


Temporary Mill Worker Killed in Fall Down Manlift Shaft
 ShareCompartir
ShareCompartir
Oregon Case Report: 07OR057
Summary
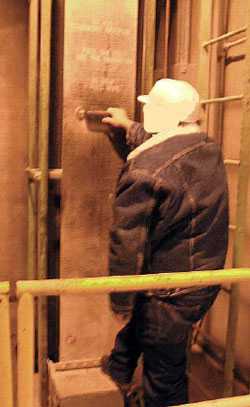 |
A worker at the mill demonstrates use of the manlift to ride between floors. |
On December 21, 2007, a 56-year-old clean-up worker at a food mill was killed when he fell into a manlift shaft. The worker apparently tripped or misjudged the handhold on a continuously running manlift in the mill that carried workers up and down between floors. He fell through the 2x2½-foot floor opening onto a crossbeam and was struck continuously by one of the manlift steps, which was unable to pass by him. The worker was employed through a temporary agency and was on the job 2 weeks. He was a native Spanish speaker with very limited proficiency in English, which made communication difficult. The victim had a visual impairment, which may have been a contributing factor in the fall.
Recommendations
- Workers must follow safe procedures when using a manlift.
- Employers must ensure workers understand safe procedures and demonstrate competence using a manlift, and are physically capable to use a manlift safely.
- Employers should have the capacity to train and supervise foreign-born workers in a language they understand.
- Employers should update manlift equipment to meet current safety standards.
- Employers must ensure landing surfaces for manlifts are clear and provide safe footing.
Introduction
On December 21, 2007, a 56-year-old temporary worker was killed when he fell down a manlift shaft at an animal-feed processing plant. OR-FACE received notification the same day. This report is based on a site visit and interview with the employer by an OR-FACE investigator, and information from Oregon OSHA, police, and medical examiner reports.
The feed processing plant was one of 65 plants in a national agriculture and dairy cooperative firm. The Oregon plant had been in operation for 35 years, and was purchased by the cooperative about 5 years earlier. The plant employed 14 workers (10 in plant, 4 in administration), working in two shifts. Raw feed material, such as corn, was delivered by rail and augured into bins on the second floor of the plant. The feed was then ground and blended with other food pellets and grains, and dumped into tanker trucks or bagged for shipping.
 |
A close-up view of a platform step on the manlift shows the metal framework on the left and emergency ladder on the right. |
A temporary hiring agency was used by the firm to provide workers at its two Oregon locations. The temporary agency trained workers with an orientation video on basic safety requirements and a test. The plants provided specific on-the-job training. The safety training provided to temporary workers at the plant in this incident involved instructions on how to operate the manlift. All job instruction and safety training at the agency and the plant were in English.
The plant followed corporate safety programs, held monthly safety meetings, and performed regular safety inspections. Toolbox safety meetings were held periodically. All workers were provided with personal protective equipment. Temporary workers, hired as cleaners (sweeping, shoveling, picking up litter), were given on-the-job training.
The company had a written safety program for the manlift and elevator at the plant, consisting of procedures, inspections, and training. Orientation included the manlift manufacturer’s safety video. Manlift safety instructions specified that no freight or handheld tools were allowed while riding the lift.
The foreign-born worker in this incident and a friend were hired together by a temporary agency to work as cleaners at the feed processing plant. The men were both native Spanish speakers. They received on-the-job training at the plant from their supervisor in English. Although the Spanish-speaking cleaner had very limited proficiency in English, he had lived and worked in the USA for 30 years, and was comfortable managing tasks in an English-speaking environment. He had a physical impairment, a “slow” eye that impaired his ability to focus, which may have been a contributing factor in this incident.
Investigation
On the day of the incident, the cleaner had worked at the plant less than 30 days. He arrived at 6 a.m. for the day shift and was assigned to sweep in the basement, where he had worked his previous shift. Two other workers were in the plant at the time.
For an unknown reason, the cleaner went to the second floor, and about 10 minutes later a crashing noise in the manlift was heard by a coworker. The cleaner had fallen down the manlift shaft and was dangling from one of the crossbeams about 8 feet below the second-floor opening. A broom that fell into the shaft with the cleaner lodged against the beams and prevented him from falling farther. A fixed platform step on the continuously moving manlift belt struck him on the back of the head, and was unable to pass. The belt slipped on the drive wheels.
 |
The victim fell through this manlift shaft opening. A platform step is shown on the lift belt, and the fixed ladder and stop cord at left. |
A coworker climbed the ladder in the manlift shaft and located the victim on the down side. Another coworker stopped the manlift and called for emergency assistance. Rescue workers found the victim dead at the scene.
Workers used the manlift to move up and down between floors. The 15.5-inch-wide manlift belt ran in a continuous loop from the basement through holes in the first and second floors, then through a roof housing; one side up and one side down. Platform steps were attached to the belt every 11½ feet, with hand grips halfway between the steps. The floor openings were roughly circular, about 2x2½ feet in diameter. A fixed ladder ascended the shaft, and a stop cord was installed next to the belt, which could be grabbed to pull in the direction of the lift to stop.
Gates guarded the manlift floor openings. Floor surfaces were not always clear and secure. On the second floor, where the incident occurred, bolt heads protruded one-half inch from the floor about 10 feet from the down shaft. On the third floor, a raised plywood floor around the shaft was spongy when walked upon.
 |
A gate guarded the manlift floor openings. At one opening, a raised plywood floor was spongy when walked upon, reducing secure footing. |
Safety instructions on the belt and on the wall near the first-floor access shaft were in English only, and partially obscured due to wear. Although each floor was well lit, the environment was dusty and the shaft openings were unlit.
This event was unwitnessed. The Oregon OSHA investigator suggested two possible scenarios.
- The cleaner may have tripped on the way to the access shaft down, and fallen with his head over the hole; a descending step then struck and pulled him down the shaft. A fracture on the right side of his face above the right eye indicates he may have been knocked unconscious.
- The cleaner may have misjudged the handhold while stepping onto the downside manlift, causing him to fall.
Back to Top
Cause of Death
Recommendations/Discussion
Recommendation #1. Workers must follow safe procedures when using a manlift.
Manlifts are for people only. Materials or equipment must not be transported on a manlift. Although the details in this event are uncertain, the broom may have contributed to the fall. The worker evidently brought the broom with him inside the gate surrounding the manlift shaft, and it could have caused a tripping hazard near the moving belt.
Recommendation #2. Employers must ensure workers understand safe procedures and demonstrate competence using a manlift, and are physically capable to use a manlift safely.
Employers are required to provide safety training to employees in hazardous work settings, and must verify that employees have acquired the knowledge and skills to work safely. Competence-based training involves verbal teaching and written materials, demonstration, and practice under supervision. New workers should be closely supervised, and retraining conducted to correct poor performance. Firms using temporary employees are responsible for specific safety training at the worksite. Temporary staffing agencies are responsible for general safety training.
In this incident, particular concern is raised by the worker’s visual impairment, with a “slow” eye that prevented him from focusing his vision. The National Safety Council has recommended that workers who use manlifts should be given physical examinations to confirm fitness. Poor depth perception or other physical issues could increase the risk of using a manlift. Workers found medically unfit should not be allowed to use a manlift.
Recommendation #3. Employers should have the capacity to train and supervise foreign-born workers in a language they understand.
In this incident, though the worker demonstrated competence using the manlift following initial on-the-job training, safe procedures may not have been adequately communicated or reinforced, due to a language barrier. All training as well as posted safety messages at the manlift were in English. In general, employers are required to present safety training information in a manner that their employees can understand, tailored to the employees' language and education. Different regulations apply for different settings (as reviewed in an OSHA policy memo, available online at www.osha.gov/dep/standards-policy-statement-memo-04-28-10.html). This incident emphasizes, however, that training materials in Spanish, by themselves, may not be enough. Employers should develop the capacity to supervise and communicate with workers in their own language. Direct communication could have allowed the supervisor to probe the effect of the worker’s visual impairment and provided the worker an opportunity for interactive questions.
Recommendation #4. Employers should update manlift equipment to meet current safety standards.
The manlift in this incident was installed 25 years earlier and did not meet all current Oregon OSHA safety requirements. Manlifts in some grain silos and mills may be so old that OSHA requirements do not apply. Employers with older manlifts should contact an OSHA office to consult with a safety officer. All new manlift installations and equipment must meet design requirements of the American National Safety Standard for Manlifts (ANSI A90.1 – updated 2009), which is incorporated in OSHA regulations (29 CFR 1910.68). Specifications apply to the diameter of the floor holes, belt width, emergency landings, ladders, and so on. Among the issues in this instance, the floor openings were smaller than the minimum required for the width of the manlift belt. For a 16-inch-wide belt, floor openings must be 36-40 inches in diameter and circular. Smaller openings can prove fatal if the manlift is used by a worker wearing gear, such as a firefighter.
Recommendation #5. Employers must ensure landing surfaces for manlifts are clear and provide safe footing.
Exposed bolt heads protruding one-half inch above the floor in the area of the second-floor manlift shaft presented a tripping hazard that may have been a factor in this incident. On another floor, an elevated, spongy plywood floor with a ramp to the manlift shaft also presented a tripping hazard. This incident emphasizes the importance of making sure the floor area around a manlift shaft is flat and solid, and clear of obstructions.
References
Brooks, Jr., R. (2003). Lost in the translation: Not being able to read a warning sign at a construction site or telltale on a piece of machinery can have deadly consequences. Occupational Health and Safety Magazine. Available online: http://ohsonline.com/articles/2003/12/lost-in-the-translation.aspx (Link Updated 10/31/11)
CROETWeb: Safety, Language and Culture. Online safety resource: www.croetweb.com/links.cfm?topicID=73&langID=2
National Institute for Occupational Safety and Health. (2008). NIOSH Science Blog: Contingent Workers. Available online: www.cdc.gov/niosh/blog/nsb021908_contworker.html
NIOSH Fire Fighter Fatality Investigation and Prevention Program. (2006). Career fire fighter killed while riding manlift to assess a silo fire – Missouri. Available online: www.cdc.gov/niosh/fire/reports/face200534.html
Occupational Safety & Health Administration. Compliance Assistance Quick Start: Hispanic Outreach. Online safety resource: www.osha.gov/dcsp/compliance_assistance/quickstarts/hispanic/index_hispanic.html
Oklahoma FACE. An elevator operator was killed when he fell from a manlift (04-OK-058-01). Available online: www.cdc.gov/niosh/face/stateface/ok/04ok058.html
Oregon OSHA. Division 4F: Manlifts [based on U.S. OSHA, 29 CFR 1910.68]. Available online: www.cbs.state.or.us/external/osha/pdf/rules/division_4/div4f.pdf
Oregon OSHA. Occupational Safety & Health Program in Spanish. Online safety resource: www.cbs.state.or.us/external/osha/educate/peso.html
Key Words: Falls, Manufacturing, Hispanic
Oregon FACE Program
OR-FACE/CROET L606
Oregon Health & Science University
3181 SW Sam Jackson Park Rd.
Portland OR 97239-3098
Phone 503-494-2281
Email: orface@ohsu.edu
Website: www.ohsu.edu/xd/research/centers-institutes/croet/outreach/or-face/ (Link updated 8/14/2012)
Oregon Fatality Assessment and Control Evaluation (OR-FACE) is a project of the Center for Research on Occupational and Environmental Toxicology (CROET) at Oregon Health & Science University (OHSU). OR-FACE is supported by a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (2U60/OH008472-06), through the Occupational Public Health Program (OPHP), Oregon Public Health Division.
OR–FACE reports are for information, research, or occupational injury control only. Safety and health practices may have changed since the investigation was conducted and the report was completed. Persons needing regulatory compliance information should consult the appropriate regulatory agency.
To contact Oregon State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research