


Career Lieutenant Dies Following Floor Collapse into Basement Fire and a Career Fire Fighter Dies Attempting to Rescue the Career Lieutenant New York
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2009-23 Date Released: March 19, 2010
Revised on November 17, 2010
Revised on June 23, 2014 to add Protective Clothing Report Findings
SUMMARY
On August 24, 2009, a 45-year-old male career lieutenant (Victim #1) died following a partial floor collapse into a basement fire, and a 34-year-old male career fire fighter (Victim #2) was fatally injured while attempting to rescue Victim #1. The career fire department was dispatched for an alarm of fire with reported civilian(s) entrapment. Arriving units discovered a heavily secured mixed commercial/residential structure with smoke showing. Following failed initial attempts to locate an entry to the basement, crews located a door on Side 2 that provided access down a flight of stairs to a basement entry door. Repeated attempts were made to force open this basement door in order to search for trapped civilians, but crews had difficulty gaining access through this door because it was made of steel and locked and dead-bolted on both sides. Other crews on scene performed primary searches of the 1st and 2nd floors with no civilians found.

|
Incident scene. |
Approximately 30 minutes into the basement fire, command ordered all interior crews to exit the structure to regroup because crews were still unable to gain access into the basement from Side 2. Additional manpower was sent with special tools to assist in breaching the basement door on Side 2. Victim #1 and two fire fighters from his crew entered into the structure from Side 1 to verify all fire fighters had exited a 1st floor deli. Victim #1, following a hoseline into the structure, was well ahead of the other two fire fighters when the 1st floor partially collapsed beneath him. Victim #1 fell with the floor into the basement, exposing him to the basement fire. The other two fire fighters immediately exited the deli after fire conditions quickly changed and shelving and displays fell on them; they were unaware of what had just occurred. Victim #1 made several Mayday calls from within the structure and activated his PASS device. Confusion erupted exteriorly on scene when trying to verify who was calling the Mayday, their exact location, and how they got into the basement. The incident commander was aware that he had crews attempting to gain access into the basement from Side 2 but was unaware that there had been a floor collapse within the deli section of the structure. Simultaneously, Victim #2, a member of the fire fighter assistance and search team (FAST), was standing by outside Victim #1s point of entry when the Mayday calls came out. It is believed that Victim #2 knew where Victim #1 was since he had gone in the structure with him earlier in the incident. Victim #2 grabbed a tool, went on air, and rushed into the structure. The FAST and additional personnel on scene concentrated on Side 2 initially while other fire fighters followed an unmanned hoseline into the deli. Crews within the deli quickly discovered a floor collapse and reported hearing a PASS device alarming. Victim #1 was immediately identified as missing during the first accountability check, but Victim #2 was not accounted for as missing until the third accountability check, more than 50 minutes after Victim #1s Mayday. After the fire was controlled, both victims were discovered side-by-side in the basement where the 1st floor had partially collapsed. They were found without their facepieces on and with SCBA bottles empty. Victim #1s PASS device was still alarming. They were pronounced dead on scene. Four fire fighters and one lieutenant suffered minor injuries during the incident. No civilians were discovered within the structure.
Key contributing factors identified in this investigation include working above an uncontrolled, free-burning basement fire; interior condition reports not communicated to command; inadequate risk-versus-gain assessments; and, crew integrity not maintained.
NIOSH has concluded that, to minimize the risk of similar occurrences, fire departments should:
- Ensure that all personnel are aware of the dangers of working above a fire, especially a basement fire, and develop, implement, and enforce a standard operating procedure (SOP) that addresses strategies and tactics for this type of fire.
- Ensure that the incident commander (IC) receives interior status reports and performs/continues evaluating risk-versus-gain.
- Ensure that crew integrity is maintained at all times on the fireground.
- Ensure that the incident commander (IC) receives accurate personnel accountability reports (PAR) so that he can account for all personnel operating at an incident.
- Ensure that a separate incident safety officer, independent from the incident commander, is appointed at each structure fire.
- Ensure that fire fighters use their self-contained breathing apparatus (SCBA) and are trained in SCBA emergency procedures.
Additionally, manufacturers, equipment designers, and researchers should:
- Conduct research into refining existing and developing new technologies to track the movement of fire fighters inside structures.
- Continue to develop and refine durable, easy-to-use radio systems to enhance verbal and radio communication in conjunction with properly worn self-contained breathing apparatus (SCBA).
INTRODUCTION
On August 24, 2009, a 45-year-old male career lieutenant (Victim #1) died following a floor collapse into a basement fire, and a 34-year-old male career fire fighter (Victim #2) was fatally injured while attempting to rescue Victim #1. On August 24, 2009, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On August 31-September 3, 2009, a safety and occupational health specialist and a general engineer from the NIOSH Fire Fighter Fatality Investigation and Prevention Program investigated this incident. The NIOSH investigators met with the fire commissioner; fire department staff involved with the internal investigation; union representatives; a safety and health inspector with the New York State Department of Labor; representatives from the citys Department of Economic Development, Permit, and Inspection Services; the citys fire marshal; and representatives from the fire departments training and fire prevention divisions. Interviews were conducted with the incident commander, fire incident operations chief, the fire departments chief of training, and lead fire investigator for the fatal incident. NIOSH investigators inspected the victims SCBA, personal protective equipment (PPE), and hand-held radios and reviewed incident scene photographs taken by a police photographer. NIOSH investigators obtained and reviewed the fire departments standard operating procedures (SOPs), victims and incident commanders training records, first line supervisor training program, fire training curriculum, radio transcripts from the incident, and city building inspection and code files for the fire structure. NIOSH investigators also visited the incident site, but the fire structure had already been demolished.
The NIOSH investigators returned September 12-17, 2009, to conduct interviews with fire fighters and officers involved with the initial incident response and those involved with the initial rescue and the recovery of the victims. The investigators met with personnel with the Federal Bureau of Alcohol, Tobacco, and Firearms local office; local news stations; and the medical examiners office. The investigators also reviewed additional photos obtained from the public, raw video footage, medical examiners reports, SCBA inspection and fit testing reports for the victims, and current investigative findings from the fire departments internal fire investigations unit. At the request of the fire department, the victims SCBAs were examined by NIOSHs National Personal Protective Technology Laboratory (NPPTL) to determine conformity to the NIOSH-approved configuration, and the victims personal protective equipment (PPE) were also examined to determine conformity to the National Fire Protection Association national consensus standards. Preliminary information provided from NPPTL to NIOSH investigators suggests that the SCBAs and/or PPE evaluated had no direct contribution to the deaths of the two fire fighters. When finalized, summaries of the SCBA and PPE evaluations will be added as appendices to this report.
FIRE DEPARTMENT
This career fire department has 19 stations with 675 uniformed members who serve a population of approximately 290,000 within an area of about 42 square miles. The fire department consists of one division separated into four battalions, which are further separated into four platoons. Each platoon will work two day shifts (0800-1700) followed by two night shifts (1700-0800). The department has a Chief of Safety who is designated as the incident safety officer (ISO) that works four 10 hour shifts (0700-1700 Monday-Thursdays). This position may respond to any incident during the duty shift. After hours, this position only responds when paged out for incidents such as hazardous materials, 2nd alarm fires, high-rise incidents, and technical rescue. The IC will assume the duties of the ISO when needed for other incident responses or until the ISO arrives. If the ISO is away on leave then arrangements are made to fill the ISO position with other chief officers.
The fire department has written SOPs covering incident command, accountability, common fireground guidelines, special fireground operations, special operations/technical rescue, large-diameter hose, emergency vehicle operations, and communications. These SOPs do not specifically address the hazards of basement fires or working above a fire. The fire department uses a helmet front passport system and personal accountability tags to maintain personnel accountability during incidents. The fire department identifies the sides of a structure numerically (e.g., Side 1 (front) and clockwise, Side 2, Side 3, Side 4).
TRAINING and EXPERIENCE
Victim #1 had been with this department for more than 22 years. He had been a lieutenant for approximately 12 years. He had completed over 2,200 documented hours of training on topics including firefighting essentials, fire behavior, ladder company operations, structural collapse, fire attack, hazardous materials, special operations, and rescue. He had also completed the departments first-line supervisor training program, which consisted of over 120 hours of training on topics such as fire department management, operations and tactics, outside agency response, building construction and collapse, and fire instructor.
Victim #2 had been with this department for more than 10 years as a fire fighter. He had completed over 800 documented hours of training on topics including basic and intermediate fire fighting, fire behavior, ladder company operations, and hazardous materials.
The initial arriving incident commander (IC) had been with this department for more than 27 years and had held the rank of battalion chief for the last 10 years. He had completed over 1,700 documented hours of training on topics including incident safety officer, fire origin, cause and behavior, incident management, ladder company operations, fire fighting essentials, and fire department management and operations. He had also completed the departments first-line supervisor training program, which consisted of over 120 hours training on topics such as fire department management, operations and tactics, outside agency response, building construction and collapse, and fire instructor.
The IC for the core of the incident had been with this department for more than 25 years and had held his current rank of division chief for the last year. He had been a command officer for the last 17 years. He had completed over 1,600 documented hours of training on topics including hazardous materials, fire officer, fire fighter survival, initial fire attack, ladder company operations, fire behavior, and fire fighting essentials. He was certified as a fire instructor for the state of New York. He had also completed the departments first-line supervisor training program, which consisted of over 120 hours training on topics such as fire department management, operations and tactics, outside agency response, building construction and collapse, and fire instructor.
This department operates their own fire academy that exceeds the minimum standards for fire fighting personnel set forth by the state of New York. Individuals are hired and must complete all aspects of the fire academy training prior to being certified as a fire fighter and released to the field. Fire fighter recruits receive 440 hours of in-house training and hands-on evolutions. Both victims had graduated from the departments fire academy. The department also provides 100 hours of annual refresher training to their fire fighters and officers on topics such as strategies and tactics, hazardous materials, radio communications, forcible entry, personnel safety, and detection and suppression. The department also provides specific training to members involved with FAST operations. Victim #2 had completed FAST training prior to this incident.
EQUIPMENT and PERSONNEL
1st Alarm Assignment:
- Engine 31 (E31) with three fire fighters and a lieutenant
- Engine 22 (E22) with three fire fighters and a lieutenant
- Engine 23 (E23) with three fire fighters and a lieutenant
- Ladder 14 (L14) with three fire fighters and a lieutenant
- Ladder 6 (L6) with three fire fighters and a lieutenant
- Rescue 1 (R1) with four fire fighters and a lieutenant (Victim #1)
- Ladder 7 (L7) with two fire fighters, a call-in fire fighter (Victim #2), and a lieutenant—FAST
- Battalion Chief 43 (B43)—initial IC
- Division Chief 56 (B56)—assumed IC upon arrival
Note: See Diagram 1 for incident scene and hoselines deployed.
2nd Alarm Assignment:
- Engine 33 (E33) with three fire fighters and a lieutenant
- Engine 28 (E28) with three fire fighters and a captain
- Engine 21 (E21) with three fire fighters and an acting officer
- Ladder 2 (L2) with three fire fighters and a lieutenant
- Ladder 15 (L15) with three fire fighters and a lieutenant
- Battalion Chief 44 (B44)
- Battalion Chief 41 (B41)—incident safety officer (arrived during rescue and recovery)
Note: Support units are not listed above for the 1st and 2nd alarm assignments.
TIMELINE
This timeline is provided to set out, to the extent possible, the sequence of events. Times are approximate and were obtained from review of the dispatch records, witness interviews, photographs of the scene and other available information. Some events may not have been included and many arrival times of units were not available. The timeline is not intended, nor should it be used, as a formal record of events.
- 0349.02 Hours
911 center receives a call for a fire inside a store - 0350.00 Hours
911 center receives a call from alarm company of motion detector going off in basement area. - 0350.35 Hours
911 center receives a call back from original caller stating, Someones inside. - 0351.36 Hours
911 center dispatches E31, E22, E23, L14, L6, R1, L7 (as FAST), and B43 for Alarm of fire, occupants still inside. - 0352.27 Hours
E31 en route from quarters and can see smoke and acknowledges report that people are trapped. - 0353.01 Hours
E31 arrives on scene and is met by unknown individual telling crew he heard people pounding and yelling on Side 2. - 0353.14 Hours
E31 officer advises dispatch they have reports from civilians of people trapped and there are steel gratings over doors and windows.
While en route to the scene, B43 requests an extra "2 and 1" to stage.
Note: "2 and 1" refers to two engines and one ladder truck, and these apparatus were part of the 2nd alarm assignment. - 0353.52 Hours
B56 en route. - 0354.04 Hours
Extra 2 and 1 dispatched that includes E33, E28, and L15. - 0354.57 Hours
L14 reports possible basement fire and heavy smoke visible. - 0355.31 Hours
B43 advises dispatch to have additional 2 and 1 stage at cross street. - 0356.32—0356.43 Hours
E31 reports to B43 with confirmed basement fire.
B43 acknowledges and arrives on scene taking initial command of the incident. - 0357.01 Hours
R1 personnel make entry onto 2nd floor to conduct a primary search. - 0357.59 Hours
B43 updates dispatch on description of structure, search and rescue operations on the 2nd floor, and entry operations on Side 2.
L7 (FAST) on location. - 0359.02 Hours
B56 arrives on scene. - 0359.23 Hours
Officer of E22, over radio, reports to B43 that a hoseline is being laid into basement and a second line is being laid in (second line laid in by E31). Note: The hoseline to the basement is only laid down a flight of stairs on Side 2 to the basement door. - 0400.30 Hourss
Radio transmission from R1, Looks like were moving right along three . - 0402.30 Hours
B56 assumes command and advises dispatch that there is no fire on the 1st floor or apartments, a 1¾-in line laid and in operation with two additional 1¾-in hoselines available, he will hold everyone he has on scene including the extra “2 and 1.”
B56 checks on location of E31. E31 advises B56 that they are in the basement.
Note: L14 is still trying to breach the basement door; door is partially opened at top. - 0404.37 Hours
B43 advises B56 that witnesses believe victims may be in the basement. - 0405.07 Hours
B56 advises R1 that civilians stated that they heard pounding on a door in the basement.
R1 advises B56 that the 2nd floor is negative and asks if the roof has been opened.
L6 advises bulkhead is open. - 0406.10 Hours
B56 checks on location of E22. E22 advises they are working on the 1st floor (rear apartment) and flowing water on fire on Side 4 of the structure.
L6 reports to B56 that chimney on roof is pushing smoke heavily. - 0406.32 Hours
B56 tells L6, Yeah, ok, I think we do have a basement fire I believe weve got 31 down in the basement. - 0407.05 Hours
B56 acknowledges radio transmission from Victim #1, Ok, you say you found the stairs to the basement, theyre where you thought they were in the rear of the 1st floor.
Note: Victim #1 was on the 1st floor inside the deli and his radio was on direct mode, which was a nonrepeated or recorded channel. Only radios scanning and within a certain radius of his radio could copy his transmission. It is suspected that Victim #2 is with Victim #1 at this time.
B43 asks, R1, do you have a camera with you—be careful that is clear, do what you can, but if it gets bad get out. Note: It is believed B43 is talking to Victim #1. - 0407.47 Hours
B56 checks on location of E23. E23 is working on 2nd floor. - 0409.15 Hours
L14 officer reports primary search of the 2nd floor is negative and that there is no fire extension to that area. - 0409.35 Hours
E22 asks for ventilation on the 1st floor. - 0409.50 Hours
B56 acknowledges E22 request for ventilation on 1st floor, and he advises E22 that he has E23 coming in Side 1 with a hoseline. Note: E23 was going to advance this hoseline to a believed basement interior door that Victim #1 had discovered while searching the deli. Victim #1 had already exited the deli from Side 1 and advised B56 that he heard people calling out and banging. The fire department believes that Victim #1 may have mistaken the crew of E22, who was working behind the coolers in the same area, as being trapped civilians. Witnesses state that Victim #1 assisted in redeploying E23s hoseline. - 0410.20 Hours
B56 requests L7 (FAST) to do what they can to ventilate the 1st floor. - 0411.01 Hours
Dispatch advises B56 that they are 20 minutes into the incident.
B56 advises dispatch that they are now operating three 1¾-in hoselines, performing an aggressive interior search, and we still have a report of civilians trapped we believe they may still be in the basement. - 0412.40 Hours
B56 repeats transmission from R1, Thats clear; youve got water on fire in the basement, still burning hot. Note: B56 was talking to Victim #1. It is believed he was spraying water into the basement from the deli floor through a burned-through area at the rear of the deli on Side 4. - 0413.36 Hours
B56 requests balance of 2nd alarm to stage on a cross street. - 0414.30 Hours
Dispatch dispatches balance of 2nd alarm: E21, L2, B41, and B44. - 0415.20 Hours
E22 radios B56 stating, Couldnt get door open in the basement. Everyone is coming out Side 2. - 0417.11 Hours
B56 advises dispatch that they are pulling all companies out of the 1st floor due to an inaccessible steel door on Side 2. - 0419.20—0420.26 Hours
Fire department reports that Victim #1, no longer with the E23 crew working within the deli, spoke to B56 in person regarding the interior conditions of the deli when he was with E23. B43 also meets with Victim #1 and B56 regarding conditions within the deli. - 0420.40—0421.01 Hours
B56 advises B43 that he is sending E31, E33, and L14 to basement door on Side 2 to force entry with a rabbit tool.
B43 copies B56 and advises him that the store owner has provided him with a key possibly to the basement door on Side 2. B43 advises B56 that conditions on the 1st floor (rear apartment) are deteriorating. - 0421.18 Hours
Last visual sighting of Victim #1 outside the structure.
At some point, Victim #1 re-enters the deli with R1 personnel to clear the deli. - 0421.22 Hours
B56 repeats B43s previous transmission for verification. The fire department dispatcher confirms 1st floor conditions are deteriorating per B43 and advises B56 that they are 30 minutes into the incident.
B56 acknowledges.
B56 checks on L14 and status of basement door on Side 2. Garbled response is heard from L14. - 0422.40 Hours
Believed time of partial floor collapse of 1st floor into basement. - 0423.06 Hours
B56 transmits over radio, Was that a Mayday? - 0423.07-0423.21 Hours
R1 transmits over radio, I believe I hear screaming in the front of the basement Side 1.
B43 transmits over radio, Whose yelling?
Several additional transmissions from B56 to Victim #1 attempting to verify location.
Victim #2 begins to enter the deli through Side 1, but is pushed back by exiting R1 personnel. - 0423.42 Hours
Victim #2 enters through the deli door. Note: This was viewed from raw video footage. - 0423.47 Hours
B56 splits rescue and fire operations to two different channels; B43 in charge of rescue.
B56 orders B43 to take the FAST to the basement Side 2. - 0424.22 Hours
A PASS alarm is heard from within the deli. - 0424.34 Hours
B56 contacts L14 to obtain update on what is happening in the basement on Side 2. Note: B56 believes that a fire fighter operating on Side 2 is his “Mayday victim.” B56 is unaware of the floor collapse within the deli. - 0426.58 Hours
B43 on radio states, to fire fighter in basement what is your last known location?
B56 on radio states, did you enter the basement from Side 1 or 2? - 0428.15 Hours
R1, on fire operations channel, states, fire fighter fell through 1st floor need water front of building. - 0428.56 Hours
Unknown transmission, on rescue channel, to B43 stating, 43 fire broke through, fire broke through. - 0429.34 Hours
R1 reports on fire operations channel, hear him (PASS device) 1st floor near the back; not sure if hes in basement or not. - 0431.02 Hours
B43 orders emergency head count from rescue channel. - 0431.06-0434.07 Hours
Companies confirm assigned personnel.
L7 (FAST) officer states status okay. Note: Victim #2 is not with other crew members of L7 (FAST).
R1 reports missing Victim #1. - 0434.42 Hours
B56 advises that he will stay in command, B43 will remain in charge of rescue operations, and B44 will take over incident operations. - 0435.08 Hours
R1 reports Victim #1 last seen going in Side 1, possibly into a hole 10 ft down. - 0436.09 Hours
B56 advises B43 that he has reports that our member may have dropped into the basement through a hole in the 1st floor. E21 is trying to get to him, but it is untenable.
Identity of Victim #1 verified by R1 members and dispatch’s roll sheet. - 0444.10 Hours
3rd alarm is dispatched. - 0447.20 Hours
All crews operating on 1st floor of deli are ordered out by B44. - 0451.01 Hours
Emergency head count ordered by B56.
L7 officer states, All okay. Note: Victim #2 is not with his crew. Fire becomes defensive with crews working on all sides on suppression and rescue/recovery operations. - 0457.39 Hours
Rescue/Recovery operations beginning on Side 4 by breaching through brick wall. - 0510.20 Hours
L7 officer over the radio states, fire fighter ____, your location.
Note: This is the first acknowledgement that Victim #2 may be missing. - 0511.09 Hours
L7 officer over radio states, Fire fighter ____, acknowledge. - 0511.53 Hours
Dispatch over radio states, Dispatch to fire fighter ____ of ladder 7, Dispatch to fire fighter ____, of ladder 7, acknowledge. - 0515.30 Hours
L7 officer over the radio states, Fire fighter ____ acknowledge your location anybody seen fire fighter ___.
Unknown individual transmits over radio, Hes got him here.
Note: The last names of Victim #2 and the other individual sound alike. - 0524.28 Hours
L7 officer over radio states, Fire fighter ____, acknowledge your presence. - 0525.08—0529.27 Hours
B56 asks dispatch to raise fire fighter ____ from ladder 7.
Dispatch advises, They found him 10 minutes ago.
Dispatch raises tones and asks for fire fighter ____ to acknowledge several times.
Dispatch notifies B56 of no response.
B56 contacts the officer of L7. - 0546.10 Hours
Crews re-enter the deli to assess collapse and debris. - 0547.44 Hours
Dispatch contacts B56 on the radio to see if Victim #2 had been located.
B56 advises they have not located Victim #2. - 0553.07 Hours
Crews within the deli are ordered out of the structure. - 0610.35-0614.05 Hours
B56 advises dispatch to perform a head count for the incident.
Dispatch performs head count.
L7 officer advises dispatch they are missing one (Victim #2). Note: His exact whereabouts unknown. - 0804.13 Hours
Rescue/Recovery operations initiated on Side 1 in conjunction with Side 4 operations. - 0918.36 Hours
Interior rescue/recovery crew on Side 1 from deli floor makes visual contact of two fire fighters. Confirmed as Victim #1 and Victim #2 in basement. - 0932.21 Hours
Hands on Victims #1 and #2. - 0939.12 Hours
Victim #1 and Victim #2 removed from structure.
PERSONAL PROTECTIVE EQUIPMENT
It was reported to NIOSH investigators that Victim #1 and Victim #2 were recovered wearing a full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, Nomex® hood, gloves, boots, and a self-contained breathing apparatus (SCBA). The turnout gears heat-resistant outer shells, moisture barriers, and insulating thermal linings were all present during the incident and documented during the investigation. Victim #1s PASS device was still alarming, but Victim #2s PASS device was not. Victim #1 was discovered with his Nomex® hood over his head and Victim #2 was discovered with his Nomex® hood rolled down on his neck; both victims were found without their helmets and facepieces on. Both victims face-mounted regulators were connected securely to the SCBAs assigned facepieces and were within arms reach. SCBA bottles were empty. Victim #1 was missing his left glove. Both victims were equipped with handheld radios and had various fire fighter hand tools in their pockets.
Due to the smoke conditions, both victims would have had to have been on air when entering the structure. It has not been determined why both victims were found without their facepieces on, but NIOSH investigators have theorized the following possibilities:
- Victim #1 removed his facepiece to transmit his “Mayday.”
- Both victims’ facepieces were unintentionally knocked off when falling into the basement.
- The facepieces were removed because they ran out-of-air or other emergency situation.
STRUCTURE
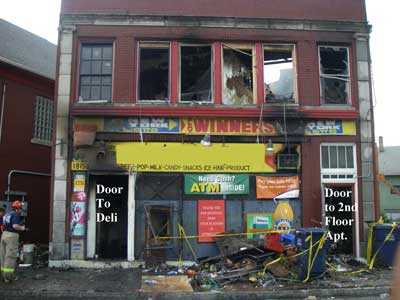
The incident occurred in a two and a one-half story structure with a one-story garage attached to the rear and an unfinished basement (see Photo 1). The fire structure and basement measured approximately 60 x 30 ft, and the attached garage measured 21 x 30 ft (see Diagrams 2 and 3). The structure had been upgraded over the years with a current layout consisting of a deli and separate apartment on the 1st floor (see Diagram 4) and two separate apartments on the 2nd floor (see Diagram 5). All apartments were vacant except the rear apartment on the 2nd floor. The exact dimensions and square footage of the deli and apartments were not available. On the 2nd floor, Side 2, the fire structure also had two enclosed walkways that connected to the Side 2 exposure.

|
Photo 1. Aerial view of the fire structure and connecting Side 2 exposure. The street facing apartment on the 2nd floor, which was directly above the deli, had a flat roof, but the rear apartment had a pitched roof with attic space; this was quickly identified during the initial size-up. |
The mixed commercial/residential, tax-payera type structure, built in 1934, was of ordinary construction consisting of wood floors and masonry/brick load bearing walls. The 2nd floor apartment located above the deli had a flat, membrane-type roof, but the rear apartment contained an attic constructed by conventional framing covered with wood planking and a slate roof. All exterior windows on the first floor and casement windows at the basement level had been bricked over for security purposes. There were two doors located on Side 1, 1st floor: one for the deli and one to access the stairway to the 2nd floor apartments (see Photo 2 & Diagram 1). The store front was protected by wire mesh and steel-grated doors/bars on the exterior and solid panels behind the plate glass store front (see Photo 3).
|
|
Photo 2. Doors located on Side 1 of structure. |

|
Photo 3. Close-up of secured store front showing security grating. |
aA commercial structure built of ordinary construction that is subdivided to hold various commercial occupancies; it is typically one story but may be two stories with apartments on the second floor.
There were two doors located on Side 2. Door #1, 40 ft from the corners of Side 1 and Side 2, was locked and protected by wire mesh and steel bars; Door #1 which once provided access into what is now the deli from the outside was now covered by a wall cooler within the deli (see Photo 4). Note: Building officials commented to NIOSH investigators that this type of occupancy only required one entry/egress point and extra entry/egress points that were no longer in use or covered up should be removed. Door #2, 60 ft from the corner of Side 1 and Side 2, was also locked, wire meshed, and covered with steel bars (see Photo 5). Once this door was opened, occupants of the structure could gain access to the 1st floor apartment, ascend a flight of stairs to the 2nd floor rear apartment, or descend a flight of stairs to access the basement door. Access to the basement was secured by a steel door, which was padlocked and dead-bolted both inside and out.

|
Photo 4. First door encountered by fire fighters on Side 2. |

|
Photo 5. Second door encountered by fire fighters on Side 2. |
The deli floor consisted of tongue-and-groove flooring covered by ceramic tile. Structural stability for the deli floor was maintained by joists that ran the length of the deli and two steel beams that ran perpendicular to the joists. The wood floor joists rested on the steel beams. The deli floor setup consisted of wall coolers lining the interior walls and display shelves placed throughout the deli space (see Photo 6). (Note: According to building officials, the dead load rating for the floor was 80 pounds per square foot, and it was not believed to have been over loaded at the time of the incident.) The basement contained excess stock for store operations, coolers, and other store/deli equipment (see Photos 7). The fire department conducts preplan inspection of occupied structures and recently implemented a hazard identification program of abandoned structures. The fire structure received yearly fire and health inspections. The origin of the fire is believed to be within the basement.

|
Photo 6. Interior view of deli following partial floor |
 |
 |
Photo 7 . Views of materials stored within basement. |
|
WEATHER
The weather at the time of the incident was clear with temperatures around 62°F. No wind conditions were reported.
INVESTIGATION
Note: The following investigative summary does not contain every event that occurred prior to the fatal incidents, but is intended to focus primarily on the actions taken by Victim #1 and Victim #2, initial search and rescue efforts for the reported entrapped civilian, and key 1st floor suppression activities and forcible entry operations into the basement prior to the fatal incident.
On August 24, 2009, between 0349-0351 hours, the local 911 center received several 911 calls from civilians reporting a basement fire with people entrapped. The initial 1st alarm included three engines, two ladder trucks, one rescue truck, a third ladder truck assigned as the FAST, one battalion chief, and one division chief. The first responding engine reported that they could see smoke in the air from their station and acknowledgement of reported people entrapped. B43 then requested extra companies (including two engines and a ladder truck) be dispatched to the incident. B56 took command upon his arrival and placed B43 in charge of operations. B43 initially concentrated on efforts already initiated on Side 2 with crews from E22, E31, and L14.
Activities on Side 2
E31 arrived first on scene, followed by L14 and then E22. All three companies heard the radio traffic regarding entrapped civilians and all observed smoke from the structure and no fire visible. E31 personnel were approached by two individuals advising them that the basement was on fire with people entrapped in it. E31 notified dispatch of smoke showing and people entrapped. The resident of the upstairs apartment escorted E31/L14 personnel to the first door (closest to the street side) on Side 2 and told them he heard people behind this door. E31 personnel never noticed any fire while assessing the structure; just smoke pushing from cracks around covered windows and an old coal chute on Side 2. E31 personnel retrieved a saw from E31 and stretched a 1¾-in hoseline to the alley on Side 2. E31 personnel used a saw to cut the steel gate on the exterior of the door. When finished, they were met with a steel door. They were not able to breach this door and discovered later that a wall cooler was placed directly behind the steel door. Note: This door was no longer in use, so the owner of the deli had placed a wall cooler in front of it to hide the door from within the store. E31 personnel then discovered a second door on Side 2, 20 ft down from the first door. This door was easily breached, giving crews access to the basement door, 1st floor rear apartment, and second floor rear apartment (see Photo 8). E22 personnel were also standing by to provide assistance. A second 1¾-in hoseline was retrieved from E31 and set up on Side 2. A crew from E31 advanced the initial 1¾-in hoseline through the second door on Side 2, down a flight of stairs to a bolted steel entry door that fire fighters presumed was to the basement to the fire structure.
B56 was advised at this point that they were advancing into the basement. No sounds from supposed trapped civilians were heard at this door. E31 requested assistance from L14 personnel to breach the basement door. The L14 crew split up to assist with gaining entry into the basement and to conduct a primary search of the 2nd floor. A fire fighter and the officer from L14 searched the 2nd floor rear apartment and crossed paths with the R1 crew. Their search was negative for civilians. L14 exited down a flight of stairs that led out to Side 1. During L14s search of the 2nd floor, a fire fighter from L14 performed a quick search of the 1st floor apartment where he discovered fire coming through the floor along the wall of Side 4. He notified B56 over the radio and he requested a hoseline into the 1st floor apartment by E22. E22 made entry into the 1st floor apartment with E31s second 1¾-in hoseline placed in the alley on Side 2. They were met with extreme heat conditions as if the fire was above them. They sprayed water on the ceiling and the room felt cooler. E22 noticed that Side 1 of this apartment was actually a row of coolers separating the apartment from the deli (see Photo 9).
 |
 |
Photos 8 and 9. Photo at left, shows the door that E22, E31, and L14 crews entered through. Personnel from E31 and L14 went down the stairs; the search crew for L14 went up the stairs, and the officer of L14 and crew from E22 made an immediate right to access the 1st floor apartment. Photo at right shows the wall of coolers that separated the deli and apartment. (Photos courtesy of police photographer.) |
|
E22 noticed a glow at the corner of Side 4 and Side 1 of the apartment and sprayed water for about 1 to 2 minutes before advancing toward the glow (see Diagram 6). E22 noticed that the floor was spongy and appeared to be getting weaker as they progressed toward the glow. Note: NIOSH investigators believe this information may not have made it to B56. One crew member from E22 stated during interviews that his hand went through the floor. They quickly backed out and advised the officer of E22 of what they found. The E22 crew went to Side 1 and changed their bottles. One of the members from this crew remembers changing a bottle for Victim #1. While E22 and the L14 search crews were inside the structure, thick, black smoke was observed pushing around a small window by the basement door and the door was hot to touch. Crews were able to partially push the steel basement door open at the top, allowing water to be flowed through it. The minimal access for water through this opening was insufficient to hit the seat of the fire. Conditions worsened as continued attempts to gain entry into the basement were unsuccessful; smoke thickened and conditions were extremely hot in the stairwell to the basement door. B43 decided to regroup and removed all E31 and L14 personnel from the basement stairwell to reevaluate their efforts. B56 ordered the search crew from L14, now on Side 1, to return to Side 2 and assist with entry into the basement; they retrieved a rabbit tool and headed back to Side 2. The deli owner also provided B43 a key, but it did not open the basement door. B43 went to the command post at the corner of Side 1 and Side 2 to speak with B56 regarding operations. Briefly following this, personnel on Side 2 observed what they thought was a flashover in the basement stairwell, followed by immediate screaming heard on the radio. B43 also heard the radio traffic and assigned the FAST to Side 2, thinking something had happened after he had stepped away from Side 2. B43 noticed that the smoke was now changing color and texture and was pushing out the coal chute and through many masonry cracks on Side 2. Crews were assigned to staff a 1¾-in hoseline down the basement stairs again in an effort to gain entry through the basement door and provide the FAST access. Their efforts were unsuccessful in gaining access through that door. Crews on Side 2 then initiated operations to insert a Bresnan distributor (a type of cellar nozzle used to combat basement fires) into the basement to suppress the basement fire. Note: The fire department did not initially use their Bresnan distributor (which uses steam conversion) to combat the basement fire in fear of injuring reported trapped civilians.
Activities of R1 on Side 1
R1 arrived on scene with four fire fighters and their officer (Victim #1). R1 members were met by the store owner, requesting them to cut the lock on the deli door and advising people may be trapped inside. R1 obtained a key to a door located at the corner of Side 1 and Side 4. This stairway led to the apartments on the second floor (see Diagram 5). Three fire fighters from R1 ascended the stairs to search the 2nd floor. Victim #1 and the remaining fire fighter from R1 gained access into the deli and performed a primary search of it. The R1 crew on the 2nd floor performed a primary search with a thermal imaging camera (TIC) of what was believed to be the rear apartment. Smoke conditions were light and then worsened with temperatures in the room increasing. The R1 crew broke windows for ventilation as they performed a left-handed search. Their search was negative for civilians and at some point they came upon members from L14 who were searching the rear apartment also. The R1 crew on the 2nd floor heard a radio transmission about possible civilians in the basement. The E23 crew, who had arrived on scene shortly after R1, had taken a third 1¾-in hoseline from E31 and followed R1 members up to the 2nd floor and were staging on the stairs when the search crew from R1 decided to exit the 2nd floor.
While R1 members were searching the 2nd floor, it is believed that Victim #1 requested a fire fighter from the officer of L7. It is believed at this point that Victim #2 was paired with Victim #1 to perform a quick search of the deli for additional access points to the basement. Note: B56 recalls pairing them together to enter the deli. While inside the deli, Victim #1 updated B56 letting him know that he believed he found the basement stairs. Following their search, both victims exited the deli. Victim #2 returned to the FAST and Victim #1 did a face-to-face with B56. He adamantly advised B56 and B43 that he could hear people calling out and banging on pipes. Note: NIOSH investigators and fire department personnel believe that Victim #1 may actually have heard E22s crew operating within the 1st floor apartment. The 1st floor apartment and deli were divided by a wall of floor coolers at the rear of the store. Victim #1 then paired up with E23, who had just descended the 2nd floor stairwell, to advance a line into the deli to prepare for a rescue attempt. The E23 crew and Victim #1 advanced into the deli and began to spray water on the corner of Side 3 and Side 4 of the deli on what was believed to be the basement stairs that had burned out (see Diagram 7). Note: This was actually a hole where fire is believed to have vented from the basement, possibly part of the fire vented hole discovered by E22 while within the 1st floor apartment. Victim #1 advised B43 that they had water on the fire in the basement, and B43 and B56 acknowledged this transmission. Shortly after this transmission, Side 2 updated their progress and inability to access the basement. B56 conferred with B43 and they decided to remove all fire fighters from interior operations. It is believed that Victim #1 exited the deli, changed his air bottle, and met B56 at the command post in front of Side 1 by the deli door. Note: During NIOSH interviews, R1 members and a member from E22 recalled seeing Victim #1 at the air utility vehicle. It is believed that Victim #1 updated B56 of what they found and accomplished while in the deli. The fire department reports that Victim #1 may have stated the following, stairs on the side but the floors getting hot its burning good. Following this face-to-face, it is believed that R1 was tasked with verifying that no additional fire fighters remained inside the deli. Victim #1 re-entered the deli followed by two fire fighters from R1 to verify no fire fighters remained within the deli. The other two fire fighters did not enter the deli immediately with Victim #1. It is believed that there was a momentary delay as they waited for their TIC to power on. It is believed that Victim #1 followed E23s hoseline, still positioned within the deli, back to where they were flowing water into the basement. The fire fighter carrying the TIC also followed the line in, staying on the left side of the deli, but he could not see Victim #1; the other fire fighter entered the deli, turned to the right, and then traveled between two rows of shelving. Both of these fire fighters view of the rear of the store was obscured by thick, black smoke and deli displays. The fire fighter who remained on the line reported hearing a pop followed by displays falling toward him. Note: This is believed to be when the floor collapsed under Victim #1. He quickly followed the line out of the deli. The second fire fighter recalled hearing someone screaming for help from what he thought was the basement. He quickly notified B56 and exited the deli; both were met by Victim #2 and a member from L15 in the deli doorway. Both members from R1 were unaware of the floor collapse that had just occurred.
Activities of L7 (FAST) on Side 1
L7 arrived on scene directly after B43 requested an extra 2 and 1. They arrived with two fire fighters, a lieutenant, and Victim #2 who was a call-in for L7 that night. They were assigned as the FAST for the incident. Equipment for the FAST was removed from the apparatus and positioned at the corner of Side 1 and Side 4, out of the collapse zone. B56 was aware of their arrival and location on scene. The officer of L7 and Victim #2 walked counter-clockwise around the structure looking for access points and sizing up the structure. After walking around the structure, they returned to their staging point. The L7 officer then went and spoke to B56 for a moment. While walking back to the FAST staging point, the L7 officer was met by Victim #1 requesting one man to assist him. The L7 officer did not question Victim #1s urgency, so he provided him with Victim #2 to assist him. Although it has not been confirmed, it is believed at this time that Victim #1 and #2 went into the deli to perform a search. A fire fighter from the FAST recalled Victim #2 going into the structure with Victim #1. After Victim #1 and #2 exited the deli, B43 ordered the FAST to open up the deli store front. The FAST had to cut through metal bars and mesh, and the store front plate glass was actually protected from the inside with paneling, which caused difficulty in gaining access for ventilation (see Photo 10).

|
|
Photo 10. L7 officer and fire fighter from FAST working on store front just before Mayday. (Photo courtesy of off-duty fire fighter.) |
While attempting to ventilate the store front, raw video shows Victim #2 back with the FAST, operating a saw, and working next to the L7 officer on the deli store front, just to the right of the deli door. The raw video jumps forward and captures Victim #2 walking at the tailboard of E31 when the Mayday from Victim #1 was transmitted and then animatedly pointing at the structure as if he knew exactly from where the Mayday call was coming. Note: Fire department personnel believe that Victim #2s radio may have been off or on the wrong channel at this time. The video shows Victim #2 getting the attention of another FAST member standing next to the officer of L7 who is next to the deli door. The officer of L7 was operating a saw on the store front and does not initially acknowledge what is going on.
Victim #2 moves to the front of the deli entrance door and is seen rapidly attempting to get his facepiece on. A L15 member briefly enters into the deli but is then pushed out by two members from R1. Victim #2 hesitates entering the deli, leaves the viewing screen of the video, and then enters through the deli door with a tool in hand. Fire fighters on the fireground are heard yelling, Basement, basement! The L7 officer assembled his crew and was met on Side 1 by B43 who ordered the FAST to Side 2. The FAST is unaware that Victim #2 was not with them. A PASS alarm is heard as the FAST turned the corner to Side 2. The FAST followed lines to the second door on Side 2 and was advised that the basement stairs had flashed.
Rescue and Recovery Operations
In the video, many fire fighters are seen moving between Side 1 and Side 2 trying to ascertain information on the location of the Mayday. The fire department commented that freelancing erupted following the Mayday. B56 believed that the Mayday came from Side 2 since that was the only known access point; B56 was not aware of the floor collapse or who transmitted the Mayday. Members from R1and L14 re-entered the deli following the same line as before. R1 reported back to B56 that fire had broken through the 1st floor and then later stated that he heard a PASS device alarming in the deli. E21 had just arrived on scene when the Mayday calls from Victim #1 were transmitted. The E21 crew left the engine and responded to the command post for an assignment. B56 advised E21 to follow the 1¾-in hoseline stretched through the deli door. They followed the line staying close to Side 2. Smoke was thick and heavy.
About 35 ft inside the deli, the crew came across a section of the deli floor that had opened up into the basement. The basement was full of fire and the hoseline appeared to be within the hole. They immediately backed out and advised B56 of what they found. B56 had E28 flake out a 2½-in hoseline from E31 and take it in to the deli. E21 personnel backed up E28 as they took the 2½-in hoseline inside the deli. Fire was now rolling across the ceiling of the deli and then without warning, blew out the deli door. E28 and E21 crews quickly evacuated the deli taking the 2½-in hoseline with them. The 2½-in hoseline was then operated from the deli door threshold.
An emergency head count was conducted following the collapse and it was determined that Victim #1 from R1 was missing. It was not until a third head count was conducted that Victim #2 was confirmed missing. Victim #2s exact whereabouts within the structure were still unknown. Rescue/recovery efforts continued while crews attempted to breach the basement door on Side 2 and breach the Side 4 wall into the basement. A technical rescue crew was also dispatched to the scene to assist in breaching and shoring a wall on Side 4 (see Photo 11).

|
Photo 11. Photo shows Side 4 point of entry and shoring during rescue/recovery operations. |
Once Side 4 was shored, a crew was able to briefly access the basement from the hole on Side 4 but due to debris, instability, and several feet of water within the basement, the victims could not be accessed and brought out that way. Crews were also concentrating on performing a rescue from Side 1 through the deli entrance. Rescue/recovery operations took a significant amount of time due to the fire structure becoming fully involved with fire and unstable following the partial collapse of the deli floor. Once the basement fire broke through parts of the 1st floor, it quickly started to burn on the 2nd floor, causing a collapse of the 2nd floor in areas as well. The IC assessed the incident and risk involved and made a decision not to send additional fire fighters into the structure until the fire could be controlled and the structure was safe to enter. Hours after the initial collapse, the fire was contained and crews were able to construct a surface that fire fighters could use to place on the unstable deli floor. The victims were found side-by-side, 35 ft within the structure, 12 ft from the Side 2 wall, and 6 ft below the deli floor within the basement (see Diagrams 8 and 9). The victims were removed from the collapsed area within the deli. They were pronounced dead on scene. No civilians were discovered within the structure.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that may have led to the fatalities:
- Working above an uncontrolled, free-burning basement fire.
- Interior condition reports not communicated to command.
- Inadequate risk-versus-gain assessments.
- Crew integrity not maintained.
CAUSE OF DEATH
According to the county medical examiners office, the victims died from inhalation of products of combustion. The carboxyhemoglobin (COHb) levels were approximately 53% for Victim #1 and 51% for Victim #2.
RECOMMENDATIONS
Recommendation #1: Fire departments should ensure that all personnel are aware of the dangers of working above a fire, especially a basement fire, and develop, implement, and enforce a standard operating procedure (SOP) that addresses strategies and tactics for this type of fire.
Discussion: Basement fires can be taxing and test a fire fighters knowledge and skill on how to combat it safely and effectively. Fire burning underneath floors can significantly degrade the floor system with little indication to fire fighters working above.1 They need to be aware of rapid heat buildup, little or no ventilation, limited accessibility, and whether it is a storage place for unknown hazards (e.g., combustibles, hazardous materials, and flammable liquids). Also of concern for fire departments is how to determine how long a fire has gone undetected. Fire fighters should be aware of what is stored on the floor directly above a basement fire, what the finished floor is comprised of (e.g., terrazzo, plywood, tongue-and-groove, tile, etc.), and what the floor structural members are comprised of (e.g., engineered wood floor joists, concrete, or steel). Structural support members may be directly exposed to fire, causing them to weaken and increase the likelihood of an above-floor collapse. Interior crew(s) intending to operate on the floor above a basement fire should limit their operating time, especially if ventilation, suppression, and accessibility are not progressing. The floors structural members will continue to weaken as fire and heat intensify. Specifying an exact length of time for how long suppression crew(s) should operate above a basement fire is questionable, and the IC should make that determination by performing a hazard analysis/risk assessment. The fire department did not have an SOP specifically addressing strategies and tactics when combating basement fires. SOPs should be developed to address structural fire fighting operations specific to basement fires, because these types of fires present a complex set of circumstances and following established SOPs will minimize the risk of serious injury to fire fighters.
During this incident, fire fighters were unable to access the basement, unable to ventilate the basement fire, and unaware of the fire load found within the basement. Initially, the department did not cut a hole in the 1st floor apartment or deli and use their Bresnan distributor, in fear of injuring reported trapped civilians. Note: The Bresnan distributor is a type of cellar nozzle used to suppress fire through steam conversion. The use of a cellar nozzle, like a Bresnan distributor, during the initial stages of the basement fire may have assisted in containing the fire and/or allowing better operating conditions for fire fighters to access the basement.2 Attempts were made to flow water on the 1st floor where fire had vented through, but this effort was not successful. Fire fighters should also recognize that fire venting through a floor is a late indication of a weakened floor system.
Recommendation #2: Fire departments should ensure that the incident commander (IC) receives interior status reports and performs/continues evaluating risk-versus-gain.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial size-up of the incident. A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. The size-up should also include assessments of risk-versus-gain during incident operations, especially after primary searches have been conducted.2-7 The size-up should include an evaluation of factors such as the fire size and location, length of time the fire has been burning, conditions on arrival, occupancy, fuel load and presence of combustible or hazardous materials, exposures, time of day, and weather conditions. Information on the structure itself should include size, construction type, age, condition (e.g., evidence of deterioration, weathering), evidence of renovations, lightweight construction, loads on roof and walls (e.g., air conditioning units, ventilation ductwork, utility entrances), and available preplan information are all key information that can affect whether an offensive or defensive strategy is employed. The incident commander should be willing to change his strategy and plan based on continued size-ups and risk assessments until the fire is brought under control. Conducting accurate size-ups and receiving interior/exterior status updates is critical to the safety of fire fighters on the incident, rescue/recovery efforts, and overall control of the incident. The decision to commit interior firefighting personnel should be made on a case-by-case basis with proper risk-benefit decisions being made by the incident commander. The commitment of firefighters lives for saving property and an unknown or marginal risk of civilian life must be balanced appropriately. 8 The fireground is very dynamic, and conditions can either improve or deteriorate based on fire suppression activities, and available resources, and most importantly assessments/size-ups of the incident are necessary to detect a change on the fireground.
During this incident, the fire department was attempting to gain access to reported trapped civilian(s) in a basement. The command post was established at the front of the structure providing views of Side 1 and Side 2. The basement contained heavy smoke and fire and was inaccessible from exterior and interior access doors. The initial IC and the IC who assumed command performed initial size-ups and received radio updates on fire and smoke conditions from personnel working on the incident, but not all interior findings were reported. Crews working in the 1st floor apartment encountered fire venting through the floor on Side 4 as early as 9 minutes after the first apparatus arrived on scene. Ten minutes later, Victim #1 was flowing water on fire that had vented in the corner of Side 3 and Side 4 of the deli. This was the same general area where crews within the 1st floor were working. The only thing separating the apartment and deli was a wall of floor coolers. The basement fire burned uncontrolled for more than 30 minutes while fire fighters continued attempts to gain access to the basement. Incident updates on the radio included transmissions such as untenable and time to get out, prior to the 1st floor partial collapse. The IC also mistook water on the fire as fire fighters actually attacking the basement fire from Side 2. This provided the IC with a false sense of progress on combating the basement fire. Also, during this incident, the IC was at times monitoring multiple radio channels and some additional transmissions may not have been received. Radio transmissions are very important for the IC to hear, acknowledge, and prioritize so that the IC can maintain situational awareness, and accurately and effectively manage and direct fireground operations. A chiefs aid or incident command technician assigned to the IC may have assisted the IC in monitoring the fireground channels and distinguishing key radio traffic and updates. It is reasonable to believe that, as time progressed and basement fire conditions continued to be uncontrolled, that the chances of survival diminished for any potentially trapped civilians exposed to the heat or products of combustion found within the smoke. According to fire investigators with the fire department, only the bodies of Victim #1 and Victim #2 were found within the structure.
Recommendation #3: Fire departments should ensure that crew integrity is maintained at all times on the fireground.
Discussion: Fire fighters should always work and remain in teams whenever they are operating in a hazardous environment.2 Team integrity depends on team members knowing who is on their team and who is the team leader; staying within visual contact at all times (if visibility is low, teams must stay within touch or voice distance of each other); communicating needs and observations to the team leader; and rotating together for team rehab, team staging, and watching out for each other (e.g., practicing a strong buddy system). Following these basic rules helps prevent serious injury or even death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained. 3
During this incident, raw video captured the FAST working on Side 1 of the structure (same side that Victim #1 had entered) during Victim #1s Mayday. At the same time, Victim #2, assigned to the FAST, was seen pointing at Side 1, donning his SCBA, and entering the structure as other fire fighters were exiting from Side 1. The FAST was activated and ordered to Side 2 where it was believed the Mayday transmission came from. Victim #2 went missing following the Mayday and his whereabouts were unknown until the recovery of Victim #1. Also, Victim #1 entered the deli not realizing that two of his team members from R1 were not following behind. Not verifying your crew is with you and/or working alone increases the risk to individuals and possibly to others during search and rescue efforts. During interviews, the fire department commented on an increase in freelancing following the Mayday.
Recommendation #4: Fire departments should ensure that the incident commander (IC) receives accurate personnel accountability reports (PAR) so that he can account for all personnel operating at an incident.
Discussion: An important aspect of an accountability system is the personnel accountability report (PAR). A PAR is an organized on-scene roll call in which each supervisor reports the status of his crew when requested by the IC or emergency dispatcher.2 The use of an accountability system is recommended by NFPA 1500 Standard on Fire Department Occupational Safety and Health Program9 and NFPA 1561 Standard on Emergency Services Incident Management System.10 A functional personnel accountability system requires the following:
- development of a departmental SOP
- training all personnel
- strict enforcement during emergency incidents
As the incident escalates, additional staffing and resources may be needed, adding to the burden of tracking personnel. An incident command board should be established at this point with an assigned accountability officer or aide. As a fire escalates and additional fire companies respond, a chiefs aide or accountability officer assists the incident commander with accounting for all fire fighting companies at the fire, at the staging area, and at the rehabilitation area. With an accountability system in place, the incident commander may readily identify the location and time of all fire fighters on the fireground. A properly initiated and enforced accountability system that is consistently integrated into fireground command and control enhances fire fighter safety and survival by helping to ensure a more timely and successful identification and rescue of a disoriented or downed fire fighter. This department has developed and implemented SOPs governing accountability and even assigns an accountability officer to the IC to assist with radio transmissions and PARs.
An accountability officer was assigned to assist the IC during the incident. A PAR was immediately obtained following the rescue attempts for Victim #1. Victim #1 was identified as missing, but Victim #2 was incorrectly identified as accounted for. Victim #2 was incorrectly accounted for during a second separate PAR. Prior to a third PAR, 50 minutes following the floor collapse, Victim #2 could not be visibly accounted for on the fireground and his whereabouts were unknown. Officers need to visually account for their members prior to providing an all accounted for to the IC or accountability officer. Quickly being able to account for all personnel at an incident is paramount and can determine how an IC orders search and rescue efforts or other suppression activities.
Recommendation #5: Fire departments should ensure that a separate incident safety officer, independent from the incident commander, is appointed at each structure fire.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System, 11 The incident commander shall have overall authority for management of the incident and the incident commander shall ensure that adequate safety measures are in place. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the incident commander is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished. 10 According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program, 9 as incidents escalate in size and complexity, the incident commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) to assess the incident scene for hazards or potential hazards. These standards indicate that the incident commander is in overall command at the scene but acknowledge that oversight of all operations is difficult. On-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO. Additionally, the incident commander relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk versus gain and offensive-versus-defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and the incident commander. NFPA 1521 Standard for Fire Department Safety Officer defines the role of the ISO at an incident scene and identifies duties such as recon of the fireground and reporting pertinent information back to the incident commander; ensuring the departments accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.11 Larger fire departments may assign one or more full-time staff officers as safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the incident commander. The presence of a safety officer does not diminish the responsibility of individual fire fighters and fire officers for their own safety and the safety of others. The ISO adds a higher level of attention and expertise to help the fire fighters and fire officers. The ISO must have particular expertise in analyzing safety hazards and must know the particular uses and limitations of protective equipment. 4
During this incident, the designated department ISO was not dispatched until the incident was upgraded to a 2nd alarm because it occurred after the normal duty shift of the ISO. The ISO did not arrive until rescue/recovery operations had begun on breaching the Side 4 wall. The presence of an ISO throughout this incident would have allowed the IC to focus on supervising the incident while the ISO directed safety operations.
Recommendation #6: Fire departments should ensure that fire fighters use their self-contained breathing apparatus (SCBA) and are trained in SCBA emergency procedures.
Discussion: Fire fighters are tasked at times to operate within environments which pose inhalation hazards (e.g., toxic smoke and oxygen deficiency12), defined by OSHA as immediately dangerous to life and health (IDLH). Proper training along with an implemented and enforced policy or procedure will assist fire fighters with proper maintenance, use, and removal of a SCBA. OSHA 29 CFR 1910.134 (g)(4)(iii) states, all employees engaged in interior structural firefighting use SCBAs.13 During this incident, the medical examiner stated both victims died from inhalation of products of combustion. The medical examiner also indicated that the victims COHb levels (a measure of carbon monoxide in the bloodstream) were over 50%. Even if nothing but carbon dioxide, water vapor, and nitrogen were present in the fire products and these were to mix with the air being breathed by a fire fighter, then the oxygen percentage would be reduced below the normal 21%. At 15% oxygen, fire fighters can experience lethargy, poor coordination, and confused thinking. The two principal toxins in smoke—carbon monoxide and hydrogen cyanide—act to deprive the brain of oxygen, and their effects would be enhanced due to the lower levels of oxygen in the air.14 Both victims were discovered without their facepieces on.
Due to the smoke conditions, both victims would have had to have been on air when entering the structure. It has not been determined why both victims were found without their facepieces on, but NIOSH investigators have theorized the following possibilities:
- Victim #1 removed his facepiece to transmit his Mayday.
- Both victims facepieces were unintentionally knocked off when falling into the basement.
- The facepieces were removed because they ran out-of-air or other emergency situation.
Emergencies created by, or associated with, SCBAs can be overcome in several ways. Fire departments can develop and implement a comprehensive respiratory protection program15 that includes fire fighter fitness, training, competency, and skill in SCBA and emergency procedures. Firefighters should remember the first rule in any emergency situation, and that is not to panic. Panic causes increased breathing air consumption and inability to focus on emergency procedures. If fire fighters become lost, trapped, or disoriented they need to focus on managing remaining air in their SCBA cylinder until other fire fighters can make a rescue attempt. Removing ones facepiece in an IDLH atmosphere can immediately expose the respiratory system to a potentially fatal environment, thus incapacitating an individual. Choosing to leave ones SCBA facepiece on may be the best chance in providing additional time for a fire fighter to be rescued. Fire fighters should follow their departments SOPs regarding emergency SCBA procedures and emergency communications.
Recommendation #7: Manufacturers, equipment designers, and researchers should conduct research into refining existing and developing new technologies to track the movement of fire fighters inside structures.
Discussion: Fire fighter fatalities often are the result of fire fighters becoming lost or disoriented on the fireground. The use of systems for locating lost or disoriented fire fighters could be instrumental in reducing the number of fire fighter deaths on the fireground. The National Institute of Standards and Technology (NIST) has been evaluating the feasibility of real-time fire fighter tracking and locator systems for some time.16, 17 Another group researching advanced fire fighter locator and tracking systems is the Maryland Fire Rescue Institute, located at the University of Maryland College Park.18 Research into refining existing systems and developing new technologies for tracking the movement of fire fighters on the fireground should continue. While it is not clear that the use of this technology in this incident would have prevented the fatalities, such technology could potentially have reduced the search time by aiding rescue teams in pin-pointing the location of the missing fire fighters. This new technology must function properly in the severe fire conditions often encountered during rescue operations.
During the initial stages of the incident, it was not known who was transmitting the Mayday, where exactly they were in the basement, or how they got into the basement. Victim #2 went accounted for approximately 50 minutes before a determination was made that Victim #2 was also missing. It was not until rescue/recovery crews visually located the victims that they accounted for the location of Victim #2. This technology may have assisted the fire department during this incident in more quickly locating Victim #1 and Victim #2.
Of importance, Victim #1s PASS device was alarming during the Mayday and when he was discovered, but it was reported to NIOSH investigators that Victim #2s PASS device was never heard. Victim #2s PASS device was evaluated as part of NIOSHS NPPTL SCBA inspection. Victim #2s PASS device failed to function when tested, but after the batteries were replaced within the PASS device, it alarmed appropriately. It has not been determined if the battery life was exhausted prior to Victim #2 going into the structure. It is important to note that the 2007 revision to NFPA 1982 Standard on Personal Alert Safety Systems (PASS) includes new heat and flame resistance requirements resulting from documented reports where PASS devices were not heard during fatal fireground incidents. 19 Laboratory testing conducted by NIST determined that exposure to high temperature environments caused the loudness of the tested PASS alarm signal to be reduced. This reduction in loudness can cause the alarm signal to become indistinguishable from background noise at an emergency scene. Initial laboratory testing by NIST highlighted that this sound reduction may begin to occur at temperatures as low as 300°F. Thus the use of PASS devices meeting NFPA 1982, 2007 Edition requirements is highly recommended.
Recommendation #8: Manufacturers, equipment designers, and researchers should continue to develop and refine durable, easy-to-use radio systems to enhance verbal and radio communication in conjunction with properly worn self-contained breathing apparatus (SCBA).
Discussion: The use of Personal Protective Equipment (PPE) and an SCBA make it difficult to communicate, with or without a radio.20-22 Faced with the difficult task of communicating while wearing a SCBA, fire fighters sometimes momentarily remove their facepieces to transmit a message directly or over a portable radio. Considering the toxic and oxygen-deficient hazards posed by a fire and the resulting products of combustion, removing the SCBA facepiece, even briefly, is a dangerous practice that should be prohibited. Even small exposures to carbon monoxide and other toxic agents present during a fire can affect judgment and decision-making abilities. To facilitate communication, equipment manufacturers have designed facepiece-integrated microphones, intercom systems, throat mikes, and bone conduction mikes worn in the ear or on the forehead.20-22
During this incident, interviewed fire fighters complained of radio transmissions being unintelligible at times or not heard at all. Although NIOSH investigators are not certain why Victim #1 and Victim #2 were found without their facepieces on, one theory is that Victim #1 may have momentarily removed his facepiece to better transmit his Mayday. Fire fighters recall hearing his transmissions as they came across the radio and also emanating clearly from the structure.
Recent testing by the National Institute for Standards and Technology (NIST) of portable radios in simulated fire fighting environments has identified that radios are vulnerable to exposures to elevated temperatures. Some degradation of radio performance was measured at elevated temperatures ranging from 100°C to 260°C, with the radios returning to normal function after cooling down. Additional research is needed in this area.16, 20 Fire service radios also need to be waterproof as normal fireground conditions dictate that radios are frequently exposed to excessive amounts of water during routine use through exposure to hose streams, overspray, water dripping from overhead, etc.
REFERENCES
- NIOSH [2009]. NIOSH workplace solutions: preventing deaths and injuries of fire fighters working above fire-damaged floors. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 2009-114.
- IFSTA [2008]. Essentials of fire fighting. 5th ed. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and control of fires and emergencies. Saddle Brook, NJ: Fire Engineering Book and Videos.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Dunn V [1998]. Risk management and lightweight truss construction. New York: WNYF, Official training publication of the New York City Fire Department, 1st issue.
- NIOSH [1999]. NIOSH alert: request for assistance in preventing injuries and deaths of fire fighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 99-146.
- Jones J [2001]. No empty threat. Fire Chief Nov 1. [http://firechief.com/mag/firefighting_no_empty_threat]. Date accessed: February 2010. (Link Updated 1/28/2013)
- NFPA [2007]. NFPA 1500 standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1561 standard on emergency services incident management system. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521 standard for fire department safety officer. 2008 ed. Quincy, MA: National Fire Protection Association.
- Klinoff R [2003]. Introduction to fire protection. 2nd ed. Clifton Park, NY: Thomas Delmar Learning.
- Occupational Safety and Health Administration (OSHA). 29 CFR 1910. 134 Respiratory Protection [https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=12716]. Date accessed: November 2009.
- Friedman R [1998]. Principles of fire protection chemistry and physics. Quincy, MA: National Fire Protection Association.
- NFPA [2006]. NFPA 1404 standard for fire service respiratory protection training. 2006 ed. Quincy, MA: National Fire Protection Association.
- NIST [2007]. Advanced fire service technologies program. Unpublished paper presented at the 2007 NIST Annual Fire Conference. National Institute of Standards and Technology, Building and Fire Research Laboratory Gaithersburg, MD April 4-5.
- NIST [2008]. Wireless sensor research at NIST. Gaithersburg, MD: National Institute of Standards and Technology, Building and Fire Research Laboratory [http://www.bfrl.nist.gov/WirelessSensor/]. Date accessed: November 2009. (Link no longer available 12/6/2012)
- Editorial Staff [2007]. Tracking system is the future of firefighting. Firehouse.Com News. [http://www.firehouse.com/news/10505378/tracking-system-is-the-future-of-firefighting]. Date accessed: February 2010. (Link Updated 1/28/2013)
- NFPA [2007]. NFPA 1982 standard on personal alert safety systems (PASS). 2007 ed. Quincy, MA: National Fire Protection Association.
- Davis WD, Donnelly MK, and Selepak MJ [2006]. Testing of portable radios in a fire fighting environment. Gaithersburg, MD: National Institute of Standards and Technology Building and Fire Research Laboratory, NIST Technical Note 1477.
- USFA/FEMA [1999]. Improving firefighter communications. USFA-TR-099. Emmitsburg, MD: United States Fire Administration.
- TriData Corporation [2003]. Current status, knowledge gaps, and research needs pertaining to fire fighter radio communication systems. Report prepared for NIOSH. Arlington, VA: TriData Corporation.
INVESTIGATOR INFORMATION
This investigation was conducted by Stacy C. Wertman, Safety and Occupational Health Specialist, and Matt Bowyer, General Engineer with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. This report was authored by Stacy C. Wertman. An expert technical review was provided by John J. Salka, Jr., Battalion Chief, Fire Department of New York.
Vance Kochenderfer, NIOSH Quality Assurance Specialist, National Personal Protective Technology Laboratory, conducted an evaluation of the victims SCBA. Angie Sheppard, NIOSH Quality Assurance Specialist, National Personal Protective Technology Laboratory, conducted an evaluation of the victims PPE.
DISCLAIMER
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
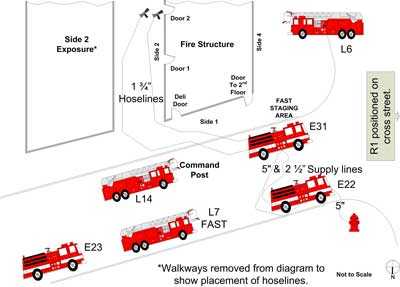
|
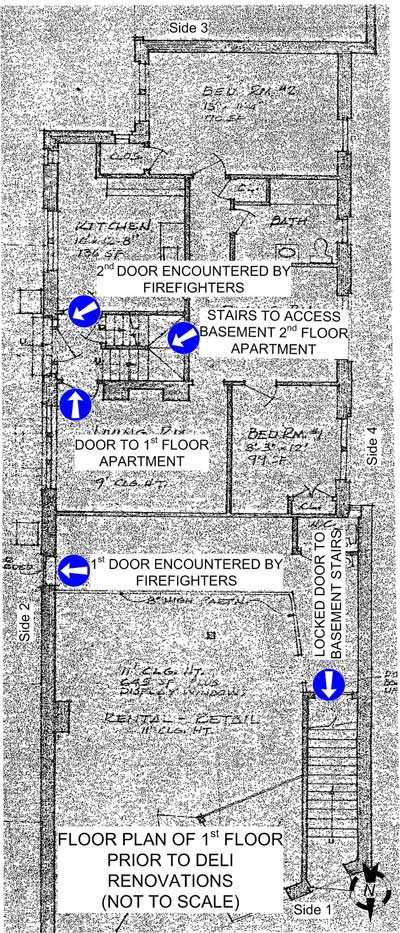
|
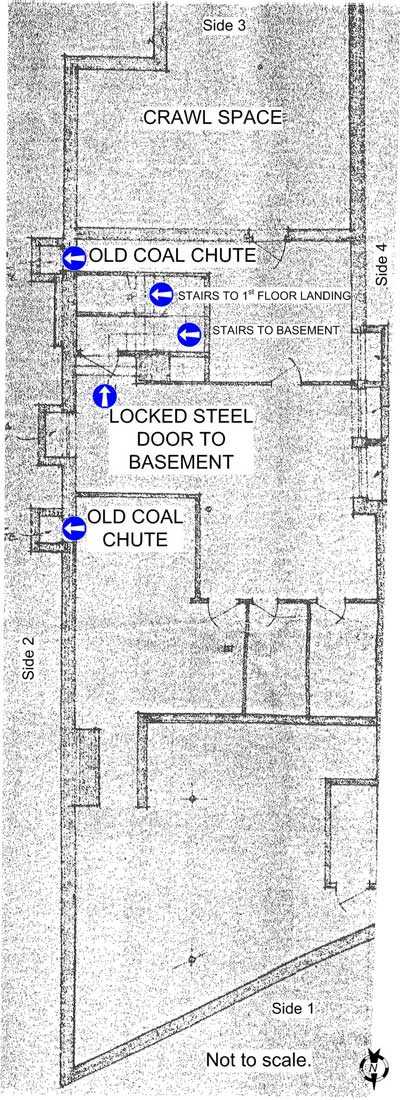
|
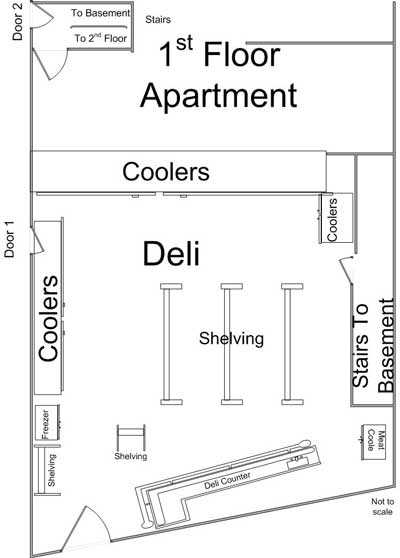
|
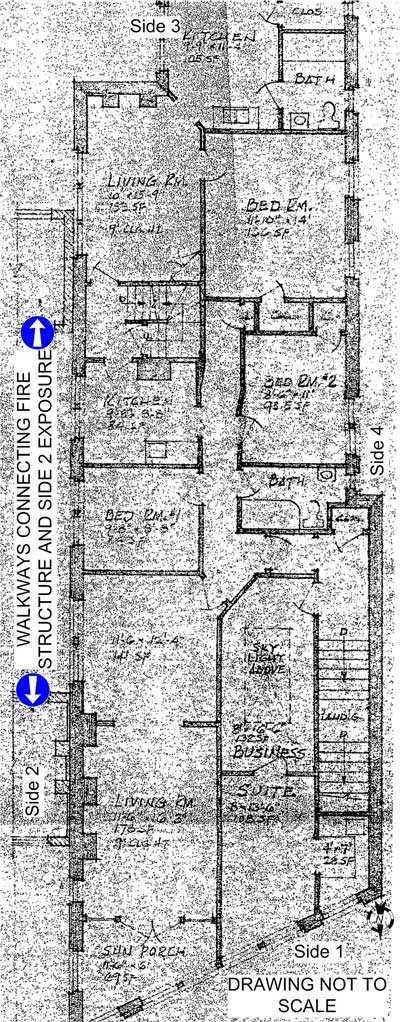
|
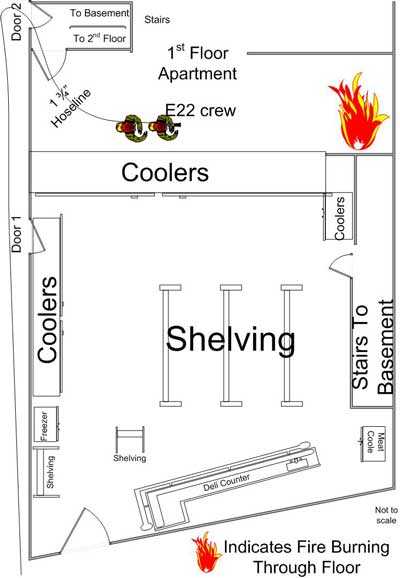
|
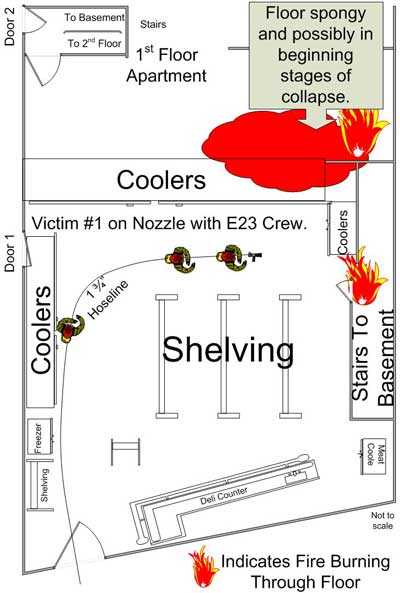
|
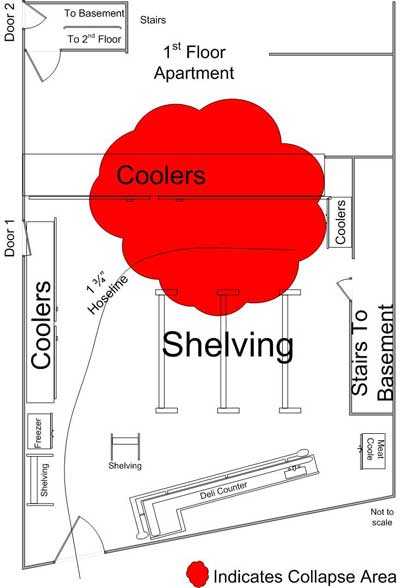
|
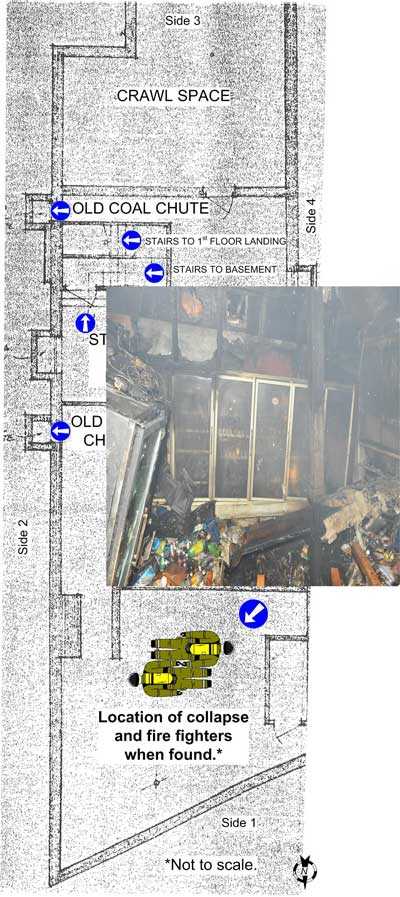
|
|
Diagram 9. Basement layout. |
APPENDIX
Status Investigation Report of Two
Self-Contained Breathing Apparatus
NIOSH Task Number 16575
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter
Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate two SCBA identified as Scott Air-Pak Fifty 4.5, 4500 psi, 30-minute, self-contained breathing apparatus (SCBA).
This SCBA status investigation was assigned NIOSH Task Number 16575. The fire department was advised that NIOSH would provide a written report of the inspections and any applicable test results.
The SCBAs, contained within two corrugated cardboard boxes, were delivered to the NIOSH facility in Bruceton, Pennsylvania on September 4, 2009. After its arrival, the packages were taken to building 108 and stored under lock until the time of the evaluation.
SCBA Inspection
The packages were opened in the Firefighter SCBA Evaluation Lab (building 02) and a complete visual inspection was conducted by Eric Welsh, Engineering Technician, NPPTL. The first SCBA was inspected on October 27, 2009 and was designated as Unit #1. The second SCBA, designated
Unit #2 was opened and inspected on October 29, 2009. The SCBAs were examined, component by component, in the condition as received to determine their conformance to the NIOSH approved configuration. The visual inspection process was videotaped. The SCBAs were identified as the Scott Air-Pak Fifty 4.5 model, 30 minute, 4500 psi units, NIOSH approval no.TC-13F-0076.
The condition of each major component was also photographed with a digital camera. It was judged that these units could be safely pressurized and tested using a substitute cylinder. A substitute facepiece was also used for the NIOSH tests that were performed.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA’s conformance to the National Fire Protection
Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-
Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
- Positive Pressure Test [§ 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [§ 84.95]
- Static Pressure Test [§ 84.91(d)]
- Gas Flow Test [§ 84.93]
- Exhalation Resistance Test [§ 84.91(c)]
- Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
- 7. Air Flow Performance Test [Chapter 5, 5-1.1]
Units #1 and #2 were tested on November 2, 3, and 24, 2009 using a substitute cylinder. All testing was video-recorded with the exception of the Exhalation Resistance Test and Static
Pressure Test.
Summary and Conclusions
Two SCBA were submitted to NIOSH by the fire department for evaluation. The SCBA were delivered to NIOSH on September 4, 2009 and inspected on October 27 & 29, 2009. The units were identified as Scott Air-Pak Fifty 4.5, 4500 psi, 30-minute, SCBA (NIOSH approval number TC-13F-0076). Both units have suffered some heat damage, exhibit other signs of heavy wear and tear, and were covered with dirt, grime, foreign particulate material and soot. The cylinder valves as received are in the open position on both units, and the gauges read zero. The regulator and facepiece mating and sealing areas on both units are very dirty and there is debris inside the facepieces and regulators. Unit #2 regulator gasket in the facepiece port was damaged and out of position. The harness webbing on Unit #1 is in poor condition with fraying and tears. The PASS device in Unit #1 did not function and the PASS device in Unit #2 worked only after the batteries, which were rust-covered on the cathode sides, were removed and re-inserted. On March 9, 2010, a new battery was placed in the Unit #1 PASS device and attempted to activate it. The device appeared to function normally, both when the manual alarm button was pressed and also in the automatic sensing mode. A voltage check of the batteries received with the PASS device revealed them to be nearly completely drained. Unit #2 exhibited some corrosion and rust on the high pressure line to the cylinder connection nut. The NFPA approval label on Unit #1 was mostly abraded away. Visibility through the lens of Unit #1 was poor and visibility through the lens of Unit #2 was fair to poor. The air cylinder on Unit #1 has a re-test date label indicating a re-test date of 9(?)/04 (month was partially obliterated, most likely is 9). The air cylinder on Unit #2 has a re-test date label of 8/04. Under the applicable DOT-E-10945 exemption, these air cylinders are required to be re-tested every 5 years after July 1, 2001. Both cylinders were therefore near their due date for re-test at the time of last use. Unit #1 cylinder also has some heavy gouges exposing the composite material. As both cylinders were past their re-test date at the time of testing, a replacement air cylinder with a current hydrostatic re-test qualification was obtained from the fire department and was substituted for all tests on both units. No other maintenance or repair work was performed on the units at any time.
Unit #1 failed to meet the requirements of the NIOSH Positive Pressure Test, with a minimum pressure of -0.05 inches of water. Units #1 and #2 met the requirements of all of the other tests.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part at this time. Following inspection and testing, the SCBA were returned to storage pending return to the fire department.
If the units are to be placed back in service, they must be repaired, tested, and inspected by a qualified service technician, including such testing and other maintenance activities as prescribed by the schedule from the SCBA manufacturer. Typically a flow test is required on at least an annual basis.
Protective Clothing Ensemble Inspection and Findings
As a component of the NIOSH Fire Fighter Fatality Investigation and Prevention Program (FFFIPP) investigation F2009-23 NY, an inspection was conducted on elements of the fire fighter protective ensembles worn by the victims. The Morgantown Testing Team, part of the Evaluation and Testing Branch (ETB) of National Personal Protective Technology Laboratory (NPPTL), conducted this evaluation on October 27, 2009 in Morgantown, WV.
The protective ensemble elements inspected included two protective coats, two protective pants, and one protective hood. No additional elements or station work uniforms were provided for evaluation.
The inspection consisted of examining the ensemble elements to determine if there was any damage, defects or conditions of the protective ensemble elements that may have contributed to the fatality.
This process was conducted in a manner consistent with Procedure No. SOP-NPPTL-TRB-PCE-0001 - “National Institute for Occupational Safety and Health (NIOSH) Procedure for Conducting Protective Clothing Evaluations for the Fire Fighter Fatality Investigation and Prevention Program (FFFIPP)”.
Based on the inspection, the protective clothing ensembles performed as intended for a single catastrophic event and the ensemble elements are not believed to have contributed to the fatalities of this incident.
A copy of the complete evaluation, NPPTL-PCER-01, will be provided upon written request.
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agencys recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit
the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 03/08/2010.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research