


High-Rise Apartment Fire Claims the Life of One Career Fire Fighter (Captain) and Injures Another Career Fire Fighter (Captain) - Texas
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2001-33 Date Released: October 21, 2002
SUMMARY
On October 13, 2001, a 40-year-old Captain (the victim) died and another Captain was injured while fighting a fifth floor high-rise apartment fire. At 0448 hours, units were dispatched to a fire alarm. Units arrived on the scene at 0453 hours and reported heavy fire showing from the exterior of the building. Crews made immediate entry and attack, but after running low on air the victim and the other Captain decided to exit. In the process, the victim apparently became disoriented and lost, whereas the other Captain was able to escape. Rescue crews were sent to the fifth floor where the victim was located in the elevator common area. The victim was transported to an area hospital where he was pronounced dead at 0615 hours. NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should
ensure that the department's high-rise Standard Operating Procedures (SOPs) are followed and refresher training is provided
ensure that team continuity is maintained
ensure that personnel are in position to maintain an offensive attack
ensure that a lifeline is in place to guide fire fighters to an emergency stairwell
instruct and train fire fighters on initiating emergency traffic (Mayday-Mayday) when they become lost, disoriented, or trapped
ensure that a Rapid Intervention Team (RIT) is established and in position
ensure that a backup line is manned and in position to protect exit routes
ensure that adequate numbers of staff are available to immediately respond to emergency incidents
ensure that the Incident Commander (IC) continuously evaluates the present weather conditions (i.e., high winds) during high-rise fire operations
Additionally,
fire departments should establish and enforce standard operating procedures on the use of thermal imaging cameras for search-and-rescue operations
the authority having jurisdiction shall ensure that the receipt and processing of alarms is completed in a timely manner

Building Involved in Fire
INTRODUCTION
On October 13, 2001, a 40-year-old Captain (victim) died and another Captain (Captain #1) was injured while fighting a high-rise apartment fire. The National Institute for Occupational Safety and Health (NIOSH) was notified of this incident by the U.S. Fire Administration (USFA) on October 16, 2001. On October 22, 2001, three Safety and Occupational Health Specialists and the Section Chief from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. Meetings were conducted with the Chief, Assistant Chiefs, a District Chief, the department's training officer, representatives of the City Fire and Arson Bureau, representatives of the International Association of Fire Fighters, and a representative from the Texas State Association of Fire Fighters. Interviews were conducted with officers and fire fighters involved in this incident. NIOSH investigators reviewed the fire department's standard operating procedures (SOPs) for high-rise fire fighting, the fire department's prefire plans for this building, witness statements, site diagrams, building floor plans and records, a National Climatic Data Center weather report for the time and area of the incident, dispatch tape transcripts, the medical examiner's report, and the victim's training records. A site visit was conducted and the incident site photographed.
The victim's SCBA was sent to the NIOSH Respirator Branch in Morgantown, West Virginia, for further evaluation. The purpose of the testing was to determine the SCBA's conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to determine conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition. Seven performance tests were run, and the unit met the requirements of all tests except for the Remaining Service Indicator Test, where the Vibralert indicator activated prematurely. Even though the respirator failed this test, NIOSH investigators do not believe it was a contributing factor to this incident. (A summary of this report is included as Appendix I.)
A follow-up visit was conducted on March 12, 2002, to interview additional officers and fire fighters involved in this incident. On April 12, 2002, a phone interview was conducted with the officer of Engine 11.
The career department involved in this incident is comprised of 3400 uniformed fire fighters. The department serves a population of approximately 1.8 million residents in a geographic area of about 618 square miles.
Training and Experience. The department requires all new fire fighters to complete 640 hours of fire fighter training and 240 hours of emergency medical technician training before they are assigned to a station. All new fire fighters are required to complete a 12-month probationary period. The victim was a Captain who had approximately 20 years of experience with the department.
Equipment.
0448 Hours-Initial Dispatch (first alarm)
District Chief 28 (incident commander [IC]), District Chief 6 (lobby sector), District Chief 5, Engine 2 (Captain [victim], fire fighter, engineer/operator), Engine 28 (Captain, two fire fighters, engineer/operator), Engine 3 (Captain, two fire fighters, engineer/operator), Engine 38 (Captain, fire fighter, engineer/operator), Engine 11 (Captain, fire fighter, engineer/operator), Ladder 28 (Captain [Captain #1], fire fighter, engineer/operator), Ladder 38 (Captain, fire fighter, engineer/ operator), Ladder 301 (Captain, fire fighter, engineer/operator), Safety Officer 2, Safety Officer 15, and Ambulance 28 (two paramedics).
0456 Hours (second alarm)
District Chief 69, District Chief 21, District Chief 10, Engine 16 (Captain, fire fighter, engineer/ operator), Engine 60 (Captain, two fire fighters, engineer/operator), Engine 37 (Captain, fire fighter, engineer/operator), Engine 51 (Captain, fire fighter, engineer/operator), Ladder 16 (Captain, fire fighter, engineer/operator), Ladder 51 (Captain, fire fighter, engineer/operator), Ladder 69 (Captain, fire fighter, engineer/operator), Cascade 2 (engineer/operator), Rehab 17 (engineer/operator), and Rescue 11 (Captain, two fire fighters, engineer/operator).
Additional units were dispatched on subsequent alarms; however, only those units directly involved in the fatal event are discussed in the investigation section of this report.
Structure. The incident site is a high-rise apartment building that was built in 1980. There are 41 stories above grade and 1 story below grade (Photo 1). The first floor consists of a main lobby area, service facilities, conference rooms, and office space (Diagram 1). Storage units are located on the second floor. Floors 3 through 15 contain 8 apartment units each (Diagram 2). The remaining floors have four apartment units each. All floors are served by four passenger elevators and two service elevators. Two stairwells ("B" stairwell [top and bottom are pressurized] and "C" stairwell [top only is pressurized]) open to the roof and to the ground level on the C-side of the building (Diagram 1). Standpipe outlets are located in each of the two stairwells. Neither stairwell has communication capabilities. All common areas are sprinklered, but not individual apartments. NOTE: This incident occurred in a city where automatic sprinkler systems were not required in this building when it was issued a building permit in 1980. Requirements for mandatory sprinklering of high-rise buildings were required for all new high-rises permitted after 1981. Automatic sprinklers are now required throughout the entire building in all new high-rise buildings.
Weather. The National Weather Service reported that the winds at the regional airport shifted to a North-Northwest direction when a line of thunderstorms hit the area between 0300 and 0400 hours. The winds diminished after 0400 hours with wind speeds of approximately 7 knots, and a wind direction coming from the North. The wind speeds increased, with gusts exceeding 17 knots (19 mph), after 0500 hours when a front passed through the area.
Fire Model. Upon a request from NIOSH, the National Institute of Standards and Technology (NIST) completed a fire model of a similar incident. The fire model demonstrates growth and the fire's reaction when different variables are introduced. The complete fire model will be available for viewing online in the near future at http://www.fire.nist.gov.
INVESTIGATION
At 0448 hours, units were dispatched to a high-rise apartment building for a reported fire alarm. At 0452 hours, Central Dispatch notified responding units that multiple calls had been received confirming a fire on the fifth floor. At 0453 hours, Engine 2 arrived on the scene and reported to Central Dispatch that they had heavy fire showing from the exterior of the building (Photo 2). The victim instructed the Dispatcher to "go ahead and give him a second alarm." NOTE: The second alarm was dispatched at 0456 hours. The victim, a fire fighter, and the engineer/operator from Engine 2 entered the main lobby and met with the security guard. NOTE: The victim and Fire Fighter #1 had on their full ensemble of turn-out gear and SCBAs, while the engineer/operator was in his station uniform. The security guard informed the crew that the fire was on the fifth floor. The security guard led the Engine 2 crew to the fifth floor via the B-stairwell (Diagram 1 and 2). The victim searched for the apartment where the fire was located while the fire fighter and engineer/operator connected 100 feet of 1¾-inch hoseline to the hose cabinet (Diagram 2 and Photo 3).
At 0454 hours, District Chief 28 (DC 28) arrived on the scene, assumed command (incident commander [IC]), and established an incident command post on the A-side of the building. The IC ordered the Engine 28 Captain to establish lobby sector. The Captain met the building security guard in the lobby and secured the elevator keys (Diagram 1). A Captain (Captain #1) and fire fighter from Ladder 28 proceeded in the elevator to the fourth floor after being informed by the security guard that civilians were trapped in apartment 5052 on the fifth floor. NOTE: They took the elevator to the fourth floor to give themselves an opportunity to become familiar with the common area floor layout. Lobby sector informed the crew of Engine 3 that the fire was on the third floor. NOTE: From the exterior of the building, the fire reportedly appeared to be on the third floor. This conflicted with the initial reports given to Central Dispatch by the building residents, who reported that the fire was on the fifth floor. This led to confusion as to which floor the backup crews should respond to. Lobby sector ordered a fire fighter from his crew (Engine 28) to assist the Engine 3 crew (assigned to be the backup crew on the fire floor (fifth floor)). At 0459 hours, District Chief 6 (DC 6) arrived on the scene and assumed lobby sector. The Engine 28 Captain informed DC 6 that Engine 2, Engine 3, and Ladder 28 were on the fire floor. He then informed him that the elevators were not working properly and crews were using the stairwells to reach the fire floor. DC 6 ordered Engine 38 and Ladder 38 to proceed to the floor above the fire floor. The IC advised Central Dispatch that they had confirmation of a civilian trapped on the fire floor.
At 0501 hours, the victim advised command that they were on the fire floor (fifth), had laid a hoseline, and would lay another. Note: At approximately this time a weather front was passing through the region with wind speeds increasing and gusts exceeding 17 knots (19 mph). At 0502 hours, the victim radioed command asking for a second company. The IC replied that Engine 3 should be there backing him up. Note: The Engine 3 crew had taken the elevator to the second floor (believing that the third floor was the fire floor) and were unable to locate either of the two stairwells. Only storage units are located on the second floor. The Engine 3 crew located and assisted a civilian to the elevator and down to the lobby. At 0503 hours, the victim advised command that he was trying to conduct a primary search of apartments (other than the apartment where the fire was located) and that he was waiting for backup before entering the fire apartment (Diagram 2 and 3).
At 0505 hours, the Captain (Captain #1) from Ladder 28 and his fire fighter (Fire Fighter #2) reached the fifth floor and met with the victim and Fire Fighter #1. Fire Fighter #2 informed Captain #1 that he had forgotten the thermal imaging camera (TIC). Fire Fighter #2 went to the stairwell and asked the engineer/operator from Engine 2 to retrieve the TIC. Note: The Engine 2 engineer/operator was unable to return to the fifth floor because he was not wearing any personal protective equipment or a self-contained breathing apparatus (SCBA). The engineer/operator had passed the TIC to another fire fighter on the second floor landing but the TIC did not make it to Captain #1. Fire Fighter #2 then returned and remained at the entrance to the fire apartment.
The victim, Fire Fighter #1, and Captain #1 made entry into the fire apartment. They encountered heavy black smoke as they entered the apartment. Fire Fighter #1 manned the nozzle, preceding the victim and Captain #1 on the hose line. They made their way toward the kitchen area before turning and seeing fire emitting from the foyer area (Diagram 3). Fire Fighter #1 opened the nozzle and began knocking down the fire in the foyer area with Captain #1, the victim, and Fire Fighter #2 (in the apartment doorway) backing him up. While attempting to locate the seat of the fire, Fire Fighter #1 informed his Captain (the victim) that he was low on air and had to leave. Fire Fighter #1 passed the nozzle to Captain #1 and exited the apartment with Fire Fighter #2. Approximately 2 minutes later, the victim informed Captain #1 that they needed to leave because he was running low on air. The victim and Captain #1 followed the hoseline down the hallway toward the emergency stairwell (Photo 3). The victim told Captain #1 that they were going the wrong way. NOTE: The hose was laid throughout the common area near the elevators in large loops and was piled in the hallway (Diagram 2 and 3). Intense heat and zero visibility at the opposite end of the hallway from the fire apartment may have made it appear to the victim that they had gotten turned around and were heading back toward the apartment and not the emergency stairwell. Captain #1 informed the victim that they were near the hose cabinet and were heading toward the emergency stairwell. The victim, who was following Captain #1, turned and headed in the opposite direction (toward the fire apartment). NOTE: Captain #1 sustained burns to his wrist and lower back before reaching the emergency stairwell. At 0509 hours, the victim radioed, "Emergency, we need help on the fifth floor." Central Dispatch advised command that they had a call for help on the fifth floor. At 0510 hours, the victim radioed, "Engine 2, we're trapped on the fifth floor. Engine 2, help." The IC radioed lobby sector asking if they had received Engine 2's message. Lobby sector confirmed that they had received the message and requested additional companies for the rescue. At 0512 hours, Central Dispatch notified all companies that they had a Mayday on the fifth floor and toned out a third alarm. At 0512 hours, the victim radioed, "Engine 2, we're trapped on the fifth floor". NOTE: The third alarm dispatched, at 0512 hours, four Engines, two Ladder Trucks, one District Chief, one Shift Commander, and one Cascade Unit. At 0513 hours the victim made his final radio transmission, "Engine 2, emergency, we're....(the rest of the transmission was unintelligible)."
The IC ordered all second alarm companies to report to lobby sector. NOTE: A fourth alarm was also dispatched at 0512 hours. At 0527 hours, the IC reported that all fire fighters were accounted for except the Captain (the victim) on Engine 2. Crew members from Engine 60 and Rescue 11 made it to the fifth floor to search for the victim. A tag line was tied off to the door leading into the hallway. A thermal imaging camera was found in the hallway by the Captain of Rescue 11, but when he attempted to use it, the screen went completely white. The Captain and a fire fighter from Rescue 11 then heard the victim's personal alert safety system (PASS) device sounding. They located the victim in the common area near the elevators (Diagram 3). The victim did not have his helmet or face mask on when the Rescue 11 crew members reached him. The crew members checked for a pulse (a pulse was not detected) and noted that the victim was not breathing. They immediately began to move the victim down the hallway toward the B-stairwell. Engine 60 crew members assisted in bringing the victim down the hallway. Additional fire fighters had now reached the fifth floor and were assisting in the removal of the victim. As the victim was being moved from the hallway into the stairwell, two fire fighters from Rescue 11 became separated from their crew. The two fire fighters crawled into the service elevator area, and after running low on air, radioed command that they were trapped. The two fire fighters were able to locate a floor plan posted near the service elevator, and after determining the floor layout, they entered the stairwell and exited the building (Diagram 2 and Diagram 3).
At 0536 hours, rescue crews brought the victim down to the ground floor and out to the C-side of the building (Diagram 1). Fire fighters began cardiopulmonary resuscitation (CPR) efforts on the victim. The victim was transported in Ambulance 2 to an area hospital where he was pronounced dead at 0615 hours.
The operation went to a defensive mode from 0613 hours to 0638 hours. Crews then made an offensive attack with the fire being brought under control by 0730 hours.
CAUSE OF DEATH
The death certificate lists the cause of death as asphyxia due to a lack of oxygen. The victim's blood level of carboxyhemoglobin measured 18% saturation.
RECOMMENDATIONS / DISCUSSION
Recommendation #1: Fire departments should ensure that the department's high-rise Standard Operating Procedures (SOPs) are followed and refresher training is provided. 1
Discussion: It is imperative that companies perform their duties as described in the high-rise Standard Operating Procedures (SOPs) unless directed or approved by the Incident Commander to do otherwise. According to the SOPs of the department involved in this incident, the following procedures should take place upon arrival of the first-alarm companies:
An Investigative Team (first Engine Company and first Ladder Company dispatched) would provide a situation report. A second alarm would be called if fire or smoke is visible from the outside of the building. Some basic information such as the location of the fire, any serious life hazards, to what extent an evacuation has been implemented, and the status of the elevator system must be provided to additional personnel arriving on the scene. The investigative team would try to obtain a master key for stairwell doors and individual rooms. While on the second floor below the fire floor, the investigative team would check the suitability of that floor as a resource pool floor. The responsibilities of the investigative team are (1) identify the extent of the fire (2) identify which stairwell offers the best access for fire attack (3) communicate this information to the Incident Commander and (4) control the situation on the fire floor.
The Lobby Sector (second Engine Company dispatched) would take control of the fire control center (FCC). The Lobby Sector would then be able to communicate over the public address system with the building occupants and monitor the alarm locations on the alarm panel. Lobby Sector would act as the Access Sector Officer recording all companies entering and exiting the elevators and stairwells.
The Backup Crew (third Engine Company dispatched) would proceed to the fire floor to assist.
The Floor Above Crew (fourth Engine Company and second Ladder Company dispatched) would proceed as a team to the floor above the fire. The team would bring extra air bottles and leave them two floors below the fire floor (future resource pool) before advancing to the floor above the fire to check for fire extension, report their findings to the Incident Commander, and control the situation.
The Top Control Sector (third Ladder Company dispatched) would advance to the roof if a clear purpose and objective has been identified by command. One possible task of the Top Control Sector is the completion of vertical ventilation.
The Rapid Intervention Team (RIT) (fifth Engine Company dispatched) would consist of a minimum of three, preferably four members. The RIT would proceed to two floors below the fire floor with at least one extra air bottle per member, one extra self-contained breathing apparatus, appropriate forcible entry tools, high-rise attack line with nozzle, and a RIT kit.
Recommendation #2: Fire departments should ensure that team continuity is maintained. 2, 3
Discussion: Team continuity relies on some very important key factors: knowing who is on your team and the team leader, staying within visual contact at all times (if visibility is obscured then teams should remain within touch or voice distance of each other), communicating your needs and observations to the team leader, rotating to rehab and staging as a team, and watching your team members (practice a strong "buddy-care" approach). These key factors help to reduce serious injury or even death resulting from the risks involved in fire fighting operations by providing personnel with the added safety net of fellow team members. As teams enter a hazardous environment together, they should leave together to ensure that team continuity is maintained.
Recommendation #3: Fire departments should ensure that personnel are in position to maintain an offensive attack. 2, 4, 5, 6
Discussion: Childress [pp. 571-572] states that "if the arriving units have adequate resources to handle the situation, then they will fight the fire aggressively and offensively. They will attack the problem head-on and, following department standards, will accomplish their objectives efficiently, effectively, and safely. If they do not have adequate resources to aggressively handle the situation, then they will have to fight the fire in a defensive mode of attack. This mode will continue until enough resources can be massed to then change to an aggressive, offensive attack." Dunn [p. 138] states that "Before forcing open a door to an apartment in a high-rise residence first size up the hall. Observe where the exit doors are located and note any dead end portions of a hallway." Dunn [p. 78] states that "when the exterior wind velocity is in excess of 30 miles per hour, the chances of a conflagration are great; however, against such forceful winds, the chances of a successful advance of an initial hose line attack on a structure fire are diminished." According to Dunn [p. 80], if fire fighters aren't able to make forward hose line progress, the interior line should be withdrawn, the door to the fire area closed, and the IC notified. According to Klaene and Sanders [pp. 365-366], the floor area of a fire-resistive building can be very dangerous for fire fighters operating hose lines as the fire can wrap around or move through hallways or concealed spaces, getting between fire fighters and their exit route.
Additional fire fighters and crews did not reach the fifth floor to continue the initial offensive attack because the back-up crew was sent to the wrong floor and other fire fighters ran out of air in the stairwell prior to reaching the fifth floor. Note: The fire fighters were forced to go on air on the third floor landing because the emergency stairwell was charged with smoke.
Captain #1 had received burn injuries when he was nearing the end of the hall due to the increased heat near the emergency stairwell entrance. The victim apparently believed that they had somehow turned and were heading back toward the fire apartment due to the intensity of the heat and the diminished visibility. The heat had increased to the point that the sprinkler head at the end of the hall fused. A common temperature rating for sprinkler heads to fuse is 165° F.
Recommendation #4: Fire departments should ensure that a lifeline is in place to guide fire fighters to an emergency stairwell. 5, 6
Discussion: Klaene and Sanders [p. 366] state that "the hose line is used as the lifeline to safety. Members should stay within range of this protective line, not only for fire suppression purposes but also as a means of finding the stairway in heavy smoke conditions. It is also good practice to place a fire fighter at the stairway opening to the floor. This fire fighter will be needed to help extend the hose and can direct fire fighters to the exit if necessary. Ropes may also be used as lifelines in similar situations as an added safety precaution." When a standpipe connection in a high-rise building stairway is used, it would provide a means by which excess hose line may be flaked up the stairway above the fire floor before fire fighters enter the fire floor, keeping excess hose out of the way. Flaking the hose line up the stairway would help in minimizing hose lines from becoming kinked or piled in areas where fire fighters are operating. The hose line extending from a stairway standpipe into a hallway may be used by the fire fighter as a life line. Dunn [p. 76] states that "Some fire departments connect the hose line to the standpipe outlet on the floor below the fire for safety."
Recommendation #5: Fire departments should instruct and train fire fighters on initiating emergency traffic (Mayday-Mayday) when they become lost, disoriented, or trapped. 2, 7
Discussion: As soon as fire fighters become lost or disoriented, trapped or unsuccessful at finding their way out of a hazardous situation (e.g., interior of structure fire), they must recognize that fact and initiate emergency traffic. They should manually activate their personal alarm safety system (PASS) device and announce "Mayday-Mayday" over the radio. A "Mayday-Mayday" call will receive the highest communications priority from Central Dispatch, Incident Command, and all other units. The sooner Incident Command is notified and a RIT is activated, the greater the chance of the fire fighter being rescued. Fire fighters should initiate emergency traffic while they are still capable, and not wait until they are too weak or low on air to call for help. A transmission of the Mayday situation should be followed by the fire fighter providing clues as to his last known location. The fire fighter should then try to remain calm (conserving air), stay in radio contact with command and the RIT, and survey the surroundings in an attempt to gain a bearing of direction or potential escape routes. It is important that if the fire fighter is not in immediate danger of fire impingement or collapse, that he remains in the safe area and moves as little as possible. This will conserve air and possibly help the RIT find the fire fighter more quickly than if the fire fighter were constantly moving. These steps should be incorporated into the department's standard operating procedures with fire fighters trained on those procedures. Investigators were unable to determine, through interviews or equipment examination, whether the victim had manually activated his PASS device or the device had gone into alarm mode.
Recommendation #6: Fire departments should ensure that a Rapid Intervention Team (RIT) is established and in position. 1, 8
Discussion: As stated in NFPA 1500, "a rapid intervention team shall consist of at least two members and shall be available for rescue of a member or a team if the need arises. Once a second team is assigned or operating in the hazardous area, the incident shall no longer be considered in the 'initial stage,' and at least one rapid intervention crew shall be required."
The fire department's standard operating procedures for high-rise fire fighting designates the fifth Engine Company dispatched on the first alarm as the initial rapid intervention team (RIT). The RIT would consist of a minimum of three, preferably four members. The RIT would proceed to two floors below the fire floor with at least one extra air bottle per member, one extra self-contained breathing apparatus, appropriate forcible entry tools, high-rise attack line with nozzle, and a RIT kit. At this particular incident, the fifth Engine Company dispatched on the first alarm arrived on the scene as the initial Mayday was called by the victim. The Engine Company's response to the scene had been delayed due to the heavy rain.
Recommendation #7: Fire departments should ensure that a backup line is manned and in position to protect exit routes. 5
Discussion: Klaene and Sanders [pp. 280-281, 366] state that "backup lines are needed to protect the crew on the initial attack line, to provide additional flow if needed, and should be at least as large as the initial attack line. Backup lines should always be in place to protect exit routes."
Recommendation #8: Fire departments should ensure that adequate numbers of staff are available to immediately respond to emergency incidents. 9
Discussion: As stated in NFPA 1710 (5.2.1.1) "On-duty fire suppression personnel shall be comprised of the numbers necessary for fire-fighting performance relative to the expected fire-fighting conditions. These numbers shall be determined through task analyses that take the following factors into consideration:
(1) Life hazard to the populace protected
(2) Provisions of safe and effective fire-fighting performance conditions for the fire fighters
(3) Potential property loss
(4) Nature, configuration, hazards, and internal protection of the properties involved
(5) Types of fireground tactics and evolutions employed as standard procedure, type of apparatus used, and results expected to be obtained at the fire scene.
NFPA 1710 recommends that a minimum acceptable fire company staffing level should be four members responding on or arriving with each engine and each ladder company responding to any type of fire. It also recommends that for companies responding in high-risk areas, a minimum of five or six members responding or arriving with each engine and each ladder company. The initial arriving company must also be able to implement an initial rapid intervention crew (IRIC).
This was a high risk incident given the high-rise structure, residential occupancy with reports of trapped civilians, and adverse weather conditions. The district involved in this incident is comprised of numerous high-risk residential occupancies, neighborhoods with structures in close proximity to one another, special medical occupancies, high-rise occupancies, and hazardous materials occupancies.
High wind may have exacerbated the situation by increasing conditions whereby the fire extended outside the room in which it originated in a shorter period of time. A National Institute of Standards Technology model of a high rise apartment fire of a similar incident suggests that winds can increase the hazards to the fire fighters and occupants by pushing the heat and smoke from the fire into different parts of the structure through windows and stairwells. The complete fire model will be available for viewing online in the near future at http://www.fire.nist.gov.
Rapid and aggressive interior attack of structure fires, as close as possible to the point of origin, can reduce human and property losses. Suboptimal staffing of arriving units may have delayed such an attack, thus allowing the fire progress to more dangerous conditions for fire fighters and civilians.
Recommendation #9: Fire departments should ensure that the Incident Commander (IC) continuously evaluates the present weather conditions (i.e., high winds) during high-rise fire operations. 5, 6
Discussion: Klaene and Sanders [pp. 59-63] state that "while responding, the dispatcher may be able to provide additional information to the responding units. Companies arriving on the scene should give status reports such as any visual indications of a working fire. During the response, all previous information is reconsidered, such as what effect the high winds will have on the operation. Initial information received from units on the scene is critical to helping formulate a strategy. The incident commander (IC) must consider the effect of the present weather conditions on the operation. High wind affects fire spread and ventilation, especially in high-rise structures." Dunn [p. 26 and 116] states that "At a low rise building fire, the heat of the fire, convection currents, fire pressure and wind determines movement of smoke. In a high-rise building fire, smoke is moved by these four factors, plus the stack effect and the currents induced by (HVAC) heating venting and air conditioning system. The stack effect is the natural movement of air in a high-rise building caused by the difference in temperature and atmospheric pressure inside and outside. The HVAC system should be shut off on arrival at a high-rise fire."
Additionally,
Recommendation #10: Fire departments should establish and enforce standard operating procedures on the use of thermal imaging cameras for search-and-rescue operations. 2
Discussion: Standard operating procedures (SOPs) provide specific information and instructions on how a task or assignment is to be accomplished. SOPs are established so that all members of a department will perform the same function with the same level of uniformity. These procedures are generally tactical in nature because in most instances they address emergency operations. At the time of the incident, the department did not have any SOPs regarding the use or application of thermal imaging cameras for search-and-rescue operations; however, thermal imaging cameras were assigned to all ladder trucks. Thermal imaging cameras with transmitters were assigned to rescue trucks, hazmat units, and the command van. The potential of a thermal imaging camera to improve fire fighting and rescue operations will not be fully realized without commensurate training and procedures.
Recommendation #11: The authority having jurisdiction shall ensure that the receipt and processing of alarms is completed in a timely manner. 10
Discussion: NFPA 1221, 4-3.1 states "the authority having jurisdiction shall ensure that the number of telecommunicators needed to effect the prompt receipt and processing of alarms shall be as follows: 1) In jurisdictions receiving 730 or more alarms per year, at least one telecommunicator shall be on duty in the communication center; 2) ninety-five percent of alarms shall be answered within 30 seconds, and in no case shall the initial call taker's response to an alarm exceed 60 seconds; 3) the dispatch of the emergency response agency shall be made within 60 seconds of the completed receipt of an emergency alarm; and 4) communication centers that provide emergency medical dispatching (EMD) protocols shall have two telecommunicators on duty at all times."
The initial 911 call reporting this fire was received at 04:43:36 hours. The initial dispatch was not completed until 04:48:48 hours, more than five minutes after the initial 911 call. The first arriving units arrived on the scene at 04:53:44 hours. Ten minutes had elapsed from the initial 911 call until the first arriving units arrived on the scene.
REFERENCES
Texas fire department standard operating procedures (SOPs) [2000].
Fire Fighter's Handbook [2000]. Essentials of fire fighting and emergency response. New York: Delmar Publishers.
Morris GP, Brunacini N, Whaley L [1994]. Fire ground accountability: the Phoenix system. Fire Engineering 147(4):45-61.
Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books & Videos.
Klaene B, Sanders R [2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
Dunn V [1999]. Command and control of fires and emergencies. Saddle Brook, NJ: Fire Engineering Books & Videos.
Hoffman, JJ [2002]. MAYDAY-MAYDAY-MAYDAY. Fire Department Safety Officers Association Health and Safety for Fire and Emergency Service Personnel 13(4):8.
NFPA [1997]. NFPA 1500. Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
NFPA [2001]. NFPA 1710. Standard for the organization and development of fire suppression operations, emergency medical operations, and special operations to the public by career fire departments. Quincy, MA: National Fire Protection Association.
NFPA [1999]. NFPA 1221, Standard for the installation, maintenance, and use of emergency services communications systems. Quincy, MA: National Fire Protection Association.
INVESTIGATOR INFORMATION
The lead investigator for this report is Mark McFall, Safety and Occupational Health Specialist. The following NIOSH staff participated in the site visit: Nancy Romano and Frank Washenitz, Safety and Occupational Health Specialists, and Robert Koedam, Chief, Trauma Investigations Section, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH.
EXPERT REVIEW
Expert review was provided by Vincent Dunn, Deputy Chief (Ret.), FDNY.
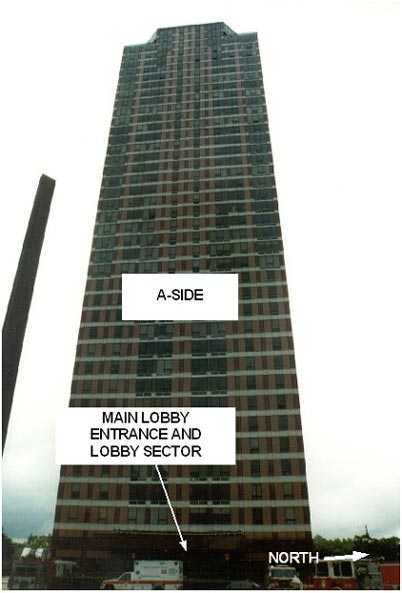
Photo 1. View of A-Side of Building

Photo 2. View of D-Side of Building
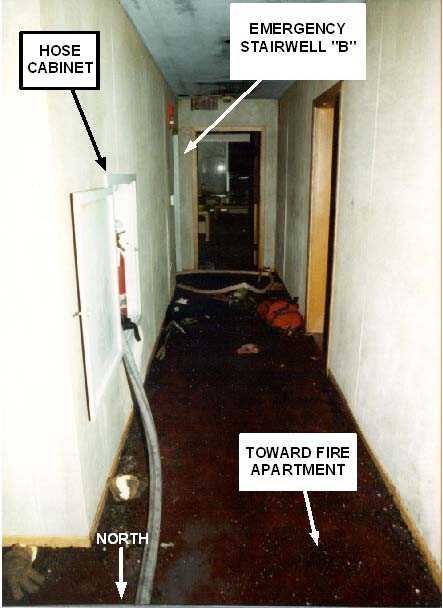
Photo 3. View of Hallway Leading Toward Emergency Stairwell "B"
Diagram 1. Lobby Layout
Diagram 2. 5th Floor Layout
Diagram 3. 5th Floor / Fire Apartment
APPENDIX I
Status Investigation Report of One
Self-Contained Breathing Apparatus
Submitted By the
Fire & Arson Investigation Division
Texas Fire Department
NIOSH Task No. TN-12192
January 10, 2002
Disclaimer
The purpose of Respirator Status Investigations is to determine the conformance of each respirator to the NIOSH approval requirements found in Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). A number of performance tests are selected from the complete list of Part 84 requirements and each respirator is tested in its "as received" condition to determine its conformance to those performance requirements. Each respirator is also inspected to determine its conformance to the quality assurance documentation on file at NIOSH.
In order to gain additional information about its overall performance, each respirator may also be subjected to other recognized test parameters, such as National Fire Protection Association (NFPA) consensus standards. While the test results give an indication of the respirator's conformance to the NFPA approval requirements, NIOSH does not actively correlate the test results from its NFPA test equipment with those of the NFPA. Thus, the NFPA test results are provided for information purposes only.
Selected tests are conducted only after it has been determined that each respirator is in a condition that is safe to be pressurized, handled, and tested. Respirators whose condition has deteriorated to the point where the health and safety of NIOSH personnel and/or property is at risk will not be tested.
Investigator Information
The SCBA inspections and performance tests were conducted by and this report was written by Thomas McDowell, General Engineer and Vance Kochenderfer, Quality Assurance Specialist, Respirator Branch, National Personal Protective Technology Laboratory, National Institute for Occupational Safety and Health, located in Morgantown, West Virginia.
Status Investigation Report of One
Self-Contained Breathing Apparatus
Submitted By the
Fire & Arson Investigation Division
Texas Fire Department
NIOSH Task No. TN-12192
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Respirator Branch agreed to examine and evaluate one Scott Health & Safety (Scott) 4500 psi, 30-minute, self-contained breathing apparatus (SCBA). The Fire & Arson Investigation Division reported that the SCBA was last used during interior firefighting operations at a structure fire on October 13, 2001.
This SCBA status investigation was assigned NIOSH Task Number TN-12192. The Fire & Arson Investigation Division was advised that NIOSH would provide a written report of the inspections and any applicable test results.
The SCBA, sealed in a corrugated cardboard box, was delivered to the NIOSH Appalachian Laboratory for Occupational Safety and Health (ALOSH) on November 20, 2001. Upon arrival, the sealed package was taken to the Firefighter SCBA Evaluation Lab (Room 1520) and stored under lock until the time of the evaluation.
SCBA Inspection
The package from the Fire & Arson Investigation Division was opened, and the SCBA inspection was initiated on December 19, 2001, in Room 1520 of the ALOSH Building. The inspection of the SCBA (referred to as Unit #1) was completed that same day. The SCBA was inspected by Thomas McDowell, General Engineer, and Vance Kochenderfer, Quality Assurance Specialist, of the Respirator Branch, National Personal Protective Technology Laboratory (NPPTL), NIOSH. The SCBA was examined, component by component, in the condition as received to determine its conformance to the NIOSH-approved configuration. The entire inspection process was videotaped. The SCBA was identified as a Scott Air-Pak® 4.5.
The only unusual observation made during visual inspection was the presence of water in the connection between the cylinder outlet and the high pressure coupling. The amount was more than would be expected to occur by condensation, indicating that part of all of the SCBA may have been submerged. This was allowed to drain and it was determined that the unit could be tested safely.
It was noted during the inspection that a personal identifier was engraved on the facepiece lens. While no structural damage to the lens was observed to result from this, it can cause cracks or weakening, and NIOSH discourages this practice. The manufacturer should be consulted to determine the proper method for marking SCBA components.
Although the cylinder was found to be past its required retest date, it was desired to test the entire SCBA in its condition as received. A thorough visual inspection was performed and special precautions were taken during filling and use to ensure that the cylinder did not present a hazard.
Personal Alert Safety System (PASS) Device
A Personal Alert Safety System (PASS) device was attached to the backframe of the SCBA. During the inspection, the PASS device was activated both manually and automatically. Although the unit appeared to function normally, it was not tested against the requirements of NFPA 1982 - Standard on Personal Alert Safety Systems (PASS), 1998 Edition. Because NIOSH does not certify PASS devices, no further testing or evaluations were conducted on the PASS unit.
SCBA Testing
The purpose of the testing was to determine the SCBA's conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA's conformance to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981 - Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
The following performance tests were conducted on the SCBA:
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
1. Positive Pressure Test [42 CFR 84.70(a)(2)(ii)]
2. Rated Service Time Test (duration) [42 CFR 84.95]
3. Gas Flow Test [42 CFR 84.93]
4. Exhalation Breathing Resistance Test [42 CFR 84.91(c)]
5. Static Facepiece Pressure Test [42 CFR 84.91(d)]
6. Remaining Service Life Indicator Test (low-air alarm) [42 CFR 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
7. Air Flow Performance Test [NFPA 1981, Chapter 6, 6-1]
Testing of the SCBA was initiated on December 20, 2001. Six performance tests were completed that day. The first two performance tests listed above are conducted concurrently. On December 21, 2001, the Exhalation Breathing Resistance Test was completed.
All testing was videotaped with the exception of the Exhalation Breathing Resistance Test.
The SCBA met the requirements of all tests except for the Remaining Service Life Indicator Test. The indicator activated prematurely; it alarmed at 1240 psi when the proper set point should have been between 1035 and 1215 psi.
During the Rated Service Time Test, droplets of water were observed to spray from the facepiece-mounted regulator onto the interior surface of the lens. While not an ordinary occurrence, this did not cause the unit to fail the test.
Summary and Conclusions
On November 20, 2001, a package arrived at NIOSH from the Fire & Arson Investigation Division of the fire department involved in this incident. The sealed package was immediately taken to the Firefighter SCBA Evaluation Laboratory (room 1520) for secured storage. The package seal was broken on December 19, 2001. The package was found to contain one complete Scott Air-Pak 4.5, 30-minute, 4500 psi, SCBA (NIOSH approval number TC-13F-76). The SCBA inspection was performed that day.
The SCBA has the appearance of having seen considerable use. It contained some water in the breathing circuit, and the cylinder was beyond its required retest date. The SCBA was determined to be in a condition safe for testing, with appropriate precautions being taken.
The SCBA was subjected to a series of seven performance tests. Testing began on December 20, 2001, and was completed on December 21. No maintenance or repair work was performed on the SCBA at any time. The unit met the requirements of all tests except for the Remaining Service Life Indicator Test, where the Vibralert indicator activated prematurely.
In light of the information obtained during this investigation, the Institute has proposed no further action at this time. Following inspection and testing, the SCBA was returned to the package in which it was shipped to NIOSH and stored under lock in Room 1520 pending return to the Fire & Arson Investigation Division. Note: After the release of this report, the SCBA was returned to the fire department in February 2002.
If the SCBA is to be placed back in service, it must be repaired, inspected, and tested by a qualified service technician. This should include replacement of missing identification and approval labels. Department of Transportation regulations require the cylinder to undergo inspection and hydrostatic testing by an authorized retester before the cylinder can be returned to service.
This page was last updated on 10/24/02
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research