


Career Fire Fighter/Paramedic Dies 2 Days After Being Ejected During an Ambulance Rollover Incident Georgia
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2009-30 Date Released: July 2, 2010
Executive Summary
On December 26, 2009, a 37-year-old male career fire fighter/paramedic (the victim) was ejected from the front passenger seat of a fire department ambulance during a rollover incident. The ambulance was responding with lights and siren to a car fire with injuries. A motorist in a privately owned vehicle (POV) turned into the path of the ambulance as it was passing the POV. The ambulance struck the POV, lost control, and left the right side of the roadway. The ambulance overturned three times, and the victim was ejected. The driver sustained minor injuries. The victims use of a seat belt could not be determined with certainty. The victim was airlifted by helicopter to a local trauma center where blunt force chest injuries, and underlying medical conditions, contributed to his death on December 28, 2009.

|
Front view of ambulance after the incident. |
Contributing Factors
- Failure of the motorist to yield the right-of-way to an approaching emergency vehicle with audible and visual signals in use
- Ejection of the victim
- Blunt chest trauma resulting in multiple rib fractures
- The victim’s underlying medical conditions.
Key Recommendations
- States and authorities having jurisdiction should take steps to ensure that motorists are aware of, understand, and follow state traffic codes/laws pertaining to yielding the right-of-way to approaching, authorized emergency vehicles using audible and visual signals
- Fire departments should take steps to ensure that seat belts are properly worn at all times
Additionally, governing municipalities (federal, state, regional, and local) should:
- Consider enacting legislation to include drivers and occupants of fire department vehicles in existing seat belt legislation and/or repeal existing laws that exempt drivers and occupants of fire service vehicles from mandatory seat belt use.

|
|
Rear view of ambulance after the incident. |
Introduction
On December 26, 2009, a 37-year-old male career fire fighter/paramedic (the victim) was ejected from the front passenger seat of a fire department ambulance during a rollover incident. The victim was airlifted by helicopter to a local trauma center where blunt force chest injuries, and underlying medical conditions, contributed to his death on December 28, 2009. On December 28, 2009, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. The ambulance was transported to fire department headquarters following the incident where it remained until the NIOSH investigation. On February 1-4, 2010, a safety and occupational health specialist from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to Georgia to investigate this incident. The NIOSH investigator met with the fire chief, officers, fire department training and administrative staff, the county fire marshal, fire fighters who had responded, and, a member of the Georgia Local Assistance State Team from the National Fallen Fire Fighters Foundation. Interviews were conducted with the ambulance driver, training division lieutenant, other ambulance drivers, a representative of the Georgia State Patrol, and fire and emergency medical service (EMS) personnel who responded to the incident. The NIOSH investigator inspected and documented the condition of the ambulance involved in the incident, photographed an identical undamaged ambulance, and reviewed incident scene photographs taken by the fire department. The NIOSH investigator reviewed the fire departments standard operating procedures (SOPs), driver training program, fire training curriculum, the victims and ambulance drivers training records, radio transcripts from the incident, ambulance specification and build sheet, Georgia State Patrol traffic crash report, death certificate, autopsy report, and ambulance maintenance records. The NIOSH investigator also visited and photographed the incident site.
Fire Department
This career fire department has 10 stations with 162 uniformed members which serve a population of approximately 126,000 within an area of about 202 square miles. All department members work a 24 hour duty shift with 48 hours off, and department members may be assigned to a fire apparatus or an ambulance for the entire 24-hour shift. The fire department currently has 10 engines, 3 aerial ladders, 6 advanced life support ambulances, and 1 heavy rescue truck. All fire department apparatus are maintained by the countys fleet maintenance division with annual testing of fire apparatus and ambulances conducted by qualified vendors.
The fire department has written policies and procedures, which are available to all department members within their stations. These policies and procedures have been implemented and are enforced and include driver safety training, out-of-service criteria for apparatus, safe placement of apparatus, and vehicle maintenance and repair reporting.
Training and Experience
Prior to 2009, the fire department did not have a driver training program that met the requirements of NFPA 1451 Standard for a Fire Service Vehicle Operations Training Program1 or minimum skills and knowledge requirements to demonstrate proficiency to be qualified to NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications.2 No funding was available to implement this type of program and no facility was available to deliver a driving obstacle course. The training division would evaluate a new hires ability to operate an ambulance and could potentially release the driver that same day to operate the ambulance if the training division staff felt comfortable with the driver. Note: Prior to 2009, most new hires had prior experience operating emergency vehicles. There were not a minimum number of driver training hours required for releasement and no records related to driver training were kept on individual fire fighters. The county did, however, require fire department members to complete the National Safety Councils Defensive Driving Course,3 which was a 6-8 hour classroom course with a final written test. Note: This defensive driving course did not provide hands-on inspection or operation of emergency vehicles and focused on passenger vehicles only.
In 2009, this department opened a new training complex, which allowed them to implement a driving obstacle course as outlined by NFPA 1002.2 The department now operates their own fire academy, which includes the countys required defensive driving course and driver obstacle course. The training division is currently recording and maintaining all driver training records for new hires and current fire fighters. However, the department has yet to implement a driver training program that includes policies and procedures on when a driver should be released to operate an emergency vehicle, or how often and what type of driver training should be provided. Note: NFPA 14511 states that fire departments should establish and maintain a driver training program and each driver/operator should be provided driver training not less than twice a year. Under the current program, new hires can still be released to operate an ambulance without any prior experience, logged miles or hours, or mentorship. Drivers can, however, lose their privilege to operate an ambulance if they are observed driving in an unsafe manner by department members, training staff, or department officers. Remedial training would then be provided to that individual.
The ambulance driver was hired with this department in August 2008 after being employed with a neighboring fire department from 2004-2008. He was not required to participate in the departments fire academy or complete the driver obstacle course. He did, however, complete the countys required defensive driving course in 2009, and he operated an ambulance under training staff supervision for about an hour before being released to operate department ambulances. While at his previous employer, the driver completed the National Safety Councils courses, Coaching the Emergency Vehicle Operator II: Fire and Ambulance.4, 5 He also completed that departments driver training program, which required him, under supervised guidance, to log driving miles, and operate the emergency vehicle under normal and emergent operations, in different types of weather and lighting. The driver of the ambulance stated to the NIOSH investigator that he had more than 5 years experience operating emergency vehicles, including ambulances, during normal and emergency conditions, and that he had not previously been involved in a vehicle incident.
Equipment and Personnel
The incident involved an ambulance with a fire fighter/emergency medical technician (EMT) driver and a fire fighter/paramedic attendant (the victim). The ambulance involved in this incident was a 2006 Type IIIa Class 1 (4x2) with a diesel engine, automatic transmission, and anti-lock brakes. The vehicle was also equipped with three-point lap and shoulder belts in the front compartment. The patient compartment of the ambulance was configured with five seating positions, each equipped with a two-point lap belt. These riding positions included a bench seat accommodating three individuals; a rear-facing, high-backed attendants seat; and a cardiopulmonary resuscitation chair. The cot provided patient restraint belts for the shoulders, pelvis, and lower legs. The incident ambulance was one of three identical ambulances purchased in 2006 by the fire department (see Photo 1).

|
Photo 1. An identical ambulance purchased by the fire department. |
The ambulances front gross axle weight rating (GAWR) was 4,600 pounds and the rear GAWR was 9,450 pounds, with a total gross vehicle weight rating of 14,050 pounds. The ambulance involved in the incident was not weighed following the vehicle incident, but an identical ambulance weighed approximately 12,000 pounds with equipment but without personnel. It is not believed that the ambulance involved in the incident was overweight. The ambulance was mounted on a 159-inch wheel base and had two axles with six wheels (two in the front and four in the rear). The state of Georgia does not require emergency vehicles to have a yearly state vehicle inspection. Also, the state of Georgia does not require any special drivers license endorsement or commercial drivers license to operate emergency vehicles. The state of Georgia exempts passenger vehicles performing an emergency service from seat belt laws. The Federal Motor Carrier Safety Administration (FMCSA) [49 CFR 390.3(f)(5)] also exempts the occupants of fire trucks and rescue vehicles from wearing seat belts while involved in emergency and related operations. However, the county and fire department involved in this incident do require all persons riding in an emergency vehicle to be properly restrained.
a A Type III ambulance is a cutaway van chassis with integrated modular patient compartment.
Timeline
The timeline for this incident is limited to the initial response of units to a vehicle fire on December 26, 2009, which included the ambulance involved in the rollover incident. The driver of the ambulance was working his normally scheduled 24-hour shift and had responded to seven previous calls since his shift began at 0800 hours on December 26, 2009. The victim was working an overtime 24-hour shift and had responded to 11 previous calls since his previous shift began at 0800 hours on December 25, 2009.
- 2308 Hours
Engine 6 (E6) was dispatched and en route to a vehicle fire. Prior to their arrival on the scene of the vehicle fire, they came upon the injured driver, who was walking along the roadway, and requested rescue to respond. - 2309 Hours
Rescue 5 (R5) was en route (driver and victim) to meet E6. - 2312 Hours
R5 was involved in a rollover incident.
Personal Protective Equipment
At the time of the incident, the victim was wearing his station uniform, work boots, and high-visibility reflective jacket. The driver of the ambulance was wearing the same attire.
Weather and Road Conditions
The weather was clear with an approximate temperature of 35°F. The incident occurred on a two-lane road traveling east and west. The eastbound and westbound lanes were divided by a double yellow line. The roadway surface was asphalt and reported to NIOSH investigators to be dry when the incident occurred. The shoulder on the eastbound lane was made of earthen materials. The westbound lane had no apparent shoulder and had a drop off in areas that exceeded 4 inches. The incident occurred just before a T-intersection where the roadway was unlit and had a posted speed limit of 45 miles per hour (mph) (see Diagram). When interviewed by the NIOSH investigator, the driver of the ambulance believed he was traveling between 50-55 mph at the time of the incident.
Investigation
On December 26, 2009, a 37-year-old male career fire fighter/paramedic (the victim) was ejected from the front passenger seat of R5 (ambulance) during a rollover incident. The R5 crew had just returned to their station from a previous medical call and decided to respond in a nonemergency mode to a vehicle fire in case there were any injuries. While en route, R5 was requested by E6 to respond to E6s location for an individual who E6 had come upon while en route to the vehicle fire. The individual, who was injured, was the driver of the vehicle that was on fire. R5 upgraded their response to code 2 (lights and siren) in response to E6s request and headed eastbound. After initiating his code 2 response, the driver of R5 noticed a POV ahead of him, traveling in the eastbound lane. The driver of R5 increased his speed to what he believed was 50-55 mph when approaching the POV in anticipation of passing the POV on the left. The driver of R5 stated that the POV appeared to slow down and pull off onto the right shoulder of the roadway to allow the ambulance to pass. The driver of R5 observed no traffic in the oncoming westbound lane so he decided to cross the double yellow line and pass the POV. While doing so, the POV driver turned into the left lane and R5 and the POV collided (see Diagram). Note: The POV driver may have been making a left-hand turn onto a side street to get out of the way of the ambulance. The POV went off the left shoulder but did not overturn. The ambulance driver lost control of the ambulance and left the right side of the roadway. R5 overturned three times, and the victim was ejected. R5 came to rest on its wheels approximately 60 ft from the roadway. The driver of R5 immediately noticed that the victim was no longer in the ambulance. He radioed dispatch and advised them of what had happened. The driver exited R5 and found the victim face down along a fence line approximately 10 ft behind R5. The victim was conscious when the driver found him. The victim was airlifted by helicopter to a local trauma center where blunt force chest injuries, and underlying medical conditions, contributed to his death two days later. The driver of the POV had to be extricated from the vehicle and was transported to a local hospital with non-life-threatening injuries.
The state of Georgia traffic crash report stated that the front passenger side of R5 struck the POV on the driver side door (see Photo 2). The airbags did not deploy, and it was undetermined whether the victim was wearing his seat belt.
The crash investigation was turned over to the Georgia State Patrol Specialized Collision Reconstruction Team (SCRT) for further investigation. Information from the ambulances event data recorder was irretrievable.

|
|
Photo 2. Vehicle damage to ambulance after impact with POV. (Photo courtesy of fire department.) |
Seat Belt Use
It has not been determined whether the victim was ejected out the passenger side window or passenger door when it became ajar, but the passenger side window was broken during the rollover. Family and coworkers interviewed by the NIOSH investigator stated that the victim was adamant about wearing his seat belt. The driver of the ambulance stated the victim always wore his seat belt when they worked together, and he believed that the victim was wearing his seat belt the night of the incident. He also advised the NIOSH investigator that the victim routinely rode with his left hand holding the seat belt connection and left arm tucked into the seat because there was no arm rest. The state of Georgia traffic crash report listed the victims use of a seat belt as undetermined. The ambulance driver advised the NIOSH investigator that he was wearing his seatbelt at the time of the incident.
Ambulance Inspection
Within the front compartment, the master console broke away from the floor and dash mounts and other dashboard covers came off (see Photo 3 and Photo 4). The front compartment space remained intact and did not show damage past the A-pillar, and the patient compartment remained intact during the rollover incident (see Photo 5). Fire department officials stated that the ground was soft and wet from several days of rain, which may have cushioned the ambulance as it rolled.
 |
 |
Photos 3 and 4. Driver compartment of an identical ambulance (left photo) and driver compartment of the involved ambulance |
|

|
Photo 5. Exterior of the involved ambulance showing no obvious intrusion into the front and patient compartments. |
Fire department photos reviewed by the NIOSH investigator showed the potential for injuries if there had been a patient or attendant in the back of the ambulance. When the ambulance rolled, the cabinets opened up spilling their contents into the patient compartment, the bench seat and support rail came apart, the cot came undone from the floor locking mechanism, and EMS equipment (e.g., oxygen cylinders, medical bags, automated external defibrillator) were thrown throughout the compartment (see Photos 6-9). All these objects became projectiles, which had the potential to injure anyone riding in the patient or driver compartments.
 |
 |
Photos 6 and 7. Typical fire department patient compartment (left photo) and patient compartment of the involved ambulance after the rollover incident (right photo). |
|
 |
 |
Photos 8 and 9. Typical fire department bench seat support rail (left photo) and bench seat support rail of the involved ambulance after the rollover incident (right photo). |
|
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:- Failure of the motorist to yield the right-of-way to an approaching emergency vehicle with audible and visual signals in use.
- Ejection of the victim
- Blunt force trauma resulting in multiple rib fractures
- The victims underlying medical conditions.
Cause of Death
According to the death certificate, the medical examiner listed the victims cause of death due to blunt force traumatic injuries to the head.
Autopsy Findings and Cause of Death
An autopsy was performed by the Countys Associate Medical Examiner. Significant findings included:
- Blunt force injury of the head and torso
- Multiple bilateral posterior rib fractures - Blunt force injuries of the extremities
- History of obstructive sleep apnea requiring continuous positive airway pressure (CPAP)
- Hypertension
- Cardiomegaly with concentric left ventricular hypertrophy (540 grams) - Obesity (Body Mass Index = 41.5)
- Blood toxicology testing results:
- Morphine level: 0.16 ug/l (therapeutic level consistent with the administration of pain relief medication)
- Negative for ethanol and other common drugs of abuse
The Associate Medical Examiner concluded that the victim died from complications from obstructive sleep apnea due to blunt force chest injuries.
Recommendations/Discussions
Recommendation #1: States and authorities having jurisdiction should take steps to ensure that motorists are aware of, understand, and follow state traffic codes/laws pertaining to yielding the right-of-way to approaching, authorized emergency vehicles using audible and visual signals.
Motorists and emergency vehicle driver/operators should know the rules and regulations that govern the operation of the vehicle(s) they drive. Emergency vehicle driver/operators should be aware of the regulations describing how vehicles should be operated when audible and visual warning devices are in use. Motorists should be aware that most laws or ordinances provide that nonemergency vehicles must pull toward the right and remain at a standstill until the emergency vehicle has passed. This does not guarantee that people will follow this procedure. Some drivers may panic at the sound of an approaching siren; others may be unable to hear the siren due to radios, closed windows, talking on a cell phone, or loss of hearing; while others may simply ignore warning signals. Emergency vehicle driver/operators should pay close attention to motorists and anticipate other drivers actions. The state of Georgia Motor Vehicles and Traffic Code allows the driver of an emergency vehicle to exceed the maximum speed limits so long as he or she does not endanger life or property, and disregard regulations governing direction of movement or turning in specified directions. These provisions, however, shall not relieve the driver of an authorized emergency vehicle from the duty to drive with due regard for the safety of all persons.6 The state of Georgia Motor Vehicles and Traffic Code goes on further to state, Upon the immediate approach of an authorized emergency vehicle making use of an audible signal and visual signals, the driver of every other vehicle shall yield the right-of-way and shall immediately drive to a position parallel to, and as close as possible to, the right-hand edge or curb of the roadway clear of any intersection and shall stop and remain in such position until the authorized emergency vehicle…has passed, except when otherwise directed by a police officer.”7
During this incident, the ambulance was overtaking the POV in the left lane after the driver of the ambulance believed that the motorist was pulling to the right side of the road after slowing down. The ambulance driver had only seconds to react when the motorist turned the POV into the left lane. Although not believed to be a contributing factor, motorists should consider that motor vehicle codes vary from state to state on areas such as how a motorist should behave when a responding emergency vehicle is approaching them.
Motorists can be reminded of specific traffic codes/laws through public service announcements, electronic message boards, or posted roadway signs. State and Federal rule making entities should consider development and promulgation of a standard set of traffic code/laws to offset any potential confusion motorists may encounter when traveling in different states.
Recommendation #2: Fire departments should take steps to ensure that seat belts are properly worn at all times.
Discussion: Vehicle crashes are the second leading cause of fire fighter line-of-duty deaths.8 NFPA 1500 Standard on Fire Department Occupational Safety and Health Program states that all persons riding in fire apparatus should be seated and belted securely by seat belts in approved riding positions at any time the vehicle is in motion, and the seat belts should not be released or loosened for any purpose while the vehicle is in motion.9 Fire departments should develop, implement and enforce SOPs on the proper use of seatbelts in accordance with NFPA standards. Numerous nationally recognized fire service entities have guidance available on implementing a seat belt policy. The International Association of Fire Fighters (IAFF) provides guidance in their document Standard Operating Procedures, Fire Department Vehicle Safety, Emergency and Non-Emergency Response, and Safe Emergency Operations on Roadways,10 and recommends that all employees use seat belts at all times: All personnel shall ride only in regular seats provided with seat belts. The company officer and driver of the vehicle shall confirm that all personnel and riders are on-board, properly attired, with seat belts on, before the vehicle is permitted to move. This confirmation shall require a positive response from each rider. The International Association of Fire Chiefs (IAFC), Guide to IAFC Model Policies and Procedures for Emergency Vehicle Safety, states that The driver shall not begin to move the vehicle until all passengers are seated and properly secured. All passengers shall remain seated and secured as long as the vehicle is in motion. Seat belts shall not be loosened or released while en route to dress or don equipment.11 NFPA 1901 Standard for Automotive Fire Apparatus,12 recommends that a seat belt warning device be installed to indicate when seat belts are not being properly used.12 The state of Georgia exempts driver/operators and passengers of fire vehicles from having to wear a seat belt. The fire department involved in this incident did have policies and a procedure requiring the use of seat belts, and a mandatory use of seat belts was also in effect for all county government employees.
During this incident, the victim was ejected from the ambulance as it rolled over. It has not been determined whether he was ejected out the passenger side window or passenger door when it became ajar. Family and co-workers interviewed by the NIOSH investigator stated that the victim was adamant about wearing his seat belt. The driver of the ambulance stated the victim always wore his seat belt when they worked together, and he believed that the victim was wearing his seat belt the night of the incident. He also advised the NIOSH investigator that the victim routinely rode with his left hand holding the seat belt connection and left arm tucked into the seat because there was no arm rest.
Recommendation #3: Governing municipalities (federal, state, regional, and local) should consider enacting legislation to include drivers and occupants of fire department vehicles in existing seat belt legislation and/or repeal existing laws that exempt drivers and occupants of fire service vehicles from mandatory seat belt use.
Discussion: Vehicle crashes are consistently the second leading cause of fire fighter line-of-duty deaths.8 The state of Georgia does not require seat belt use by driver/operators and occupants of fire department vehicles and apparatus. The FMCSA also exempts the occupants of fire trucks and rescue vehicles while involved in emergency and related operations from wearing seat belts. These laws are not consistent with NFPA standards, and IAFC and IAFF recommendations as mentioned previously.9-12 Governing entities should consider enacting legislation that requires seat belt use by drivers and occupants of fire department vehicles and apparatus.
Recommendation #4: Fire departments should ensure that current driver training programs provide ample classroom instruction, behind-the-wheel driving, procedures for driver clearance, and annual refresher training.
Discussion: Although there is no evidence that the following recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. NFPA 1451 Standard for a Fire Service Vehicle Operations Training Program1 states that fire department personnel must be trained in and exercise applicable principles of defensive driving techniques under both emergency and nonemergency conditions. NFPA 1500 Standard on Fire Department Occupational Safety and Health Program9 and NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications2 describes the necessary knowledge and skills individuals need to possess in order to be a driver/operator, including such things as preventive maintenance inspections and demonstration of the proper operation of an apparatus under a variety of conditions.
NFPA 14511 and NFPA 10022 both state that fire departments should establish and maintain a driver training program and NFPA 1451 recommends that each driver/operator should be provided driver training not less than twice a year. Fire departments should be able to provide additional training specific to apparatus that the driver/operator would be assigned to drive. This should include training on how to handle the apparatus under difficult road conditions (e.g., steep grades, grade changes, and narrow roads) and when something unexpected occurs with the apparatus (e.g., unexpected brake failure, tire blowouts, or regaining control). During fire department training, instructors should verify that the driver/operator can safely operate the apparatus in accordance with local and state laws, perform a pre-trip inspection, identify gauges and controls within the cab of the apparatus (e.g., what gauge readings should be, what readings mean, and how and when to operate controls), and demonstrate knowledge and skills necessary to operate vehicles equipped with air brakes. Records should be maintained on each driver/operator of behind-the-wheel miles or hours and training.
A fire departments driver training program will assist the department in making a determination on whether a new driver or current driver is qualified and possesses enough experience to safely operate an apparatus. Fire departments should understand that documented training hours alone do not prove that the training was effective. However, the program may help in areas such as speeding, inexperience with apparatus, identification of hazardous situations or actions, overconfidence, urgency, and poor driving habits.
The ambulance driver involved in this incident was previously cleared to drive under another fire departments driver training program, which provided such items as listed above. He was not required to participate in a driver training program when he was hired on with the current department. The fire department is currently evaluating its policy on driver training.
Recommendation #5: Ambulance manufacturers, fire and EMS departments, and standards setting bodies, should develop standards and implement policies to reduce the likelihood of material and equipment from becoming projectiles during crash events.
Discussion: Although there is no evidence that the following recommendation would have prevented this fatality, it is being provided based on inspection of the ambulance patient compartment which showed the potential for injuries if a patient or attendant had been in the patient compartment. During this incident, the oxygen cylinder came out of its housing device, cabinets opened up dumping equipment and material, equipment stored on countertops was displaced, the cot came loose from its floor mount and flipped upside down, and coverings for mechanical and electrical compartments came off. Although the patient compartment was unoccupied during this incident, these items became projectiles that may have posed an injury risk to patients and care providers had they been present in the compartment.
Current U.S. ambulance standards address cot and oxygen retention systems and cabinet doors.13 Improvements to these existing standards as well as new standards addressing the crashworthiness of retention systems for other types of equipment such as fire extinguishers, sharps containers, defibrillators, etc., should also be considered. In 2004 the National Registry of Emergency Medical Technicians (NREMT) surveyed the safety habits of 5,533 registered emergency medical technicians (EMTs) and paramedics. Of the 1,773 who responded, 26% reported their defibrillators were rarely or never secured and 9% reported their oxygen cylinders were rarely or never secured.14 Implementation of policies by fire departments and EMS services requiring materials and equipment to be properly stowed and secured within the patient compartment could reduce the potential for injury from loose materials and equipment launched as projectiles during vehicle crashes.
NFPA is in the process of developing NFPA 1917 Standard for Automotive Ambulances, which will focus exclusively on ambulance vehicles and will address many of the same topics referenced within NFPA 1901. NFPA 1917 is being drafted by the Technical Committee and will be available for review and submission of public proposals to the Technical Committee for consideration in July 2010, with publication of an accepted document planned in late 2011. Authorities having jurisdiction will then have an ambulance specific standard for voluntary adoption and utilization in promoting safety of fire fighters, paramedics, and emergency medical technicians.
References
- NFPA [2007]. NFPA 1451 Standard for a fire service vehicle operations training program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1002 Standard for fire apparatus driver/operator professional qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- NSC [2005]. The defensive driving course. 8th ed. Itasca, IL: National Safety Council.
- NSC [2008]. Coaching the emergency vehicle operator II—fire. Itasca, IL: National Safety Council.
- NSC [2008]. Coaching the emergency vehicle operator II—ambulance. Itasca, IL: National Safety Council
- Georgia Motor Vehicles and Traffic Code [2009]. Title 40-6-6. Authorized emergency vehicles.
- Georgia Motor Vehicles and Traffic Code [2009]. Title 40-6-74. Operation of vehicles on approach of authorized emergency vehicles.
- NFPA [2008]. Fire fighter fatalities in the United States—2008. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 Standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- International Association of Fire Fighters [2008]. Fire department standard operating procedure, fire department vehicle safety, emergency and non-emergency response, safety emergency operations on roadways. [http://www.iaff.org/hs/evsp/Vehicle%20Safety%20SOP.pdf] Date accessed: June 2010. (Link Updated 1/28/2013)
- International Association of Fire Chiefs [2007]. Guide to IAFC model policies and procedures for emergency vehicle safety. [http://www.iafc.org/files/1SAFEhealthSHS/VehclSafety_IAFCpolAndProceds.pdf]. Date accessed: June 2010. (Link updated 10/28/2013)
- NFPA [2003]. NFPA 1901 Standard for automotive fire apparatus. 2003 ed. Quincy, MA: National Fire Protection Association.
- GSA [2007]. Federal specification for the star-of-life ambulance. Washington, DC: U.S. General Services Administration, Office of Motor Vehicle Management, KKK-A-1822F.
- Proudfoot S, Moore P, and Levine R [2007]. Safety in numbers: a survey on ambulance patient compartment safety. Journal of Emergency Medical Services, March: 87-90.
Investigator Information
This incident was investigated by Stacy C. Wertman, Safety and Occupational Health Specialist, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. An expert technical review was provided by Kevin Roche, Assistant Fire Marshal of Phoenix Fire Department. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division and James Green, Safety Engineer, Safety Controls Team, Protective Technology Branch, Division of Safety Research, NIOSH located in Morgantown, WV.
Special thanks to the Georgia State Patrol Specialized Collision Reconstruction Team III for their assistance during this investigation.
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
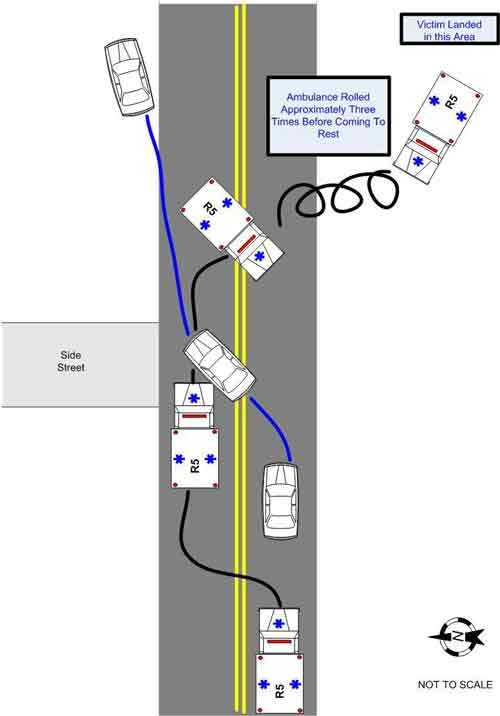
|
Diagram of the incident scene. |
|
The National Institute for Occupational Safety and Health (NIOSH) initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agencys recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim.
|
For further information, visit the program Web site at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
This page was last updated on 03/08/2010.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research