


Ranch Worker Killed by Pressurized Water Striking Eye
 ShareCompartir
ShareCompartir
Oregon Case Report: 06-OR-025
Summary
On July 4, 2006, a 42-year-old ranch hand was struck in the eye by a stream of pressurized water from an irrigation line, and died 5 days later. The ranch hand was working alone in a hay field, moving wheeled irrigation equipment. Pumped water reached the fields through 4-inch risers located every 30 feet in the field, connected to a 12 inch mainline underground. Each riser was equipped with a built-in shut-off plate that was opened by a removable valve with a crank handle. Following standard procedure, the ranch hand closed the valve and drained the supply line so the valve could be removed from the riser. When he began to remove the valve, the cap of the riser blew off and pressurized water struck him in the face. He was knocked unconscious and fell face down in a growing pool of water. The ranch manager saw the geyser from the ranch house and drove to the site to investigate. He discovered the ranch hand and pulled him from the pool of water. Emergency responders arrived in about 10 minutes. The victim was transported to a hospital, where he died in intensive care 5 days later. The explosion of water caused a severe penetrating injury of the eye and resulting brain injury.
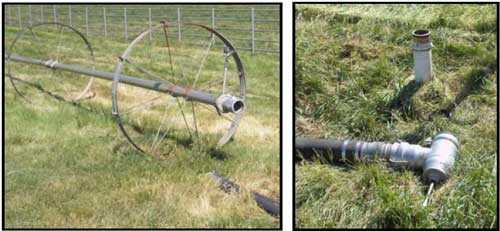 |
The irrigation wheel (left) connects to a heavy rubber supply line, which attaches to a removable valve (right foreground). The valve mounts over pressurized risers installed in the field, like the one shown here that failed (right background). |
Recommendations:
- When working with a pressurized irrigation system, stay clear or guard yourself from the outlet path where valves and hoses connect.
- Components of a pressurized irrigation system should be inspected for defective parts at least annually.
- Employers should establish an emergency plan for personnel who work alone.
Back to Top
Introduction
On July 4, 2006, a 42-year-old experienced ranch hand was fatally injured after being struck in the face and right eye by a geyser of water from an irrigation system. OR-FACE was notified of the incident the next day. OR-FACE did not make a site visit. This report is based on interviews with the employer by an OR-FACE investigator, and Oregon OSHA and Medical Examiner reports.
The employer is a large Oregon manufacturer and supplier of ready-mixed concrete, asphalt and paving, and aggregate materials. The firm is also a construction contractor, including excavation and site development services, building-material sales, and equipment rentals. The nonunion firm has been in business since 1993, and employs about 380 workers.
The firm has a full-time safety manager and a comprehensive safety program in the manufacturing, construction, and building-materials divisions, including regular safety meetings and training, lockout/tagout, and hazard communication.
The employer also employs eight workers at a horse and hay ranch, where this incident occurred. The ranch hand was of Hispanic ethnicity, spoke English and Spanish fluently, and served as interpreter to the Spanish speaking household workers at the ranch. He worked at other ranches previously, and had worked for 2 years with this employer. He was experienced with irrigation equipment, horse care, maintenance, and landscaping. He was working alone in the hay field at the time of the incident, moving irrigation equipment.
Back to Top
Investigation
The ranch's irrigation system had been installed in several stages before the ranch was purchased by the employer in 1985. The system was equipped with a 12-inch mainline buried underground, with multiple 4-inch risers installed about 30 feet apart in the field. Water pressure of 80 psi at the pump fed the mainline continuously, charging the risers in multiple fields at once. Each riser was equipped with a built in shut-off plate that was opened by a removable valve with a crank handle. The elbow valve connected the riser to a heavy rubber supply line that led to an irrigation wheel. The riser where the incident occurred was about one-quarter mile from the pump house, and pressure on the line there was estimated to be about 60 psi.
On the morning of the incident, the ranch hand was working alone in a hay field, moving an irrigation wheel line to the next riser. Following standard procedure, he shut off the valve on the riser and disconnected the heavy rubber supply line from the irrigation wheel to drain the hose. He then released the bottom clamp that connected the valve to the riser. At that moment, the cap of the riser blew out, releasing a 4 inch column of pressurized water. The geyser struck the ranch hand in the face and right eye, causing multiple lacerations, and severing an artery in the eye. The victim was knocked unconscious by the blow and fell face down in a growing pool of water.
The ranch manager, seeing the water geyser in the hay field from the ranch house, drove to the site and discovered the victim, and pulled him from the water. He called 911 and administered first-aid. Emergency responders arrived in about 10 minutes. The victim was transported by helicopter to a hospital, where he died in intensive care 5 days later.
Following the incident, the entire irrigation system was immediately shut down and inspected. Examination of the riser shut-off cap showed heavy corrosion on the inside anchor nut, threaded stem, and metal retainer. The metal retainer had broken, allowing the stem to slip free and release the cap.
Two years prior to this incident, a riser cap had failed and resulted in a similar explosion of water. In that case, the threads of the stem were apparently stripped from being tightened excessively with a wrench. Field workers had been in the practice of tightening the riser caps to seal leaks. Subsequently, to avoid a similar occurrence, workers stopped carrying wrenches to repair leaks. Instead, the pump was shut down, pressure released from the system, and the riser cap removed to fix the leak. Leaks were generally caused by bad gaskets, stripped stem threads, bent or broken anchor nuts, or corrosion.
All riser caps on the ranch were opened and inspected for corrosion following this incident. Those with slack in the anchor nut or corroded elements were replaced.
 |
The corroded stem from the riser (middle), displayed in perspective with the connecting valve, shows the anchor nut screwed up tight under the shut-off plate, indicating the riser was closed when the incident occurred. The corroded retainer inside the riser failed (right). |
Cause of Death
Intracranial trauma
Recommendations/Discussion
Recommendation #1: When working with a pressurized irrigation system, stay clear or guard yourself from the outlet path where valves and hoses connect.
Serious injuries from pressurized irrigation systems are rare, but fittings on pressurized lines of various kinds are known to occasionally fail catastrophically. On machinery, manufacturing standards have developed to place guards around hydraulic fittings and generally position them away from the active work area. In an irrigation system, built-in guards may not be feasible, and workers are regularly exposed to pressurized valves. Personal protective equipment such as impact-resistant safety glasses could be used while working with irrigation valves. In any circumstances, this incident emphasizes the importance of keeping your head clear of the outlet path of the pressurized water in case a failure should occur.
Recommendation #2: Components of a pressurized irrigation system should be inspected for defective parts at least annually.
Components in an irrigation valve are subject to corrosion and pressure damage. Defects in a stem, nut or retainer that result in a leak, can also result in an explosion as in this instance. The timing of this incident suggests a final twist or pull when a person is working on the system can trigger the failure. Employers should consider performing scheduled inspections and preventive maintenance on depressurized irrigation systems at least annually.
Recommendation #3: Employers should establish an emergency plan for workers who work alone.
The geyser in this incident happened to provide a signal for a rapid response. Employers should consider a means of communication for any lone worker to use in case of emergency. A check-in system can help to keep track of an employee's location and any unaccountable absence. Supervisors and others should be trained in first-aid, and know who to call in an emergency and how to direct responders to the site in a remote location.
Prearranged signals, accountability, first-aid skills, and emergency contacts can make a vital difference in rapid response, especially for those who work alone. OSHA rules prohibit working alone only in certain jobs - when exposed to harmful atmospheres, chemicals, electricity, fire, and in logging operations.
Back to Top
References
- Coble, D.S. (2004). Almost everyone needs a working alone policy. Industrial Safety & Hygiene News (Sep 1); 63, 65.
- NURSE Project. (1992). Irrigator struck in face by pipe valve. California Department of Health Services. Available online: http://www.nasdonline.org/document/257/d000061/irrigator-struck-in-face-by-pipe-valve.html (Link updated 10/5/2009)
- Hansen, H. & Trimmer, W. (1996). Irrigation System Walk-through Inspection Analysis. Pacific Northwest Extension - Oregon, Washington, Idaho. Available online: http://extension.oregonstate.edu/catalog/pdf/pnw/pnw293.pdf (Link no longer available 3/26/2013)
Oregon FACE Program
CROET at OHSU performs OR-FACE investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research. The goal of these evaluations is to prevent fatal work injuries in the future by studying the work environment, the worker, the task, the tools, the fatal energy exchange, and the role of management in controlling how these factors interact.
To contact Oregon State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
Oregon FACE reports are for information, research, or occupational injury control only. Safety and health practices may have changed since the investigation was conducted and the report was completed. Persons needing regulatory compliance information should consult the appropriate regulatory agency.
Back to Top
Oregon Case Reports- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research