2006–2015. National Center for Health Statistics. Vital Health Stat 2(165). 2014.
- Chen LH, Warner M, Fingerhut L, Makuc D. Injury episodes and circumstances: National Health Interview Survey, 1997–2007. National Center for Health Statistics. Vital Health Stat 10(241). 2009.
- Warner M, Schenker N, Heinen MA, Fingerhut LA. The effects of recall on reporting injury and poisoning episodes in the National Health Interview Survey. Inj Prev 11(5):282–7. 2005.
- RTI International. SUDAAN (Release 11.0) [computer software]. 2009.
Suggested citation
Sheu Y, Hedegaard H. Increases in medically attended nonfatal injury episodes among females in the United States. NCHS data brief, no 255. Hyattsville, MD: National Center for Health Statistics. 2016.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Irma E. Arispe, Ph.D., Director
Makram Talih, Ph.D., Associate Director for Science
- Page last reviewed: July 14, 2016
- Page last updated: July 14, 2016
- Content source: