


Part-time Laborer Pinned Between Scissor Lift Work Platform Railing and Doorway Header - Virginia
 ShareCompartir
ShareCompartir
NIOSH In-house FACE Report 2003-01
April 15, 2004
Summary
On August 11, 2002, a 42-year-old part-time laborer (the victim) was killed when the scissor lift he was operating elevated and pinned him against the header of an interior doorway. The victim had been working during a weekend performing touch-up painting at a newly constructed day care center. Around midmorning, two coworkers left the jobsite while the victim continued to work alone, using a scissor lift to access the ceiling areas of the structure. Later, between 9:30 and 10:00 pm., one of the coworkers discovered the victim located on the scissor lift platform. The lift was positioned partway through an interior doorway with the platform elevated. [Photo 1] The victim was pinned between the top rail of the work platform and the head jamb of the doorway. The coworker exited the building and called 911 for assistance. Emergency medical service (EMS) personnel and local police responded and arrived at about 10:00 pm. The victim was pronounced dead at the scene. Later examination by the medical examiner’s office revealed that the victim had been dead for several hours.
NIOSH investigators concluded that to help prevent similar incidents, manufacturers of self-propelled elevating work platforms such as scissor lifts should:
- ensure that selector switches used to change the operating mode of single lever control systems are guarded against inadvertent activation;
- consider equipping them with audible alarms that provide different sounds for specific operational modes.
Employers should:
- ensure that workers are trained to recognize the hazards of operating self-propelled elevating work platforms in tight quarters;
- ensure that all equipment is inspected for defects by a competent person and maintained in proper working order, including the function of all safety devices and alarm systems.
And, equipment rental agencies should:
- ensure that machines are delivered to their customers in safe operating condition.
Introduction
On August 11, 2002, a 42-year-old part-time laborer was asphyxiated when the scissor lift he was operating elevated and pinned him against a doorway header. On August 28, 2002, the NIOSH Division of Safety Research (DSR) was notified of the incident by the Virginia Occupational Safety and Health (VOSH) Compliance Division. On October 8, 2002, a DSR Safety Engineer met with the VOSH Compliance Safety and Health Officer (CSHO) who investigated the case. The VOSH CSHO and the Safety Engineer met with staff of the rental agency who owned the scissor lift, and examined, tested, and photographed the machine.
The employer in this incident was the owner of a marine electrical company that had been in business for 20 years. The employer’s business provided engineering, design, prototyping and manufacturing of electronic-mechanical systems and marine devices. However, in this incident, the employer was acting as a construction general contractor to construct an addition to an existing school and day care center operated by a family member. Various subcontractors had been hired to erect the framework, install mechanical systems, and finish the interior of the addition. The victim and 3 other employees were active-duty military personnel who worked part-time for the employer as general laborers on weekends and during evenings, performing finish work such as touch up painting and hanging ceiling tiles. The victim had 1 year of experience with the employer. While serving in the military he had received safety training, but this did not include instruction for scissor lift operation. Hazard communication and safety training had not been provided by the employer. The victim often directed work when others were present.
This was the employer’s first fatality.
Back to Top
Investigation
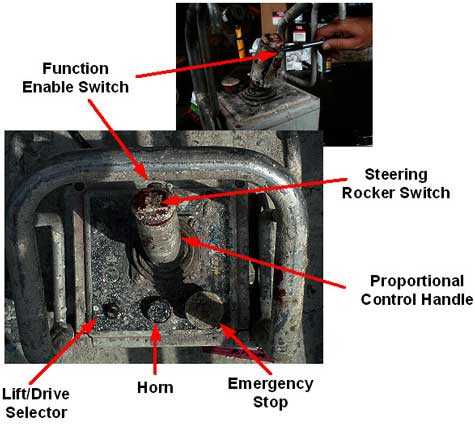
The scissor lift involved in the incident had been manufactured in 1998 and had 892 operational hours recorded on the hour meter. It was owned by an equipment rental company. The rental company’s maintenance records were incomplete regarding documentation of the machine’s condition as delivered. It had been delivered to the job site 2 months prior to the incident. The machine is 30 inches wide by 72 inches long and measures 74 inches from ground level to the top of platform rails when in the lowered position. [Photo 2] The maximum working height is 21 feet. Lift and drive operations are controlled by a control box connected to the machine by a 15-foot tether. The control box can be secured to a mount located on the right-side railing at the steering axle end of the work platform, hung over the platform rail, or used as a remote control from the ground. To drive the lift from place to place, the lift/drive function selector switch is moved to the drive position, the function enable paddle switch located on the proportional control handle is squeezed, and the control handle is pushed for forward motion, and pulled for rearward motion. [Photo 3] To elevate the work platform, the lift/drive function selector switch is moved to the lift position, the function enable paddle switch is squeezed, and the proportional control handle is pushed to elevate the platform and pulled to lower it. To steer left or right, the steering rocker switch on top of the proportional control is moved right or left to direct the wheels on the steering axle and the proportional control is used to drive forward or back. A set of ground operating controls is located on the side of the machine base. This set of controls contains the on/off switch for the machine, an emergency stop button, and platform elevation controls. No drive controls are located at this panel.
 |
|
Photo 2. Scissor lift in lowered position
|
On the day of the incident, the victim and a co-worker started work about 8:00 a.m. Work consisted of touch-up painting and hanging suspension wires for the installation of ceiling tiles. About mid-morning, the coworker left the job site for the day. Shortly before 10:30 a.m., another coworker, who had not been scheduled to work that day, stopped briefly to chat with the victim and then he also left. The victim remained on the job site and continued to touch-up the paint-work on the ceiling beams. Later that night, between 9:30 p.m. and 10:00 p.m. in response to telephone calls from the victim’s wife asking the whereabouts of her husband, one of the coworkers went to the site. He found the victim on the scissor lift platform caught between the upper platform railing and the head jamb of the doorway. The victim was slumped over the platform railing with his arms hanging down in front. The coworker exited the building and called 911 for assistance. EMS and police responded at 10:00 pm. The victim was pronounced dead at the scene. Later examination by the medical examiner’s office revealed that the victim had been dead for several hours.
 |
|
Photo 3. Control box operating switches
|
Although the event was un-witnessed, evidence collected by VOSH, the medical examiner’s office, and the police suggest that the incident occurred as the victim was moving the lift from one room to another. As he was maneuvering through a doorway, 40 ¼ inches wide by 83 inches high, the work platform elevated pinning the victim between the platform top rail and the doorway header. The lift/drive selector switch was found to be in the lift position. Police photos of the incident scene show the victim’s abdomen forced against the proportional control handle, pushing it fully forward, suggesting that the victim had been leaning forward over the platform railing while operating the proportional control by reaching his hand over and back through the railing between the top and mid-rail. The control box had been hung on the mid-rail. The forward most part of the scissor lift had just cleared the doorway. Considering the width of the doorway, the width of the lift, and the angle which the lift was driven through the doorway, there would have been only a few inches of clearance on each side. The victim may have been leaning forward and looking to the rear along the right side of the lift to observe this clearance. As the victim reached over the top rail and back through the mid-rail to grasp the proportional control, he may have inadvertently moved the lift/drive selector switch to lift position. Then, intending to drive through the doorway, he moved the proportional control forward. Instead of driving forward, the lift platform unexpectedly raised, pinning the victim and forcing his abdomen against the proportional control thus preventing him from moving the control back to lower the platform.
Back to Top
Cause of Death
The medical examiner’s official cause of death was mechanical asphyxiation.
Recommendations/Discussion
Recommendation 1: Manufacturers of self-propelled elevating work platforms should ensure that selector switches used to change the operating mode of single lever control systems are guarded against inadvertent activation.
Discussion: The control system for the lift involved in the incident used a single proportional control handle to control both drive and lift functions. A two-position toggle-type switch was used to select the desired function. When the selector switch was placed in the lift position, the proportional control handle was used to raise or lower the work platform. When the switch was placed in the drive position, the proportional control handle was used to move the machine forward and backward. After the incident, the lift/drive selector switch was found in the lift position. The lift/drive selector switch is located on the lower left quadrant of the control panel and enclosed under a weatherproof rubber boot when manufactured. However, the switch lever protrudes from the control panel unprotected. (Photo 4) It is possible that the victim inadvertently moved the selector switch from drive to lift mode when he reached through the platform rails to grasp the proportional control. Pulling the control forward, would then have raised the platform, pinning him against the head jamb of the doorway. It should be noted that the rubber boot had been damaged and/or removed from the switch in the incident. To protect against inadvertent activation of the selector switch, it could be enclosed in a switch guard or alternatively, the lift/drive mode could be selected by use of a recessed button or rocker switch.
 |
|
Photo 4.Unguarded lift/drive toggle switch
|
Recommendation #2: Manufacturers of self-propelled elevating work platforms should consider equipping them with audible alarms that provide different sounds for specific operational modes.
Discussion: The lift involved in this incident was equipped with an audible alarm system that sounded intermittent alarms of differing intervals depending on the operational mode of the lift. As observed during the investigation on October 8, 2002, the alarm provided an intermittent tone immediately prior to the lift being elevated. The same intermittent tone was sounded when the machine was in the drive mode immediately before moving. The investigator could discern no difference between the tone sounded before elevation and that sounded before driving. An alarm system that would provide a distinctly different sound immediately prior to the platform elevating, as opposed to the alarm that sounded before driving, may have alerted the victim to release the proportional control before he was pinned against the doorway header. It should be noted that immediately after the incident, when the lift was examined and tested by VOSH, none of the machine’s audible alarms were functioning.
Recommendation #3: Employers should ensure that workers are trained to recognize the hazards of operating self-propelled elevating work platforms in tight quarters.
Discussion: As previously noted, the clearance between the machine and the doorway was limited. Further, to access the room through the doorway while avoiding collision with a closet inside the room, the machine had to negotiate a tight turn from the hall way. There was just over 9 inches of clearance between the machine’s frame and the doorway, about 4 ½ inches on each side. [Photo 5] Also, when fully lowered, there would have been only 9 inches of clearance between the platform top rail and the head jamb of the doorway. Although the machine in question moves slowly, when clearances are tight, workers can be caught between structures or objects as a result of only minimal unexpected machine movement. OSHA regulation 29 CFR 1926.21 (b) (2) requires employers to instruct workers in recognition and avoidance of unsafe acts.* The circumstances surrounding this incident suggest that the victim may not have fully appreciated the risks of operating the machine in tight clearances. The machine’s control box was equipped with a 15-foot tether, making it possible for the operator to maneuver the machine while remaining on the ground, either in front of or behind the machine. In this case, it may have been safer to move the machine from place to place in that manner, although operation in this manner would not completely eliminate injury risks from tight clearances. Additionally, the police photographs show the victim’s knees covered by dust and debris from the platform, suggesting that he had been driving the machine while kneeling on the platform. Had he continued to operate in this manner or used the tethered control from the ground, the incident may not have occurred.
 |
|
Photo 5. Doorway to classroom from hall
|
Recommendation #4: Employers should ensure that all equipment is inspected for defects by a competent person and maintained in proper working order, including the function of all safety devices and alarm systems.
Discussion: Immediately after the incident, the machine was examined and tested by VOSH, and several functions and alarms were not working. None of the audible alarms were working and the platform controls were not operating as designed. When the proportional control lever was pushed forward the machine would intermittently fail to operate until the emergency stop button had been depressed and then reset. Further examination revealed moisture accumulations on the circuit boards inside of the control box. The control box weather seals, including the rubber boot around the proportional control lever, the boot over the lift/drive selector switch, and the rubber cover for the steering rocker switch had been compromised. After the moisture was removed, the controls operated correctly. Additionally, the machine had been used during spray painting operations and the control box was covered with paint overspray making the informational labels illegible and the indicator lights indiscernible. These conditions may not have had a direct impact on the incident; however, the general condition of the machine indicates a lack of appreciation for maintaining equipment in safe working condition. When workers are routinely using equipment and tools that need repair, it may be difficult for them to differentiate between workplace hazards that can be controlled through procedural intervention and those that can be controlled through proper equipment maintenance. Had the machine been inspected by a competent person with knowledge of correct scissor lift operation, the machine may have been removed from service until the malfunctions were corrected and the incident may not have occurred.
Recommendation #5: Equipment rental agencies should ensure that machines are delivered to their customers in safe operating condition.
Discussion: As previously mentioned, the maintenance records from the rental company were incomplete regarding documentation of the condition of the machine when it was delivered to the customer. It is possible that some of the malfunctions may have been present when the machine was delivered to the jobsite. This may have led the employees to believe that the machine’s operation was satisfactory. The American National Standards Institute has developed consensus standards addressing the safe operation of scissor lifts. ANSI/SIA A92.6-1999 Self-Propelled Elevating Work Platforms contains specific standards for owners and operators of scissor lifts addressing inspection, maintenance, safe operation, and record keeping. [ANSI/SIA 1999] Had the machine been inspected by a competent person with knowledge of correct scissor lift operation, the machine may have been removed from service until the malfunctions were corrected and the incident may not have occurred.
* Code of Federal Regulations. See CFR in references.
Back to Top
References
- CFR. Code of Federal regulations. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- ANSI/SIA [1999] American national standard: Self-propelled elevating work platforms. New York, NY: American National Standards Institute, Inc. ANSI/SIA A92.6-1999.
Investigator Information
This incident was investigated by Paul H. Moore, Safety Engineer, NIOSH, Division of Safety Research, Surveillance and Field Investigation Branch.
In-house Reports
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research