


A Career Lieutenant Dies and Three Fire Fighters are Injured in Ladder Truck Crash - Massachusetts
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2009-05 Date Released: February 26, 2010
SUMMARY
On January 9, 2009, a 52-year-old male career Lieutenant (the victim) died and three male career fire fighters were injured, when the ladder truck they were riding in failed to stop while traveling down a hill. The ladder crew had just cleared from a medical assist call prior to the incident. The chauffeur turned left out of a parking lot and immediately had to stop and back up to allow the aerial ladder overhanging the cab enough clearance to pass a utility pole on the street. After clearing the pole, the chauffeur immediately negotiated a right downward curve. He then applied the brake pedal and had no response. The chauffeur told the victim he had "no brakes" as the ladder truck gained speed descending the hill. The chauffeur tried placing the ladder truck in neutral and applying the parking (maxi) brake to slow the apparatus down, but there was no response. The chauffeur was able to navigate the ladder truck through a busy intersection, crashing through two parked cars and a brick wall, before coming to rest within a multi-story residential complex. The victim was pronounced dead at the scene; the chauffeur was extricated and transported to a local hospital where he was treated for serious traumatic injuries. The two fire fighters riding in the crew compartment were also transported to the hospital with minor injuries.

|
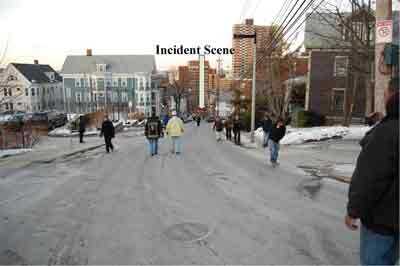
Incident scene. |
Key contributing factors identified in this investigation include apparatus braking system deficiencies, deficiencies in the apparatus maintenance program, insufficient training for fire apparatus operators and fleet maintenance personnel, and failure to wear seat belts.
NIOSH investigators concluded that, in order to minimize the risk of similar occurrences, fire departments should:
- Ensure that preventive maintenance programs are developed and implemented for fire apparatus according to manufacturer guidelines/specifications and national consensus standards.
- Ensure that preventive maintenance on fire apparatus is performed and/or overseen by qualified personnel who meet the certification requirements outlined in NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications.
- Develop and utilize policies and procedures that monitor preventive maintenance and other automotive services performed by vendors.
- Work with local, state, and federal authorities having jurisdiction (AHJ) in adopting an air brake endorsement for noncommercial driver's licenses that would require individuals operating air brake equipped fire apparatus to verify their knowledge and skill proficiency (e.g. air brake system, air pressure gauges and alarms, and pre-trip inspection) prior to operating the fire apparatus.
- Ensure that current driver training programs provide ample classroom instruction, behind the wheel driving, procedures for driver clearance, and annual refresher training.
- Develop and implement fire apparatus inspection procedures and check sheets for their fleet, provide a systematic approach for communicating and receiving inspection sheets from the field, and institute a system to file and track fleet records (e.g., inspection sheets, work orders, repairs, apparatus specifications, and maintenance).
- Ensure that policies and procedures are developed and enforced on the use of seat belts.
- Develop policies and procedures that assist with determining specifications for new apparatus and replacement cycles of existing fire apparatus.
Additionally, fire departments and fleet maintenance divisions should:
- Understand that the manual adjustment of automatic slack adjusters, a mechanical component of the air brake system that adjusts brakes as necessary when the vehicle is in operation, may contribute to unexpected brake failure.
Additionally, governing municipalities (federal, state, regional, and local) should:
- Consider enacting legislation to include operators and occupants of fire department vehicles in existing seat belt legislation and/or repeal existing laws that exempt drivers and occupants of fire service vehicles from mandatory seat belt use.
INTRODUCTION
On January 9, 2009, a 52-year-old male career Lieutenant (the victim) died and three male career fire fighters were injured, when the ladder truck they were riding in failed to stop while traveling down a hill. On January 10, 2009, the U.S. Fire Administration (USFA) notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. The fire apparatus was impounded following the January 9, 2009 incident and secured at the local transit authority police department's restricted-access facility. On February 2-6, 2009, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program, and a fire service consultant knowledgeable in fire apparatus operations, preventive maintenance, and performance requirements contracted by NIOSH, traveled to Massachusetts to investigate this incident.
The NIOSH investigators and consultant met with members of the fire department assigned to their board of inquiry (BOI), union representatives, police detectives and investigators, and individuals assigned to the automotive maintenance division. The NIOSH investigators and the consultant inspected the ladder truck's brake system components with representatives present from the local police department, BOI, and fire fighter's union. The ladder truck and brake system components were also photographed. Photos and witness statements taken by police and the fire department's BOI were reviewed. The NIOSH investigators and the consultant visited the apparatus maintenance facility, reviewed maintenance records for the ladder truck, and discussed fire department procedures for apparatus repair work. NIOSH investigators and the consultant also visited the incident site and took photographs. The NIOSH investigators returned to Massachusetts on June 15-19, 2009 to interview fire fighters and officers involved with the incident and those who had experience in operating the ladder truck. The investigators also reviewed driver/operator training records for the chauffeur, 911 dispatch logs, and the driver training program for the fire department. After collecting the preliminary information, NIOSH developed a Safety Advisory entitled, Manual Adjustment of Automatic Slack Adjusters May Contribute to Unexpected Brake Failure on Automotive Fire Apparatus1, to notify the fire service to take immediate steps to ensure that automatic slack adjusters are not manually adjusted and to establish procedures to ensure apparatus maintenance is conducted by qualified technicians following recommended guidelines of the National Fire Protection Association. The complete Safety Advisory can be viewed at the NIOSH website http://www.cdc.gov/niosh/docs/2010-102/. (Link Updated 1/15/2013)
FIRE DEPARTMENT
This career fire department has 35 stations with 1,505 uniformed members (during the investigation) that serve a population of approximately 600,000 within an area of about 45 square miles.
The fire department has a combined facility and apparatus maintenance division. At the time of the investigation, this division was staffed with a deputy fire chief, a district chief, a lieutenant, eight fire fighters, and six civilians that oversaw and maintained building facilities and apparatus. Note: Up until the 1980s, the department had employed civilian mechanics, but due to budget constraints, those positions were eliminated. In regards to apparatus maintenance, the division is responsible for: scheduling routine preventive maintenance and service calls; shuttling apparatus to, from, and between vendors and fire stations; minor repairs/adjustments (e.g., replacing lights bulbs and wiper blades, adjusting brakes, changing tires); responding to apparatus crashes; and, record keeping for all department apparatus which includes 33 engines, 22 aerial ladder trucks, 2 rescue trucks, 23 spare apparatus pieces, and numerous response/support vehicles (e.g., SUVs, vans, mid-size cars, etc.).
The apparatus maintenance division did not have policies or procedures for preparing, performing, and verifying work completed on department apparatus by division staff or vendors. At the time of the incident, the division did not have an apparatus inspection program or preventive maintenance schedule within the fire stations. The division relied on the driver/operator and/or station officer to notify them of apparatus concerns or problems. Although not routinely used, a form was available which allowed the station officer to notify the maintenance division of apparatus needing to be serviced and document the problem(s). However, no guidance had been provided to field fire fighters or officers to make a determination on what was considered a potential problem.
When an apparatus was received by the maintenance division, they would attempt to diagnose the problem before sending it out to an approved list of vendors. An apparatus would be taken to one of several vendors depending on how quickly repairs or services could be completed. Once repairs were completed members in the division would validate exterior work performed, but there was no procedure to monitor or verify mechanical or engine repair work prior to placing the apparatus back in service. The maintenance division relied on hand written notes and informal logs for apparatus record keeping. They currently have electronic software that can help manage the apparatus (e.g., daily logs, maintenance records, work requests, etc.), but because of staffing constraints, it is utilized in a limited fashion, and the full potential of the software has not been realized.
TRAINING and EXPERIENCE
The fire department provides emergency vehicle driver training to fire recruits while in recruit school, but had not established a refresher driver training program. The department uses the Volunteer Firemen's Insurance Services, Inc. (VFIS) program on driver training.2 This course includes eight hours of classroom instruction covering topics such as human and legal aspects, standard operating procedures/guidelines (SOPs/SOGs), emergency vehicle operations and safety, and vehicle inspection and maintenance. A second eight hour session provides for driver training within a predesigned obstacle course according to NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications.3 The obstacle course is designed to test the driver's judgment, skill, and emergency vehicle knowledge through scenarios such as parallel parking, driving around objects, and driving in diminished clearances. The chauffeur successfully completed both the written and driver competency tests required by this course in May 2007. Once the course is successfully completed, the VFIS program suggests that a minimum of 10 supervised hours be spent on over-the-road driving for each apparatus the driver will operate. This training should be documented by the fire department, but does not need to be verified by VFIS. The fire department did not have a formal policy or procedure to clear a chauffeur to drive/operate a fire apparatus.
Once a fire fighter graduates from recruit school they are assigned to a fire station, and provided time to operate the apparatus under non-emergency conditions, working their way up to emergency response(s). The fire fighter also receives hands-on training by department members on basic apparatus checks (e.g., tire pressure, water tank level, battery changes on handheld radios, etc.). The company officer makes a determination when the fire fighter will be cleared to operate an apparatus without supervision. The company officer may document the fire fighter's over-the-road driving hours within the station's daily officer log. The chauffeur graduated from the department's drill school in July 2007 and began operating fire apparatus in November 2007 on non-emergency responses. In September 2008, the chauffeur was released to operate the ladder truck on a full-time basis. Prior to the fatal incident, the chauffeur had driven the ladder truck involved in this incident for approximately 10 duty shifts. The chauffeur routinely worked 24 hour shifts, but the actual driving hours could not be determined by NIOSH investigators. The chauffeur had prior experience driving fire apparatus while in the military, and had no prior documented vehicle incidents.
Staff within the facility and apparatus maintenance division had not received departmental training or vehicle/apparatus maintenance certification (e.g., National Institute for Automotive Service Excellence (ASE)4 or NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications5) to assist them in performing work on fire department apparatus. Many relied on previous personal experiences with vehicles and/or on the job training. Since the incident, the fire department has hired a fleet manager, fleet safety officer, and certified mechanics, all civilians, to oversee the fire department's apparatus fleet. Due to a change in the department's record keeping system, no training records were available for the victim that could be assessed.
EQUIPMENT and PERSONNEL
The incident involved a ladder truck with two firefighters, Lieutenant (victim), and a chauffeur. The apparatus involved in this incident was a 1995, 110-ft rear-mounted aerial ladder truck with a diesel engine, automatic transmission, and anti-lock and air brake systems (see Photo 1). Based on the department's aerial ladder specifications sheet6 for that year, the engine was a 736 cubic inch turbocharged two-cycle diesel engine. The automatic 4-speed transmission was specified to have an integral output retarder using a hydrodynamic braking system capable of being activated through normal application of the air brake treadle valve utilizing a step apply system to activate it, and a foot control valve supplied to provide modulated application to the retarder system. The specifications also included installation of a retarder enable switch to activate the retarder system with separate indicator lights mounted in the cab that would indicate activation of the retarder and retarder overheating. The air brake system was specified to have separate brake chambers for each wheel, a dual treadle valve splitting the braking power between the front and rear systems, an air dryer with an additional 1,738 cubic inch reservoir added to the air system to serve as a wet tank and a quick build-up for sufficient volume of air to comply with Federal Motor Vehicle Safety Standard 121 (FMVSS 121)a, and spring actuated emergency/parking brakes installed on the rear axle.

|
Photo 1. Aerial ladder truck following the incident. |
The ladder truck's front gross axle weight rating (GAWR) was 18,700 pounds and the rear GAWR was 30,250 pounds with a total gross vehicle weight rating of 48,950 pounds. The ladder truck was mounted on a 215-in wheel base and had two axles with six wheels (two in the front and four in the rear). The engine hour counter registered a total of 13,925 hours. The odometer was destroyed during the crash, but the last documented odometer reading was 77,712 in October 2005. The ladder truck had a current state inspection as required by the Commonwealth of Massachusetts.
The Commonwealth of Massachusetts does not require any special driver's license endorsement or commercial driver's license (CDL) to operate a fire apparatus.7, 8
a FMVSS 121 is a federal standard that specifies performance, equipment and dynamometer test requirements for braking systems on vehicles equipped with air brake systems, including air-over-hydraulic brake systems, to ensure safe braking performance under normal and emergency conditions.9
The ladder truck had been involved in three previous incidents: in August 2006, July 2007, and December 2008. The two more recent incidents involved motorists pulling in front of the ladder truck and the ladder truck not being able to stop in time (brakes not believed a contributing factor). The incident in August 2006 occurred on the same hill that the fatal incident occurred. A chauffeur was backing out of an alley onto the roadway in order to go up the hill when the brakes failed to stop the apparatus. The ladder truck continued backwards down the hill as the chauffeur attempted to set the maxi brake and pump the brake pedal. While this was occurring, the company officer recalls hearing the low air alarm for the air brake system sounding while he stood at the front of the ladder truck. The ladder truck backed down the hill for a short period before the chauffeur cut the apparatus to the left striking a building, but stopping the apparatus. Nobody was hurt in the three prior incidents. Following the August 2006 incident, the ladder truck was placed out of service and a brake job conducted, including replacement of front pads and rotors; and, replacement of both rear spring brake chambers, drums, shoes, and S-cams. Prior to the August 2006 incident, the ladder truck received a brake job (October 2005) that included replacement of both rear spring brake chambers, front pads and rotors, calipers, and automatic slack adjusters. Note: The October 2005 and August 2006 brake jobs had different sized air brake spring chambers replaced on the rear axle by the same vendor; size 30/30 installed in October 2005 and size 30/36 installed in August 2006. Prior to this, a different vendor installed 36/36 in June 2002 and 30/36 in December 2003. The brake chamber type number denotes the square inches of effective area of a brake chamber's diaphragm. Braking force is determined by multiplying the delivered air pressure by the effective diaphragm area. The first number is the service brake diaphragm size and the second number is the spring (parking) brake size. The manufacturer calls for 36/36 rear brake chambers on this size apparatus because 30 inch chambers do not provide adequate braking force. Within three months of the October 2005 brake job, the brakes needed to be adjusted. Note: Automatic slack adjusters (ASA) should not be manually adjusted after the initial installation adjustment; manually adjusting an ASA to correct an out-of-adjustment brake will not fix the underlying problem(s) (e.g., defective ASA, improper installation, or associated problems with other braking components). The apparatus should be taken out-of-service immediately.1, 10 The ladder truck received a total of five documented manual adjustments of the ASAs prior to the August 2006 incident, with one of these adjustments two weeks prior to that incident. In the four years leading up to the fatal incident, the ladder truck had received three documented brake jobs and twelve manual adjustments of the ASAs (the five documented adjustments prior to the August 2006 incident are included in the twelve total adjustments). The documented manual adjustments were conducted by fire department apparatus maintenance personnel, and the fire department maintained an approved outside vendor list for work that could not be completed within the fire department's apparatus maintenance division. Fire apparatus could be moved from vendor to vendor depending on who could service the apparatus and have it back in service the fastest.
TIMELINE
- 1405 Hours
Ladder truck dispatched for a difficulty breathing medical assist call. - 1406 Hours
Ladder truck en route. - 1410 Hours
Ladder truck arrives at the medical assist call. - 1414 Hours
Ladder truck updates dispatch on the patient’s condition. - 1428 Hours - estimated by fire department investigators
Ladder truck clears the medical assist call. - 1432 Hours
A fire fighter from the ladder truck states, "fire alarm, Ladder 26 has crashed into a building."
PERSONAL PROTECTIVE EQUIPMENT
At the time of the incident, the victim was wearing his department issued uniform shirt and pants, steel-toed work boots, and bunker coat, and the chauffeur was wearing his station house uniform shirt and pants, and steel-toed work boots.
WEATHER and ROAD CONDITIONS
The temperature was 25°F and sunny. According to the chauffeur and witnesses interviewed, road conditions were dry and free of snow and ice. The paved city street was 26 ft wide with cars parked on the left side of the road when descending the hill. The street had a posted speed limit of 25 miles per hour (mph) and a 13% downward grade (see Photo 2). The police department crash investigator estimated the ladder truck had accelerated to an approximate speed of 57 mph when entering the intersection.
|
|
Photo 2. View from atop the hill after the incident. (Photo courtesy of fire department.) |
INVESTIGATION
On January 9, 2009, a 52-year-old male career Lieutenant (the victim) died and three male career fire fighters were injured when the ladder truck they were riding in failed to stop while traveling down a hill. The ladder truck and crew had responded to approximately five calls prior to the fatal incident. Nothing out of the ordinary was noted, especially in apparatus braking capability. Just prior to the incident, the ladder truck responded on a medical assist call with the city's emergency medical service's (EMS) department. The ladder truck responded from quarters at 1405 hours and traveled approximately 1.4 miles as they responded through six intersections and made two left hand turns before it ascended the hill (see Photo 3) where the incident occurred.

|
Photo 3. View from the bottom of the hill; taken after the fatal incident. |
At the top of the hill, the chauffeur turned right into a medical facility's parking lot (the location of the medical assist call) and drove straight to the front entrance. The ladder truck came to a complete stop allowing the victim and the other two fire fighters to exit the ladder truck and enter the facility. The chauffeur then drove forward and turned right around an island to position the ladder truck toward the exit of the parking lot. The chauffeur stated he had to reposition the ladder truck due to the wide turn needed in order to get the ladder truck around the island. Once the ladder truck was straightened up and facing the exit, the chauffeur placed the push button gear system to "neutral" and set the parking brake. The chauffeur does recall hearing a release of air when he engaged the ladder truck's spring actuated parking brake.
The chauffeur briefly exited the cab of the ladder truck to get a bearing on his surroundings. He stated that he noticed no movement of the ladder truck after he exited. He then reentered the cab of the ladder truck and waited for the victim and other fire fighters to finish assisting EMS.
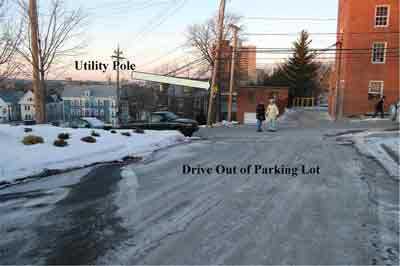
When preparing to leave the medical call, the chauffeur placed the ladder truck in "drive" and released the parking brake. The chauffeur pulled forward and turned left out of the parking lot, immediately stopped, and then backed up to reposition the ladder truck so that the ladder did not strike a utility pole (see Photo 4). He pulled forward again and carefully negotiated the ladder truck away from the utility pole.
|
Photo 4. Shows the left hand turn the chauffeur had to make |
After this maneuver, the chauffeur had to immediately negotiate the aerial ladder through a right hand, downward curve (see Photo 5). Once the ladder truck was straight and descending the hill, the chauffeur applied pressure with his foot to the brake pedal and had no response. The brake pedal went to the floor without resistance. He quickly began pressing the brake pedal in an attempt to get the brakes to actuate as he advised the victim that he had "no resistance or pressure" when applying his foot on the brake pedal.

|
Photo 5. Right downward curve negotiated by ladder truck chauffeur. |
The chauffeur continued to press the brake pedal repeatedly and then attempted to place the truck in "neutral" and engage the parking brake several times. According to interviews reviewed by NIOSH investigators, it does not appear that the chauffeur attempted to place the ladder truck in a lower gear to see if the engine retarder would assist in slowing the ladder truck down. The apparatus also had a push-button transmission retarder switch located within the cab with an on/off indicator light. Note: The push-button switch was in the activated position during our inspection of the ladder truck following the incident. The ladder truck continued to accelerate down the hill with no apparent response from the parking brake. The chauffeur began to veer the ladder truck toward parked cars or utility poles, but the victim instructed him not to hit anything. The chauffeur does not believe he heard an audible or saw a visual alarm indicating that something was wrong with the air brake system. Note: When interviewed by police investigators, the chauffeur stated that he had never received training on what the air pressure should be, what the gauge should read, or how to check/inspect an air brake system. He had been told by other department fire fighters that an indicator light would activate indicating low air pressure, but he had never seen this occur. With emergency lights on and electronic siren sounding, the chauffeur was able to negotiate the ladder truck through a busy intersection before he struck two parked cars, went through an 8-ft tall, three course thick brick wall, and came to rest within a multi-story residential building (see Photos 6, 7, and 8). The victim died minutes following the impact and the chauffeur had to be extricated by arriving fire department personnel. Note: The victim, chauffeur, and one of the fire fighters were not wearing a seat belt when the incident occurred. The second fire fighter buckled his seat belt just prior to the ladder truck colliding with the parked cars. The Commonwealth of Massachusetts exempts operators and passengers of fire vehicles from having to wear a seat belt.7

|

|
Photos 6 and 7. Photo at top shows damage received to parked cars and exterior view of brick wall. Photo at bottom shows the thickness
|

|
Photo 8. Damage sustained to multi-story building |
Apparatus Inspection
Following the fatal incident, the ladder truck was transported to a restricted-access facility within the local transit authority police department. The police department and International Association of Fire Fighters (IAFF) local each secured their own separate experts to perform an inspection of the ladder truck. The primary focus of the inspection was the braking system and its’ components. The IAFF local’s expert shadowed the police department’s expert when he inspected the ladder truck on January 13 and 17, 2009. The IAFF local’s expert released his investigative report11 shortly after the inspection to individuals tasked with investigating the ladder truck incident (i.e., BOI and NIOSH). The police department’s final report and their expert’s motor vehicle autopsy investigative report12 were released in December 2009. The city’s District Attorney concluded that no criminal charges were warranted.
In March 2009, at the request of the department's fire commissioner, an independent assessment was performed by a third party firm on the fire department's apparatus maintenance program and practices.13 This assessment included conclusions such as the fire department did not have a fleet manager or apparatus maintenance technicians; lacked an effective vehicle inspection program; lacked procedures for communicating apparatus deficiencies from the field; no defined preventive maintenance program; failure to adequately process work orders; inadequate driver training; and, inability to effectively manage vendor performed services.13
NIOSH contracted with an expert consultant to inspect the ladder truck and evaluate the fire department's apparatus maintenance program on February 3-5, 2009 as part of the NIOSH investigation. See Appendix for a summarized description of the apparatus inspection and findings. The NIOSH consultant concluded that the left rear brake had not worked for some time, and that the front brakes and right rear brake were not working to maximum efficiency. However, because these problems with the braking system existed prior to the incident, the consultant concluded that additional problems also contributed to this incident. Note: Problems prior to the incident include inefficiently working braking components and neglected or incorrect apparatus maintenance. The consultant identified several possible causes of the brake failure:
- Inoperable or improperly working auxiliary braking or transmission retarder.
- Inefficient brakes inability to slow the ladder truck traveling down a steep grade.
- Failure of the air brake system to supply enough air to the brake chambers due to freezing of moisture in a valve, oil in the air tanks, or an inefficient air dryer.
If freezing in the brake system, noted above, had occurred then the driver should not have been able to release the spring brakes when leaving the parking lot. Typically, freezing of the brake system would be more prevalent after 20 minutes of the truck not moving in the parking lot. The fact that the driver was able to release the spring brakes and apply pressure on the brake pedal with brake actuation while negotiating the ladder truck out of the parking lot and around the utility pole indicated that the air system was not frozen. If the air brake pressure had gone down to critical levels (less than 80 psi) then the spring brake system should have activated at some point, applying the spring brakes and locking up the right rear brake (the left rear should have locked up also, but it was not working). If the right rear spring brake had actuated then the apparatus may have pulled to the right or left depending on road conditions. Note: Initial police investigative findings observed during their expert's inspection of the apparatus' rear brake components were not made available to the NIOSH investigators and consultant during our inspection of the ladder truck because their investigation had not been finalized. The NIOSH investigators and consultant were able to view the rear brake components and document findings.
Since the NIOSH consultant inspection, NIOSH investigators were provided with recorded interviews from the police department and fire department BOI of the driver and other occupants on the ladder truck. NIOSH investigators received the final copy of the police investigator's report and their expert's motor vehicle autopsy investigation report in December 2009. However, review of the information contained in these interviews and reports did not allow investigators further specificity in identifying the root cause of why the ladder truck failed to stop on January 9, 2009 because the identified braking system deficiencies noted in the reports existed prior to the fatal incident.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:- Apparatus braking system deficiencies.
- Deficiencies in the apparatus maintenance program.
- Insufficient training for fire apparatus operators and fleet maintenance personnel.
- Failure to wear seat belts.
CAUSE OF DEATH
According to the death certificate, the medical examiner listed the victim's cause of death due to blunt force traumatic injuries to the head.
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should ensure that preventive maintenance programs are developed and implemented for fire apparatus according to manufacturer guidelines/specifications and national consensus standards.
Discussion: NFPA 1911 Standard for the Inspection, Maintenance, Testing, and Retirement of In- Service Automotive Fire Apparatus states that all fire apparatus that could be placed in service for emergency response should be inspected, maintained, tested, and retired as required to keep them in safe operating condition and ready for response at all times.14 Maintenance schedules should be established and recorded as an integral part of a well-planned maintenance program.14 The maintenance program should include daily, weekly, monthly, yearly, and periodic maintenance service checks. The maintenance checks should be based on the manufacturer's service manuals, the tire manufacturer's recommendations, and operating conditions. Safety and operational readiness need to be the highest priority when inspecting and maintaining apparatus. NFPA 1911 recommends that information from several sources, including the manufacturer's manuals and NFPA standards, be used to determine fire apparatus preventive maintenance schedules. As the necessary maintenance tasks are identified, each should be assigned a schedule based on months, years, apparatus hours, or other appropriate time frame that will determine when it is to be performed and by whom. Once the tasks have been performed, frequency determined, and individuals identified to do the work, the preventive maintenance program can be organized into a series of schedules, check sheets, record sheets, and other documentation that will ensure correct implementation of the program.
NFPA 1500 Standard on Fire Department Occupational Safety and Health Program states there should be criteria established to assist a fleet maintenance division in determining when an apparatus should be placed out-of-service.15 NFPA 1911 specifically addresses criteria for taking an apparatus out-of-service. Once out-of-service, the fleet service manager should determine who is capable of performing the work, the fire department fleet maintenance division or a local vendor. A policy addressing preventive maintenance or repair work should be established to better assist the fleet service manager in making this decision.
Prior to this incident, the fire department did not employ a fleet service manager or qualified personnel to oversee daily operations of their fleet service department. Manufacturer or department preventive maintenance programs had not been established to better assist the fire department in making determinations on whether an apparatus needed routine service, repairs, or was safe to be in service. Preventive maintenance programs are designed to reduce apparatus downtime, breakdowns, extend the life of an apparatus, and identify potentially life-threatening problems.
Recommendation #2: Fire departments should ensure that preventive maintenance on fire apparatus is performed and/or overseen by qualified personnel who meet the certification requirements outlined in NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications.
Discussion: NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications establishes the minimum job performance requirements for a person qualified as an emergency vehicle technician (EVT) who is engaged in the inspection, diagnosis, maintenance, repair, and testing of an emergency response vehicle.5 Qualifications should be evaluated by assessing schooling, training, practical experience, and review of existing certification programs. There are a variety of programs that can help fire departments determine if EVT candidates have the requisite knowledge and skills to perform fire apparatus maintenance and repairs. The Automotive Service Excellence, Emergency Vehicle Technicians Certification Commission, the Canadian provincial journeyman license for heavy equipment, the Canadian registered apprentice program under the supervision of a licensed journeyman, a technician certification program recognized by a federal or state agency, or equivalent programs can be utilized to help determine the requisite knowledge and skills of an EVT candidate.5
NFPA 1071 A.1.1 states that "there are certain components on emergency response vehicles that are not unique, but there are many complex, highly integrated components found within the apparatus such as the engine, transmission, and pump with the electronic lockups and interlocks." Because of this complexity, NFPA 1071 recommends that a person qualified as an emergency vehicle technician possess minimum skills and knowledge to inspect, diagnose, and perform repairs, and understand that the root cause of a problem can be beyond the unique component where the symptom is present, and in fact can be related to a component that otherwise might not be considered unique.5 EVT qualified personnel should be performing any scheduled maintenance correctly and entirely, paying close attention to other possible maintenance repair issues that may or may not be related to the apparatus' scheduled prevention maintenance appointment.
Prior to this incident, the fire department fleet maintenance division was staffed with civilians and fire fighters with no vehicle maintenance certification(s) or fleet maintenance training. The ladder truck received numerous documented brake adjustments without ever determining the underlying problem. Having qualified personnel within a fleet service division will allow for better diagnosis of a problem, prevention of potential problems, and decision making regarding vendor performed maintenance and outsourcing.
Since the incident, the fire department has hired a fleet manager, fleet safety officer, and certified mechanics, all civilians, to oversee the fire department's apparatus fleet.
Recommendation #3: Fire departments should develop and utilize policies and procedures that monitor preventive maintenance and other automotive services performed by vendors.
Developing policies and procedures on preventive maintenance can assist a fleet department in performing scheduled maintenance, outsourcing work to be performed, monitoring maintenance conducted, and inspecting completed maintenance. Performing preventive maintenance on a vehicle can be time consuming and redundant at times, but the overall goal is to lengthen the life of a vehicle and diagnose potential problems before they become costly to repair, take a vehicle out-of-service, or pose a safety risk to the operator and/or passenger(s). Preventive maintenance can include things such as oil changes, lubrication, recording condition of parts, and replacing deteriorating parts; and should be done only by appropriately trained and certified technicians. When outside vendors are utilized there should be contractual agreements in place with perspective vendors to ensure they have the appropriate qualifications and that they are familiar with the vehicle or apparatus to be maintained. These vendors should be qualified to perform work on fire apparatus and meet the recommended qualifications and certifications set forth in NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications.5
The fleet department needs to be able to specify to the vendor what maintenance or work needs to be performed, question/research additional work suggested by the vendor, and verify, through visual inspection, that the work was performed to manufacturer and fire department specifications. The vendor should be provided with documentation as to what work should be performed and describe the events leading up to the vehicle issue. If the vendor finds something else wrong, a qualified fire department fleet representative should be able to research previous work performed on that vehicle to verify whether it had been done previously. This assists the fleet department by allowing them to have the final say in whether or not a service is performed. Finally, qualified fleet department personnel should visually inspect that the work requested to be performed was performed correctly with the appropriate equipment replaced to specifications. This provides for overall quality control of the work performed. If the fleet department does not inspect and verify the work performed upon receipt of the vehicle from the vendor, then they risk a chance of potentially establishing responsibility and/or liability in the event that the vehicle component fails after it was purportedly inspected, serviced, and/or repaired by a vendor.13 This is especially important when multiple vendors could be used throughout the life of the vehicle.
As in the case with this fire department, there were several vendors that did routine work on the ladder truck. Prior to the incident, the smaller size brake chambers were placed on the apparatus during a brake job that may or may not have had an affect on the braking ability of the ladder truck. According to the NIOSH expert consultant, the front brake pads were the wrong friction rating for that type of apparatus. Unless the vendor is skilled and knowledgeable in the apparatus and work to be performed, or can verify replacement parts with the manufacturer; they may replace incorrect parts used in prior maintenance work. The department did not document service requests to vendors; only billed invoices from the vendor specifying the services that they performed were kept on file. It is important that procedures are set in place prior to outsourcing apparatus work to a vendor because it will provide the apparatus owner with vendor performed maintenance oversight, accountability, and maximize the value of the fleet maintenance program.
Recommendation #4: Fire departments should work with local, state, and federal authorities having jurisdiction (AHJ) in adopting an air brake endorsement for noncommercial driver's licenses that would require individuals operating air brake equipped fire apparatus to verify their knowledge and skill proficiency (e.g. air brake system, air pressure gauges and alarms, and pre-trip inspection) prior to operating the fire apparatus.
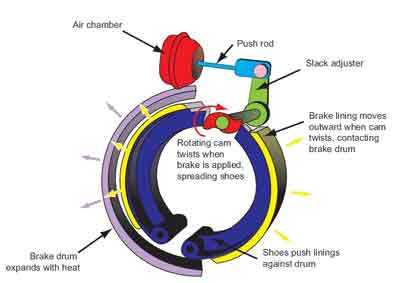
Discussion: Air brake systems are used on most heavy-duty vehicles for reasons of efficiency and reliability. Air brake systems use air as a medium for transmitting pressure or force from the driver control to the service brakes. When an operator of a vehicle presses down on the brake pedal, air is passed through supply lines to the brake chambers forcing the pushrod out. The pushrod, which is attached to a slack adjuster, actuates the slack adjuster and turns the camshaft, which in turn twists the S-cam, forcing the brake shoes to contact the brake drum, which slows the vehicle down due to friction (see Figure 1).
|
Figure 1. Actuation of air supplied brake drums. |
The vehicle operator needs to understand how an air brake system works and how to inspect the system prior to operating the vehicle. The operator needs to be cognizant of all dashboard gauges within the cab of the fire apparatus, but specifically the air pressure gauge.16 The air pressure gauge indicates the amount of air pressure available to operate the vehicle's air brake system. The air pressure gauge reading should stay within the manufacturer's recommendation, which is normally 80-125 pounds per square inch (psi). The driver should know that at 60 psi an audio and/or visual alarm should activate alerting the operator that there is low air pressure, and at 20-40 psi the spring brake (parking brake) should actuate.2 The chauffeur of the ladder truck completed department required driver training (VFIS Emergency Vehicle Driver Training), but stated he did not know what to look for when reading the air pressure gauge. During the incident, the chauffeur does not recall hearing or seeing a low air pressure alarm, but he also stated he had no prior knowledge as to what the low pressure alarm would look or sound like. The chauffeur also indicated that he pressed on the brake pedal repeatedly in an attempt to get the brakes to slow the apparatus down. Repeatedly pressing the brake pedal, or "pumping the brakes," can drastically deplete air pressure within the air brake system, thus lowering the ability of the brakes to slow or stop a vehicle.10 Knowing how to interpret an air pressure gauge reading, ensuring that the system is operating correctly, and understanding how the system should work is paramount.
In October 1986, Congress passed the Commercial Motor Vehicle Safety Act of 198617 which required each State to meet the same minimum standards for commercial driver licensing, now overseen by the Federal Motor Carrier Safety Administration (FMCSA). Most states, including the Commonwealth of Massachusetts, have adopted the American Association of Motor Vehicle Administrators' model for Commercial Driver License Manual. The model manual and Massachusetts' CDL Manual8 contain sections specifically addressing air brake knowledge, pre-trip vehicle inspection, and provides testing modalities and rules, developed by the Federal Highway Administration (FHWA), to verify knowledge prior to receiving one's CDL. If an individual fails to pass the knowledge and skills tests, then they are prohibited from operating any vehicle equipped with an air brake system. Currently, fire departments are exempt from the FMCSA CDL program because fire apparatus do not classify as a commercial vehicle. The adoption of an air brake endorsement for noncommercial vehicles will better ascertain one's knowledge and skill of air brake systems, thus making the fire apparatus driver better capable of operating the fire apparatus. Canada recognized the importance of being air brake proficient when issuing licenses, and since 2001 has seen a decrease in brake-related incidents after Transport Canada required air brake endorsements for all drivers wanting to operate any air brake equipped vehicles.18 Having fire apparatus drivers obtain an air brake endorsement, similar to the proficiency required within a commercial driver's license (CDL), would help ensure that drivers tasked with operating fire apparatus equipped with an air brake system would have the knowledge and skills to do so safely.
Recommendation #5: Fire departments should ensure that current driver training programs provide ample classroom instruction, behind the wheel driving, procedures for driver clearance, and annual refresher training.
Discussion: NFPA 1451 Standard for a Fire Service Vehicle Operations Training Program19 states that fire department personnel must be trained in and exercise applicable principles of defensive driving techniques under both emergency and nonemergency conditions. NFPA 1500 Standard on Fire Department Safety and Health Program15 and NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications3 describe the necessary knowledge and skills individuals need to possess in order to be a driver/operator, including such things as preventive maintenance inspections and demonstration of the proper operation of an apparatus under a variety of conditions.
NFPA 1451 and NFPA 1002 both state that fire departments should establish and maintain a driver training program and each driver/operator should be provided driver training not less than twice a year. Fire departments should be able to provide additional training specific to apparatus that the driver/operator would be assigned to drive. This should include training on how to handle the apparatus under difficult road conditions (e.g., steep grades, grade changes, and narrow roads) and when something unexpected occurs with the apparatus (e.g., unexpected brake failure, tire blowouts, or regaining control). During fire department training, instructors should verify that the driver/operator can safely operate the apparatus in accordance with local and state laws, perform a pre-trip inspection, identify gauges and controls within the cab of the apparatus (e.g., what gauges should read, what readings mean, and how to operate controls and when), and verify knowledge and driver operability of air brake equipped vehicles. Records of driver/operator behind-the-wheel hours and training should be maintained on each driver/operator. Additionally, since most fire apparatus are equipped with an air brake system, fire departments should consider whether their fire department driver training program is sufficient to cover topics and problems associated with air brake equipped vehicles, or should be supplemented by incorporating the state's commercial driver's license certification, or even consider adoption of an air brake endorsement for noncommercial driver's license. Both would assist an instructor in determining a driver/operator's knowledge of air brake equipped vehicles. The department's driver training program will assist the department in making a determination on whether a new driver or current driver is qualified and possesses enough experience to safely operate an apparatus(s). Fire departments should understand that documented training hours alone do not prove that the training was effective. However, the program may help in areas such as speeding, inexperience with apparatus, identification of hazardous situations or actions, overconfidence, urgency, and poor driving habits.
The fire department did train fire fighter recruits according to the driver program developed by VFIS2, but had not instituted an annual driver refresher program. No formal program had been instituted to clear a driver/operator once graduated from recruit school. Behind-the-wheel driving hours may or may not be recorded and placed on file. Station officers would make a determination on when a driver/operator could operate the apparatus without being shadowed by a released driver/operator. The chauffeur stated, during his interview with police investigators, that he did not know how to inspect or check an apparatus equipped with air brakes or what an air pressure gauge should read. During the incident, it appeared that the air brake system failed to stop the ladder truck which was no fault of the chauffeur. Due to lack of training and experience and gravity of the situation encountered by the chauffeur, he attempted to stop the apparatus by continually depressing the brake pedal and placing the apparatus in neutral. Proper training would have provided the chauffeur with an understanding that depressing the brake pedal repeatedly does not allow the air in the brake system to replenish, and that placing an apparatus in "neutral" instead of a lower gear, does not allow engine braking, or compression braking, to occur. Placing an apparatus in a lower gear attempts to slow a vehicle down and transfer mechanical advantage from the downward grade to the engine, thus, counteracting acceleration caused by gravity. But even with this requisite knowledge, NIOSH investigators do not believe that the chauffeur would have been able to stop the ladder truck in this incident.
NFPA 1901 states that apparatus over 36,000 lbs should be equipped with an auxiliary braking system such as an engine retarder, transmission retarder, exhaust retarder, or driveline retarder because these devices can provide various levels of effectiveness on braking, especially apparatus exposed to steep grades or high call volumes; and, these systems can be operated automatically or manually.20
Of importance, fire departments should evaluate all available auxiliary braking systems and determine the system that best fits their department's needs (e.g., terrain, apparatus replacement cycle, or weight). Note: Auxiliary braking systems may need to be turned off when an apparatus is operated on slippery road surfaces. NIOSH investigators recommend that fire departments consult the manufacturer's recommendations regarding the apparatus's auxiliary braking system. The ladder truck involved in this incident was equipped with a brake retarder system. It has not been confirmed if the chauffeur attempted to manually activate the transmission retarder switch located within the cab, or if the on board retarder was working efficiently or operational. The transmission retarder switch was found in the activated position. This was discovered by the NIOSH consultant during his inspection of the ladder truck. It could have already been activated prior to the fatal incident or placed in the on position during/following the fatal incident.
Recommendation #6: Fire departments should develop and implement fire apparatus inspection procedures and check sheets for their fleet, provide a systematic approach for communicating and receiving inspection sheets from the field, and institute a system to file and track fleet records (e.g., inspection sheets, work orders, repairs, apparatus specifications, and maintenance).
Discussion: NFPA 1911 Standard for the Inspection, Maintenance, Testing, and Retirement of In- Service Automotive Fire Apparatus states, "All fire apparatus that could be placed in service for emergency response shall be inspected, maintained, tested, and retired as required by this standard."14 Daily, weekly, monthly, and yearly inspections should be conducted by qualified personnel or individuals. NFPA 1911 further explains that inspections, maintenance, and diagnostic testing on fire apparatus should be performed by qualified personnel meeting qualifications set forth in NFPA 1071 Standard for Emergency Vehicle Technician Professional Qualifications5, or the equivalent, and those performing inspections, maintenance, diagnostic testing, or operational checks on fire apparatus should consult the appropriate operator's, service, and maintenance manuals before starting any work on the apparatus. It is the responsibility of the fire department to determine who is qualified to perform the daily/weekly inspection and the operational checks of fire apparatus. These types of inspections and checks should be able to be conducted within the fire station by driver/operators of the fire apparatus. Guidelines should be established for field personnel to take an apparatus out-of-service if a check or inspection discovers something is wrong.
NFPA 1911 provides example check sheets and forms that can be utilized by fire departments to verify the fire apparatus is ready for service, such as:
- daily/weekly apparatus check form
- quarterly/annual apparatus inspection report
- pump performance test form
- aerial device inspection and performance test form
- low voltage electrical system performance test form
- line voltage electrical system performance test form
- foam proportioning system performance test form
- compressed air foam system compressor performance test form
Once these forms are completed, there needs to be a systematic approach in communicating this information back to the fleet maintenance division. This can be done through emailing of an electronic form, fax, or delivery/receipt of an actual form to the fleet maintenance division. The fleet maintenance division should maintain individual files for each apparatus and keep the file for the life of the apparatus. These files should be well-organized and filed according to date, and include items such as daily/weekly/quarterly/annual checks and inspections, work orders, repairs, apparatus specifications, and performed maintenance. This allows fleet personnel to evaluate the current status of the apparatus and identify potential issues before they arise. These records should be maintained via electronic means, through the use of fleet maintenance managing software, and maintaining paper records as a backup. Developing a sound program for inspecting and checking apparatus will only increase the value of a fire department's fleet and potentially lower the chances of vehicle incidents.
Recommendation #7: Fire departments should ensure that policies and procedures are developed and enforced on the use of seat belts.
Discussion: Vehicle crashes are the second leading cause of fire fighter line-of-duty deaths.21 The fire department involved in this incident did not have a SOP requiring the use of seat belts. NFPA 1500 Standard on Fire Department Occupational Safety and Health Program states that all persons riding in fire apparatus should be seated and belted securely by seat belts in approved riding positions at any time the vehicle is in motion, and the seat belts should not be released or loosened for any purpose while the vehicle is in motion.15 Fire departments should develop, implement and enforce SOPs on the use of seatbelts in accordance with NFPA guidelines. Numerous nationally recognized fire service entities have guidance available on implementing a seat belt policy. The International Association of Fire Fighters (IAFF) provides guidance in their document Standard Operating Procedures, Fire Department Vehicle Safety, Emergency and Non-Emergency Response, and Safe Emergency Operations on Roadways,22 and recommends that all employees use seat belts at all times and "All personnel shall ride only in regular seats provided with seat belts. The company officer and driver of the vehicle shall confirm that all personnel and riders are on-board, properly attired, with seat belts on, before the vehicle is permitted to move. This confirmation shall require a positive response from each rider." The International Association of Fire Chiefs (IAFC), Guide to IAFC Model Policies and Procedures for Emergency Vehicle Safety, states that "The driver shall not begin to move the vehicle until all passengers are seated and properly secured. All passengers shall remain seated and secured as long as the vehicle is in motion. Seat belts shall not be loosened or released while en route to dress or don equipment."23 NFPA 1901 Standard for Automotive Fire Apparatus, establishes requirements for the minimum length of seat belts, together with how they are measured. The standard also recommends that a seat belt warning device be installed to indicate when seat belts are not being properly used.20
The Commonwealth of Massachusetts exempts operators and passengers of fire vehicles from having to wear a seat belt.7 The fire department had not implemented a seat belt policy, and during the incident, the victim and three other fire fighters were not wearing their seat belts. Note: One fire fighter did buckle his seat belt seconds before the ladder truck made impact with the parked cars. Due to the severity of the fatal incident, a seat belt may not have saved the victim, but is recommended as a good safety practice.
Recommendation #8: Fire departments should develop policies and procedures that assist with determining specifications for new apparatus and replacement cycles of existing fire apparatus.
Discussion: NFPA 1901 Standard for Automotive Fire Apparatus defines the requirements for new automotive fire apparatus and trailers designed to be used under emergency conditions to transport personnel and equipment and to support the suppression of fires and mitigation of other hazardous situations.20 The standard provides guidance to fire departments that are looking to build and purchase a new fire apparatus. Fire departments could consider organizing a committee that would be responsible in the development and selection of a new apparatus. This committee could include individuals such as those involved with the maintenance of the apparatus, budgetary personnel, and union representation. This committee should look at the current and future needs of the department fleet, and consider things such as call volume, seasonal climate and weather, topography, and replacement cycles prior to finalizing a new apparatus for the fleet. The fire department wants to make sure new apparatus will last the allotted time provided by the department before having to be replaced according to the replacement cycle. Having to replace an apparatus prior to its scheduled cycle replacement can cause budgetary problems and disrupt plans for purchasing new and replacement apparatus.
It is a generally accepted fact that fire apparatus have a finite life, and in the fire service, there are fire apparatus with 8 to 10 years of service that are simply worn out.14 The length of that life depends on factors such as vehicle mileage, engine hours, preventative maintenance program, and driver/operator training. The ladder truck involved in this incident was 13 years old and had almost 14,000 registered engine hours and a last documented mileage on the ladder truck, more than three years prior to the incident, of almost 78,000 miles. Couple the age of the ladder truck and its' mileage and engine hours with deficiencies in the fire department's maintenance of the ladder truck, the apparatus perhaps should have been taken out-of service and replaced.
While it is important that fire departments seek constant improvements and upgrades to their fire apparatus and equipment through enhancements of their apparatus maintenance program and personnel training, some departments may not have the resources or programs to adequately maintain, upgrade, or replace their apparatus and equipment as often as they should. Alternative funding sources, such as federal grants, are available to purchase fire apparatus and equipment. Additionally, there are organizations that can assist fire departments in researching, requesting, and writing grant applications.
Useful resources include:
- Federal Emergency Management Agency, Assistance to Firefighters Grant Program
- www.firegrantsupport.com
- Federal Emergency Management Agency grants are awarded to fire departments to enhance their ability to protect the public and fire service personnel from fire and related hazards. This Web site offers resources to help fire departments prepare and submit grant requests.
- FireGrantsHelp.com
- www.firegrantshelp.com
- A nongovernmental group, FireGrantsHelp.com provides an extensive database of information on federal, state, local, and corporate grant opportunities for first responders. The primary goal of the Assistance to Fire Fighters Grant (AFG) Program is to provide critically needed resources such as emergency vehicles and apparatus, equipment, protective gear, training for responders, and other needs to help fire departments protect the public and emergency workers from fire and related hazards. The Grant Programs Directorate of FEMA administers the grants in cooperation with the United States Fire Administration.
Recommendation #9: Fire departments and fleet maintenance divisions should understand that the manual adjustment of automatic slack adjusters, a mechanical component of the air brake system that adjust brakes as necessary when the vehicle is in operation, may contribute to unexpected brake failure.
Discussion: An automatic slack adjuster (ASA) is a mechanical component of the air brake system that adjusts brakes as necessary when the vehicle is in operation to compensate for wear in the brake shoes (drum brakes) or pads (disc brakes). When an ASA is found to be out of adjustment, it signifies the existence of a larger braking system problem that needs correction, and the apparatus should be taken out-of-service immediately. The ASA should not be manually adjusted as it may cause wear on the ASA itself and give the driver a false sense of security that the brakes are working efficiently. This was first reported by the National Transportation Safety Board (NTSB) following their 2003 investigation into a fatal incident involving a dump truck and four passenger cars.10 The report stated that mechanics who worked on the dump truck manually adjusted ASAs without looking for an underlying brake problem, and possibly misdiagnosed why the brakes were not staying in adjustment. The NTSB investigation also determined the lack of readily available information on ASAs, inadequately maintained brakes, lack of owner oversight, and an untrained driver contributed to the incident.10
In 2006, the NTSB report was released and the IAFC released a lessons learned24 article to the fire service. During the NIOSH investigation it was discovered through interviews and documented apparatus sheets that the ladder truck in this incident was repeatedly having its brakes adjusted, even after recently performed brake jobs. It has not been determined beyond a reasonable doubt that the ASAs failed to work properly on the day of the fatal incident, but adjusting ASAs was a maintenance practice performed by fire department fleet maintenance personnel to troubleshoot brakes that were out of adjustment.
During the course of the investigation, NIOSH developed a Safety Advisory1 to notify the fire service to take immediate steps to ensure that automatic slack adjusters are not manually adjusted and to establish procedures to ensure apparatus maintenance is conducted by qualified technicians following recommended guidelines of the National Fire Protection Association.
Recommendation #10: Governing municipalities (federal, state, regional, and local) should consider enacting legislation to include operators and occupants of fire department vehicles in existing seat belt legislation and/or repeal existing laws that exempt drivers and occupants of fire service vehicles from mandatory seat belt use.
Discussion: Vehicle crashes are consistently the second leading cause of fire fighter line-of-duty deaths.21 The Commonwealth of Massachusetts does not require seat belt use by operators and occupants of fire department vehicles and apparatus. The FMCSA also exempts the occupants of fire trucks and rescue vehicles while involved in emergency and related operations from wearing seat belts. These laws are not consistent with NFPA standards, and IAFC and IAFF recommendations as mentioned previously. 15, 22, 23 Governing entities should consider enacting legislation that requires seat belt use by drivers and occupants of fire department vehicles and apparatus.
REFERENCES
- NIOSH [2009]. NIOSH Safety Advisory: manual adjustment of automatic slack adjusters may contribute to unexpected brake failure on automotive fire apparatus. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2010-102 [http://www.cdc.gov/niosh/docs/2010-102/]. (Link Updated 1/15/2013)
- VFIS [2008]. Emergency vehicle driver training. York, PA: Volunteer Firemen's Insurance Services, Inc.
- NFPA [2009]. NFPA 1002 Standard for fire apparatus driver/operator professional qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- National Institute for Automotive Service Excellence. [https://www.ase.com/Home.aspx]. (Link Updated 4/9/2013)
- NFPA [2006]. NFPA 1071 Standard for emergency vehicle technician professional qualifications. 2006 ed. Quincy, MA: National Fire Protection Association.
- Fire Department [1995]. Aerial ladder procurement specifications.
- Massachusetts Registry of Motor Vehicles [2009]. Commonwealth of Massachusetts driver's manual. Boston, MA. Date accessed: October 2009. [http://www.massrmv.com/rmv/dmanual/index.htm]. (Link updated 4/9/2013)
- Massachusetts Registry of Motor Vehicles [2009]. Commonwealth of Massachusetts commercial driver's license manual. Boston, MA. Date accessed: October 2009. [http://www.massrmv.com/rmv/cdlmanual/index.htm]. (Link updated 4/9/2013)
- Code of Federal Regulations [2003]. 49 CFR 571.121. Air brake systems. Washington, DC: U.S. Printing Office, Office of the Federal Register. Date accessed: July 2009. [http://www.gpo.gov/fdsys/pkg/CFR-2003-title49-vol5/pdf/CFR-2003-title49-vol5-sec571-121.pdf]. (Link Updated 1/17/2013)
- NTSB [2006]. Collision between a Ford dump truck and four passenger cars, Glen Rock, PA, April 11, 2003. Washington, DC: National Transportation Safety Board, NTSB Report Number HAR-06/01.
- Craven and Associates [2009]. Special report for the ___ fire fighters local ___. (Report requested by fire department union.)
- CMVSC [2009]. CMVSC-09-VA-092: Fire department ladder __ motor vehicle autopsy investigation report. Comprehensive Motor Vehicle Services and Consulting. (report requested by local police department.)
- Mercury Associates [2009]. Report on maintenance practices assessment for the ___ fire department. Gaithersburg, MD. Date accessed: March 2009. [http://www.cityofboston.gov/Images_Documents/Final%20Report%20on%20BFD%20Fleet%20Maintenance%20Practices%20Assessment_tcm3-4016.pdf]. (Report requested by the local fire commissioner.) (Link updated 5/13/2015)
- NFPA [2007]. NFPA 1911 Standard for the inspection, maintenance, testing, and retirement of in-service automotive fire apparatus. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 Standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- IFSTA [2000]. Aerial apparatus driver/operator handbook. 1st ed. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- The Commercial Motor Vehicle Safety Act of 1986. [http://www.aamva.org/NR/rdonlyres/751BBDAF-1DD6-48CC-B65D-9F4F2FA17AEF/0/CommercialMotorVehicleSafetyActCMVSA.pdf]. Date accessed: October 2009. (Link no longer available 12/6/2012)
- CVSA [2009]. Operation Air Brake. Commercial Vehicle Safety Alliance. [http://www.cvsa.org/programs/op_airbrake.aspx] Date accessed: October 2009.
- NFPA [2007]. NFPA 1451 Standard for a fire vehicle operations training program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2003]. NFPA 1901 Standard for automotive fire apparatus. 2003 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. Fire fighter fatalities in the United States - 2008. Quincy, MA: National Fire Protection Association.
- IAFF [2008] International Association of Fire Fighters, Fire Department Standard Operating Procedure, Fire Department Vehicle Safety, Emergency and Non-Emergency Response, Safety Emergency Operations on Roadways. [http://www.iaff.org/hs/evsp/vehicle%20Safety%20SOP.pdf] Date accessed: October 2009. (Link Updated 1/17/2013)
- Guide to IAFC Model Policies and Procedures for Emergency Vehicle Safety. [http://www.iafc.org/files/1SAFEhealthSHS/VehclSafety_IAFCpolAndProceds.pdf]. Date accessed: October 2009. (Link updated 10/28/2013)
- IAFC [2006]. Lessons learned from a fatal crash: Truck air brake warning: Manually adjusting automatic slack adjusters is dangerous, can lead to deadly consequences. Fairfax, VA: International Association of Fire Chiefs, Article on Website. Date accessed: September 2009. [http://www.iafc.org/files/onscene/pdfs2006/onscene061506.pdf#page=2]. (Link Updated 1/17/2013)
- Emergency Vehicle Technicians Certification Commission. [http://www.evtcc.org].
INVESTIGATOR INFORMATION
This incident was investigated by Jay Tarley and Stacy C. Wertman, Safety and Occupational Health Specialists, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. Stephen Wilde, a fire apparatus maintenance expert with Certified Fleet Service of Illinois was contracted by NIOSH to perform an apparatus inspection of the ladder truck. He has 35 years of experience as a mechanic, is a Master Certified EVT, chairs NFPA 1071, and sits on committees for NFPA 1901 and 1911. He is also the president of the Emergency Vehicle Technician Certification Commission.25 The report was authored by Stacy C. Wertman. A technical review was provided by William Peters, of Peters Associates, Fire Apparatus Consulting Services, Inc. Mr. Peters is a retired Battalion Chief with over 28 years experience with the Jersey City, New Jersey Fire Department and is active in the National Fire Protection Association (NFPA) consensus standards process.
DISCLAIMER
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
Summary of Apparatus Inspection and Findings from Stephen Wilde
For a copy of the complete apparatus inspection and findings report, contact
NIOSH Fire Fighter Fatality Investigation and Prevention Program
304-285-5916
On February 3, 2009, the NIOSH investigators and consultant were transported to a secured facility to inspect the ladder truck. The inspection began at the rear axle by checking the air brake system (ABS) modulator and relay valves for signs of oil. The rear ABS valves did not show signs of oil contamination. The rear relay valve showed slight signs of oil contamination. The rear air tanks had been drained, but still had oil in them. Pictures viewed from the police’s investigation showed an abundance of oil drained from the multiple air tanks. The treadle valve supply lines in the cab had been cut for removal of the valve and oil was found inside the lines. While in the cab, the consultant noticed the air gauge and hour meters had been removed prior to his inspection. The transmission electronic control unit and WABCO® ABS computers were still in the cab. The retarder switch was in the activated position, and the seat belts were still intact.
The consultant then focused on the braking system components. Both rear spring brake chambers had been “caged” (spring brakes pulled off with caging bolts to release spring brakes), and the left rear automatic slack adjuster (ASA), s-cam, brake shoes and drum had been removed prior to his inspection. The right rear brake shoes and drum had also been removed. Note: The rear braking system components had been removed and secured by the police department prior to the NIOSH inspection. The rear brake components were later inspected at the local police department headquarters. The consultant looked at the brake chambers, which appeared to be the wrong size. He found 30 service/36 spring brake chambers on the unit, which should have been 36 service/36 spring brake chambers. Having incorrect or mix-matched sized brake chambers may affect the overall braking ability of the apparatus. Note: Following this initial inspection, the consultant was able to briefly inspect another department ladder truck purchased at the same time as the ladder truck involved in the fatal incident, and found that the rear chambers on this unit were 36 service/36 spring brake chambers, the rear brakes looked like they had recently been changed.
Upon proceeding to the front to check the front brakes, it appeared that neither front brake had been disassembled. The front air tank could not be checked for oil, because the petcock on the bottom of the tank had been sheared off during the incident. The front drop frame brackets, bumper, steering gear mount and steering gear were damaged and had been removed. The front axle spring mount fasteners were broken. Upon examination of the front rotors, both left and right front rotors had slight heat cracks (normal wear), but showed no signs of overheating.
The consultant stated, “If the front brakes had been working properly we should have seen the front rotors overheat and turn blue as they tried to stop L26 on the way down the hill. Also, the reported loss of the left rear brake would have caused the two front brakes to do more braking than they were designed for, thus overheating the rotors. However, we did not see signs of overheating.”
The NIOSH consultant examined the left and right front ASA adjusting nuts to see if the brake adjustment (free play) had been checked. He found the ASA adjusting nuts had not been moved and the caliper lock pin nuts on both front wheels had not been removed. These findings indicated that the front brakes had not been disassembled as part of the police’s investigation. He asked the detective in charge if he could come back on February 4, 2009 and disassemble the front brakes to inspect the pads. Permission was granted from the local district attorney’s office. The department’s maintenance facility was also visited and all maintenance records for the ladder truck were obtained.
On February 4, 2009, NIOSH investigators and the consultant were allowed to disassemble the front brakes at the secured facility. Arrangements were made with motor squad personnel to meet us at the secured facility with tools so the consultant could remove the front wheels and disassemble the front brakes. He started with the right front brake. The brake caliper mounting, pads, rotor, chamber and ASA were examined prior to disassembly. There was little evidence of lubrication. The inner brake pad was resting on the caliper torque plate. The pads were not excessively worn as indicated by the amount of caliper pin protruding from the inner caliper mount. The rotors did not show signs of overheating, but did have slight heat stress cracks, which would be considered normal. He checked the ASA clevis pins to see if they were binding in the bore, which they were not. He found no evidence that the right front brake had been disassembled or that the free stroke had been checked during the initial accident investigation. The free stroke on the right front ASA was checked and found to be within the allowable .075 inch to .0875 inch range. This finding indicated that the right front brake adjustment was correct and the ASA was within the proper adjustment. He removed the upper caliper lock pin nut and removed the upper caliper pin. The lock pin retaining nut was not as tight as it should have been and the pin came out freely. He removed the air line to the brake chamber and cut the tie wraps on the ABS sensor wire. He moved the caliper off the rotor, allowing it to pivot on the lower pin, exposing the face of the pads and rotor. The face of the inner pad had some rust on it, as did the inner face of the rotor. This would indicate that the inner pad was not braking as much as the outer pad, which had only a slight amount of rust on the rotor surface. He saw the torque plate and the inner pad were gouged where the inner pad was resting on the torque plate; this would indicate that the inner pad had been resting on the torque plate for some time. He then removed the outer pad from the caliper, and the pad had one lateral crack from the bottom of the pad to the top, with minor spider heat cracks. The inner pad had two lateral cracks similar to the outside pad from the bottom to the top of the pad. The face of the inner pad was rust colored, which indicated that it did not do much braking. Neither pad appeared to be the recommended manufacturer’s pad, nor correct friction content pad for use on fire apparatus due to the long lateral cracks. He measured the rotor thickness for wear. The rotor was not worn beyond the minimum thickness. Since the rotors were not replaced (according to vendor paper work) during the last brake job and the pads were changed, he concluded that the pads were not the correct hardness. Note: Normally, when the correct hardness pads are used, the rotors wear at the same rate as the pads, so the rotors would have to be changed at every brake pad replacement. If the rotor is harder than the pads, the rotor will not wear at the same rate and the braking efficiency will be reduced. He reassembled the right side brake and reinstalled the wheel.
Next, the left front wheel was removed and the left front brake system was examined. The inner pad was found to be resting on the torque plate in the same location as the right side. The pads were worn similar to the right side. The rotors did not show signs of overheating, but did have slight heat stress cracks, which would be considered normal. He checked the ASA clevis pins to see if they were binding in the bore and he found the large pin would not turn freely. He found no evidence that the left front brake had been disassembled or that the free stroke had been checked during the police’s investigation. The free stroke on the left front ASA was checked and found to be .055 inch which is less than the required .075 inch to .0875 inch range. This would indicate that the left front ASA was over adjusting. Note: Several problems can cause the ASA to over adjust; (1) the initial setup of the ASA could have been incorrect; (2) the binding clevis pin could have caused over adjusting; or (3) the caliper might not be returning properly. These findings would normally have caused the left front brake to brake more than the right, causing a pull to the left during braking, and the left front rotor would show signs of overheating.
Upon removing the upper caliper lock pin nut and the upper caliper pin, it was discovered that the lock pin retaining nut was not tight; the pin came out freely and the pin showed signs of moving in the torque plate. The gouges in the pin lock area could have been caused by the loose lock pin retaining nut or if the caliper pins had not been changed at the last pad replacement. Note: The vendor paper work for the last pad replacement did not show caliper pin kits. Normally, caliper slide pins are changed when pads are changed. He removed the air line to the brake chamber and cut the tie wraps on the ABS sensor wire. He moved the caliper off the rotor allowing it to pivot on the lower pin, exposing the face of the pads and rotor. The face of the inner pad had some rust on it as did the inner face of the rotor. As with the right side, this would indicate that the inner pad was not braking as much as the outer pad, which had only a slight amount of rust on the rotor surface. He observed that the torque plate and the inner pad were gouged where the inner pad was resting on the torque plate; this would indicate that the inner pad had been resting on the torque plate for some time. The rotor hub showed signs of the outer pad riding on the hub. The outside pad had a bent and loose caliper retaining bracket. This allowed the pad to move in the caliper slide area enough to move down and rub on the rotor hub. The caliper holding area of the pad was damaged and the pad was loose in the caliper slide area. He then removed the outer pad from the caliper; the pad had two lateral cracks from the bottom of the pad to the top. The inner pad had two lateral cracks similar to the outside pad from the bottom to the top of the pad. The face of the inner pad was rust colored and did not appear to be doing much braking. Neither pad appeared to be the manufacturer’s recommended pad, or correct friction content for fire apparatus. The inner pad retaining bracket was loose and bent, and the slide pad area was damaged. He measured the rotor and the rotor was not worn beyond the minimum thickness. As with the right side, he concluded that the pads were not the correct friction content due to the lack of rotor wear. He reassembled the left side brakes and reinstalled the wheel. He also confirmed his findings from February 3, 2009, that the rear brake chambers were 30 service and 36 spring brake chambers.
On February 5, 2009, NIOSH investigators and the consultant received permission to view the brake system components that had been removed and secured by police investigators prior to our investigation. NIOSH investigators and the consultant went to the police department’s evidence lockup and began an inspection of the rear brake shoes, drums, left rear cam shaft and left rear ASA. The left rear drum was completely rusted with rust flaking off the braking surface. This indicated that the brake linings were not touching the drum on the left rear wheel. He inspected the left upper and lower brake linings and found gouges in the surface of the shoes from the flaking rust in the drum. These findings indicated that the left rear brake linings were not contacting the drum for some time. In other words, the left rear brake was not working, so there was no braking being done by that wheel. The cause of the left rear brake not working could be a defective left rear ASA, incorrect brake adjustment, incorrect chamber rod length, or defective brake chamber. The vehicle autopsy reported that the left rear ASA was disassembled and inspected, and found to have a damaged pull pawl, but the ASA was functional.12 The damaged pull pawl would only disable the automatic adjusting feature of the ASA and not cause the ASA to not function.12
The NIOSH consultant measured the thickness of the brake linings in multiple locations on the anchor pin side, in the center and on the roller side. The left side linings were slightly thicker then the right which would be expected due to the left brake not working and the right working. The lining friction content markings were not visible on the right or left linings, but due to the lack of significant heat cracks or even overheating of the right drum, the linings and drums might not be the correct ones for the fire apparatus. The consultant stated he would have expected to see much more wear and overheating on the right rear brake linings since the left rear was not braking at all. Because the left rear brake was not working at all, the reported skid marks at the accident scene could not have been made by the left rear tires.
No free stroke measurement is listed in the autopsy report for the left rear brake. In the autopsy report, the adjusted chamber stroke measurement for the left rear brake is reported as .808 inch.12 Because the free stroke was not measured prior to disassembly and there is no starting or ending measurements for the adjusted chamber stroke given, there is not a clear picture of what was wrong with the left rear brake system. The measurements would have told us if the chamber was in the fully retracted (released position) or if the chamber rod had been pulled out of the chamber due to an incorrect adjustment procedure of the ASA. It is possible to turn the ASA in the wrong direction, if the lock pawl has been removed or disengaged far enough to seat the s-cam against the rollers. If the ASA is turned farther, it will pull the chamber rod out of the chamber. If the ASA adjustment is left in this position, it will reduce the amount of travel the chamber can push the ASA. This will reduce the amount of s-cam rotation and reduce the travel of the shoes out toward the drum. In other words, the brakes are backed off and the shoes will be at the maximum distance away from the drums instead of the required minimum distance from the drums. When air is applied to the service side of the chamber and the rod has been pulled out of the chamber by an incorrect brake adjustment, the full stroke of the chamber will not be available to move the ASA the required 2 inch. The required free stroke of .500 inches places the shoes at the correct distance from the face of the drum, so there is no “brake drag,” but still allows maximum lining force against the drum face. Increased free stroke indicates the brakes are out of adjustment and the shoes have to travel farther to contact the drums, thus reducing braking force. Another possible cause for the reduced adjusted chamber stroke could be that the ASA clevis fork was installed incorrectly on the chamber push rod. The clevis fork adjustment is how the ASA initial setup is obtained during installation. For the ASA to properly adjust for brake wear automatically, the initial setup angle must be correct. After adjustment of the clevis fork, if the chamber push rod protrudes farther then .125 inches, the rod must be cut off. If the rod protrudes through the clevis fork more then .125 inches and is not cut off, the rod will contact the ASA body. When the chamber pushes the rod out, the rod tip will mechanically lock on the ASA body, stopping the chamber rod from reaching the proper stroke. If the report had listed the free stroke and adjusted chamber stroke starting and ending measurements, that could have helped determine what reduced the left ASA stroke.
Regarding the right rear brake system, the autopsy report listed an adjusted chamber stroke of 1.597" which is less then the required 2" for a # 30 brake chamber. As above, the autopsy report does not list the free stroke or adjusted chamber stroke starting or ending measurements, so we do not know why the adjusted chamber stroke was not correct. We can deduce that the right rear brake was not braking properly because of the reduced stroke. We can apply the same reasoning from the left side to the right. The difference being that the right side brake shoes were contacting the drums thus providing some braking force. The incorrect adjusted chamber stroke measurements from the autopsy report indicate serious issues with both rear ASA brake adjustments and operation.
Suggested items by the NIOSH consultant to implement:
- implement driver training program or CDL program
- use of certified emergency vehicle technician(s) (EVT)
- follow proper maintenance procedures
- document maintenance, repairs, and testing
- perform daily operational checks
- implementation of a formal written system to report problems from stations to maintenance personnel
- implement quarterly, semiannually, and annually preventive maintenance inspections
- review outside vendor qualifications and check required certifications
- utilize NFPA 1911 recommendations for testing and preventive maintenance
- implement NFPA 1911 “out of service” criteria
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency's recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit
the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 03/08/2010.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research