


One Career Fire Fighter/Paramedic Dies and a Part-time Fire Fighter/Paramedic is Injured When Caught in a Residential Structure Flashover Illinois
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2010-10 Date Released: September 13, 2010
Revised on September 30, 2010.
Revised on November 17, 2010.
Executive Summary
On March 30, 2010, a 28-year-old male career fire fighter/paramedic (victim) died and a 21-year-old female part-time fire fighter/paramedic was injured when caught in an apparent flashover while operating a hoseline within a residence. Units arrived on scene to find heavy fire conditions at the rear of a house and moderate smoke conditions within the uninvolved areas of the house. A search and rescue crew had made entry into the house to search for a civilian who was entrapped at the rear of the house. The victim, the injured fire fighter/paramedic, and a third fire fighter made entry into the home with a charged 2 ½ inch hoseline. Thick, black rolling smoke banked down to knee level after the hoseline was advanced 12 feet into the kitchen area. While ventilation activities were occurring, the search and rescue crew observed fire rolling across the ceiling within the smoke. They immediately yelled to the hoseline crew to get out. The search and rescue crew were able to exit the structure safely, then returned to rescue the injured fire fighter/paramedic first and then the victim. The victim was found wrapped in the 2 ½ inch hoseline that had ruptured and without his facepiece on. He was quickly brought out of the structure, received medical care on scene, and was transported to a local hospital where he was pronounced dead.

|
Scene conditions after crews advanced inside. |
Contributing Factors
- Well involved fire with entrapped civilian upon arrival
- Incomplete 360 degree situational size-up
- Inadequate risk-versus-gain analysis
- Ineffective fire control tactics
- Failure to recognize, understand, and react to deteriorating conditions
- Uncoordinated ventilation and its effect on fire behavior
- Removal of self-contained breathing apparatus (SCBA) facepiece
- Inadequate command, control, and accountability
- Insufficient staffing.
Key Recommendations
- Ensure that a complete 360 degree situational size-up is conducted on dwelling fires and others where it is physically possible and ensure that a risk-versus-gain analysis and a survivability profile for trapped occupants is conducted prior to committing to interior fire fighting operations
- Ensure that interior fire suppression crews attack the fire effectively to include appropriate fire flow for the given fire load and structure, use of fire streams, appropriate hose and nozzle selection, and adequate personnel to operate the hoseline
- Ensure that fire fighters maintain crew integrity when operating on the fireground, especially when performing interior fire suppression activities
- Ensure that fire fighters and officers have a sound understanding of fire behavior and the ability to recognize indicators of fire development and the potential for extreme fire behavior
- Ensure that incident commanders and fire fighters understand the influence of ventilation on fire behavior and effectively coordinate ventilation with suppression techniques to release smoke and heat
- Ensure that fire fighters use their self-contained breathing apparatus (SCBA) and are trained in SCBA emergency procedures.

|
View of flashover. |
Introduction
On March 30, 2010, a 28-year-old male career fire fighter/paramedic (victim) died and a 21-year-old female part-time fire fighter/paramedic was injured when caught in an apparent flashover while operating a hoseline within a residence. On March 31, 2010, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On April 14, 2010, a safety and occupational health specialist and a general engineer from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to Illinois to investigate this incident. The NIOSH investigators met with the fire chief, his appointed liaison, and administrative staff. Interviews were conducted with the fire chief, mutual aid fire chiefs and fire fighters who were on scene, and the ambulance crew that treated the victim. The NIOSH investigators also met with local law enforcement to inspect and photograph the victims and injured fire fighter/paramedics structural fire-fighting gear and self-contained breathing apparatus (SCBA) involved in the incident, and a non-damaged SCBA and to review law enforcements witness statements and their preliminary investigative report. The NIOSH investigators visited, documented, and photographed the fire scene and structure. The NIOSH investigators reviewed the victims and injured fire fighter/paramedics training and department medical records, the victims autopsy report, and written radio transcripts from the incident.
The NIOSH investigators returned to Illinois on April 69, 2010, to meet with investigating officials from the Federal Bureau of Alcohol, Tobacco, and Firearms and the Illinois Department of Labor. Interviews were conducted with mutual aid fire fighters on scene, responding members from the victims department, the incident commander (IC), and a village building official. NIOSH investigators also spoke with the fire departments union representative. The NIOSH investigators reviewed training records for the incident commander, radio transcripts, photos and videos taken by bystanders, department standard operating guidelines (SOGs) and general orders, the fire department incident report, and documented SCBA air quality testing results. At the request of the fire department, the NIOSH investigators took possession of the victims and injured fire fighter/paramedics SCBA and structural fire-fighting gear/personal protective equipment (PPE) and transported them to NIOSHs National Personal Protective Technology Laboratory. The SCBA were evaluated to determine conformity to the NIOSH-approved configuration, and both sets of PPE were also examined to determine conformity to the National Fire Protection Association (NFPA) voluntary consensus standards. When finalized, summaries of the SCBA and PPE evaluations will be added as appendices to this report.
Fire Department
This career fire department has one station with 15 full-time and 17 part-time fire fighters who serve a population of approximately 20,000 within an area of about 4 square miles.
Full-time fire fighters work a 24-hour duty shift with 48 hours off, and part-time fire fighters are required to work a minimum of two 12-hour duty shifts a month. Part-time fire fighters may work additional shifts during the month to fill staffing needs. Department members may be assigned to a fire apparatus or an ambulance for the entire 12- or 24-hour duty shift. The fire department currently has 3 engines, 1 aerial ladder, 2 advanced life support ambulances, 1 squad, and 4 support vehicles.
The fire department has written SOGs and general orders regarding such topics as 2-in/2-out, rapid intervention teams (RIT), use of PPE, employee medical evaluation and clearance, responding apparatus and personnel duties, respiratory protection, incident command/management, and response and vehicle staffing.
Mutual Aid Box Alarm System (MABAS)
The fire department is a member of an organization known as the Mutual Aid Box Alarm System (MABAS). MABAS is a mutual aid system designated to assist with mutual aid response of fire, emergency medical services (EMS), specialized response teams, and station coverage during a state declared disaster or when an incident overwhelms the available resources of a participating community. Primarily in the state of Illinois, MABAS has also branched out to additional states such as Wisconsin, Indiana, Iowa, Michigan, and Missouri. Approximately 1,000 fire departments from the state of Illinois have joined this organization. The MABAS requires that all its members agree to and sign an identical contract that includes standards of operation, incident command procedures, minimal equipment staffing requirements, and safety and on-scene terminology. This agreement also aids departments and agencies by having predetermined resources that will be sent from one’s community to assist other communities when in need. This allows the fire chief and incident commanders to focus on operational needs during a serious incident, knowing that a predetermined set of resources is responding upon issuance of a single order by command. Having members agree to the same contract allows departments or agencies from around the state to work together seamlessly.
Apparatus and Staff Response
MABAS agencies are dispatched for response according to predetermined response cards that a community tailors to their individual needs. This department and surrounding village departments had made predetermined auto aid response cards for their initial response, also known as a Still, and for additional resource responses, also known as a Full Still, which included backfills of affected stations. The victims department primarily operated with 4-6 personnel per shift including a lieutenant/acting officer in a command vehicle. Note: The lieutenant/acting officer sometimes needs to ride on an apparatus to fill staffing needs, which is what occurred during this incident. According to the departments SOGs, the minimum staffing requirements were 3 personnel for an engine, aerial ladder, or squad, and 2 paramedics for an ambulance. The type of call and whether the department is first due or assigned as automatic aid determines which apparatus(s) is taken. For example, if this department receives a report of smoke or a structure fire within their first due area, then an engine and an ambulance will respond. The predetermined response card is used by the local dispatch center to dispatch neighboring village departments for additional apparatus to include 1 aerial ladder, 2 additional engines, 1 additional ambulance, and optional apparatus such as an additional aerial ladder or squad, which will fill out the incident assignment. The optional apparatus is dependent on this departments availability of off-duty personnel. If this department is required to respond outside of their first due area then they will provide 3 personnel on the requested apparatus (predetermined by the response card), but if it is a working fire then the departments ambulance will also respond for man power. Note: Ambulance personnel are cross-trained as fire fighters and carry structural fire-fighting gear and SCBA on the ambulance.
At some point during an incident, a determination may be made by the IC, or ranking officer, that the incident can no longer be handled with the resources allotted from the Still and Full Still assignments. When this occurs, MABAS is notified and a Box or Box Alarm is requested. A Box can include two to three engines, one or two ladder trucks, and/or ambulances or specialty teams and equipment. Additional Boxes can be requested such as an EMS Box which will dispatch additional EMS resources such as ambulances to the incident scene.
This incident occurred in the department’s first due area, and they responded with 3 personnel in an engine and 2 personnel in an ambulance. Upon arrival, the ambulance personnel (the victim and injured fire fighter/paramedic) were immediately assigned fire suppression duties by the IC. The incident was upgraded to a “Box” after the flashover occurred and the report of a downed fire fighter.
MABAS Dispatch and Radio Communications
When MABAS is requested to handle extra alarms or a Box, then the local dispatch center will allow MABAS to handle the dispatch control on the Interagency Fire Emergency Radio Network (IFERN). MABAS, over the IFERN frequency, will notify fire dispatch centers of the situation and what resources or equipment are needed according to the predetermined response card. The local dispatch center(s) will then dispatch what is needed through their local frequency. The dispatched resource will then notify MABAS of their response on IFERN, and all further radio communications will be handled through MABAS. Additional color coded fireground channels (e.g., red, green, white) are made available to assist with radio traffic while on the fireground. This incident used the red fireground channel.
Although a written SOG had not been finalized by the time this incident occurred, the chief of this department reported verbally communicating to fire department members a SOG requiring that all incident commanders maintain a non-mobile command post within a vehicle from a visible location (e.g., truck, engine, command car). The fire chief believed having a stationary command post within a vehicle would allow the officer-in-charge, or IC, to monitor all radio channels, specifically, the IFERN and fireground channels. However, at the time of the incident there was a written SOG that had not been repealed that allowed a mobile command operation during nothing showing mode or fast attack mode. Evidence suggests that the fire department may have been operating in the fast attack mode.
Training and Experience
The victim had been hired as a part-time fire fighter/paramedic in August 2008 before accepting a full-time position in December 2009. He went through the departments 6 week (approximate) orientation program while he was part-time. While he was part-time, he also worked for a neighboring department as a fire fighter/paramedic, a total of 3 years. He had received Fire Fighter II and Paramedic certifications from the state of Illinois. He had completed training courses on technical rescue, incident command, and hazardous materials. As a member of this department, he had completed approximately 338 hours of documented training on topics such as SCBA, pre-plans, fire hose and nozzles, fire fighter survival, and emergency medical care. The 338 total hours did not include any fire behavior training. He had also accrued approximately 515 hours of documented training at his previous place of employment, and fire behavior was not documented as being included in those 515 hours.
The injured fire fighter worked part time with this department for approximately 5 years prior to the incident and worked an average of eight 12-hour shifts per month. She had received certifications from the state of Illinois such as Fire Fighter II, Fire Service Instructor I, and Paramedic. She had completed training courses on the incident command system, technical rescue, and hazardous materials. As a member of this department, she had completed approximately 971 hours of documented training on topics such as SCBA, pre-plans, fire hose and nozzles, and emergency medical care. Training on fire behavior accounted for 12 hours of the 971 total hours.
The IC, at the time of incident, had been with this department for approximately 19 years. He had been a lieutenant for the previous 4 years and had 5 years of experience as an IC. In the 1990s, he received certifications from the state of Illinois such as Fire Fighter III, Fire Officer II, Fire Service Instructor II, Certified Fire Investigator, and Fire Apparatus Engineer. He had completed courses in hazardous materials, technical rescue, incident command, incident safety officer, and strategies and tactics. As a member of this department, he had completed approximately 3,830 hours of documented training on topics such as SCBA, pre-plans, search and rescue, fire fighter survival, and emergency medical care. Training on fire behavior accounted for 12 hours of the 3,830 total hours.
Equipment and Personnel
Still (First Alarm) Assignment:
- First due fire department: Engine 534 (E534) with a lieutenant (IC), a fire fighter (FF1), and an engineer. Note: E534 has a 1,500 gallon per minute pump and contains 750 gallons of tank water.
- First due fire department: Ambulance 564 (A564) with 2 fire fighter/paramedics (the victim and the injured fire fighter/paramedic).
- 1st arriving auto aid department: Truck 1220 (T1220) with a lieutenant (FF2), a fire fighter (FF3), a roof man (also a fire fighter), and an engineer.
- 2nd arriving auto aid department: Engine 1340 (E1340) with a lieutenant, three fire fighters, and an engineer.
- 3rd arriving auto aid department: Truck 1145 (T1145) with a lieutenant, two fire fighters, and an engineer.
- 4th arriving auto aid department: Squad 440 (S440) with a lieutenant and three fire fighters.
- First due fire department’s fire chief: Note: Responded from home and arrived after the Mayday.
Note: See Diagram 1 for incident scene and hoselines deployed.
Full Still Assignment:
- Ambulance 2101 (A2101), from nearby village, with two fire fighter/paramedics.
Note: Additional apparatus dispatched with the Full Still assignment are not included because they arrived after the victim was removed from the house.
Timeline
This timeline is provided to set out, to the extent possible, the sequence of events. Times are approximate and were obtained from review of the dispatch records, witness interviews, photographs of the scene and other available information. Times have been rounded to the nearest minute. The timeline is not intended, nor should it be used, as a formal record of events.
- 2055 Hours
Local dispatch center received a 911 call from a resident stating that her paralyzed husbands chair was on fire. - 2057 Hours
Victims and auto aid response fire departments were dispatched for a chair on fire within a residence with a paralyzed subject on oxygen in the chair. The initial Still dispatch included three engines, an aerial ladder, an ambulance, a squad, and fire chief from the victims department. - 2058 Hours
E534 and A564 en route. - 2059 Hours
Officer on E534 requested an all-call for any available personnel from his department.
Police officer on scene reported the house was fully engulfed over the main dispatch channel. S440 en route. - 2100 Hours
T1145 en route.
Police officer on scene reported house was fully engulfed, subject in chair still inside house, and officer unable to get in.
E1340 en route. - 2101 Hours
T1220 arrived on scene and reported a one-story family dwelling involved. Note: No en route time is recorded.
E534 arrived on scene; E534 officer assumed incident command and reported heavy fire showing, and going to red fireground channel.
A564 arrived on scene. - 2103 Hours
E1340 arrived on scene. - 2105 Hours
IC advised local dispatch center that a primary search was underway, crews were beginning to vent, and he requested utilities (to be turned off).
IC requested the local dispatch center to upgrade to a Full Still. - 2106 Hours
T1145 arrived on scene.
S440 arrived on scene. - 2107 Hours
MABAS 24 took control of radio communications from the local dispatch for the Full Still. The Full Still for this incident included an engine for RIT, an ambulance for RIT, a chief of safety, and two changes of station quarters from the auto aid response list. Note: These apparatus arrived after the downed fire fighter (victim) was removed from the house and are not listed within the timeline. - 2109-2110 Hours
IC advised the local dispatch center that the building flashed, with one fire fighter down and a search was commencing.
MABAS 24 and the local dispatch center asked the IC several times if he had a Mayday, with no reply. - 2111 Hours
MABAS 24 upgraded the fire incident to a Box due to a fire fighter missing.
IC requested an EMS Box to his location. - 2113 Hours
A2101 en route to fire scene. Note: This ambulance was part of the Full Still assignment, and they assisted and transported the downed fire fighter (victim) to the hospital. - 2114 Hours
MABAS 24 dispatched and filled Box upgrade from auto aid response departments. Note: Additional apparatus dispatched on the Box upgrade did not have an effect on the incident and are not included. - 2119 Hours
A2101 arrived on scene.
Personal Protective Equipment
It was reported to NIOSH investigators that the victim entered the structure wearing a full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, gloves, boots, and a SCBA with an integrated personal alert safety system (PASS) device, but his Nomex® hood and helmet were unaccounted for when he was located and removed from the structure. Note: Fire fighters interviewed by NIOSH investigators do not recall whether the victim was wearing his Nomex® hood when he entered the house. The victims facepiece was properly connected to his regulator, but when he was found and removed from the structure he was not wearing his facepiece. The victims PASS device was alarming when he was located in the house. It was reported to NIOSH investigators that the injured fire fighter/paramedic was removed from the structure wearing a full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), helmet, Nomex® hood, gloves, boots, and a SCBA with an integrated PASS device. She was still on air when she exited the structure and her PASS device was alarming. Preliminary information provided from NPPTL to NIOSH investigators suggests that the SCBAs and/or PPE evaluated had no direct contribution to the deaths of the two fire fighters. Both sets of turnout gear had their heat-resistant outer shells, moisture barriers, and insulating thermal linings present during the incident and documented during the investigation. NIOSH investigators observed that both sets of turnout gear were directly affected by extreme fire conditions causing thermal degradation of the gear, resulting in thermal injuries to the victim and injured fire fighter/paramedic. When finalized, summaries of the NPPTL SCBA and PPE evaluations will be added as appendices to this report. Both the victim and the injured fire fighter/paramedic were equipped with handheld radios; however, the victims radio was discovered in the back pocket of his station duty pants which made it inaccessible after donning his structural fire-fighting gear.
The fire department maintains their SCBA equipment and compressed breathing air refill system. Several weeks prior to this incident, the fire departments stationary and mobile air refill system was evaluated by a third party. This evaluation found both systems to be in compliance with NFPA 1989-2008 and Compressed Gas Association G-7.1-2004 Grade E standards and regulations.
Structure
Built in 1951, this single family one-story house of Type V wood frame construction contained approximately 950 square feet of living space (see Photo 1 and Diagram 2). A two-car garage of Type V wood frame construction was located at the rear of the house and was connected to the house by an addition (family room) which was added at some point. The house was built on a concrete slab and contained a small attic space. Traditional drywall over interior wood framing was complemented with a brick veneer exterior. Since the house was built it had undergone permitted changes that included a concrete driveway, new windows, and a new asphalt shingled roof. According to the local building official, the addition (see Photo 2) between the garage and house provided additional living space (Type V wood frame construction). There was no recorded permit for this addition.

|

|
Photo 2. Looking from the B-side, photo taken by |
The fire is believed to have originated within the addition, but a cause has not been determined. NIOSH investigators reviewed written witness statements taken from the civilian and the audio 911 call she placed. She was beckoned by her husband when the chair he was sitting in was believed to be on fire. She stated she observed black smoke and flames coming from underneath the chair and she immediately attempted to put the fire out and call 911. Her efforts were unsuccessful. She managed to escape from the house, but her husband perished within the fire. Fuel sources for the fire included polyurethane foam padding, upholstered furniture, a motor vehicle within the garage, and other combustible materials. Also, the civilian victim had three medical oxygen bottles [one D-cylinder (425 liters) and two M-cylinders (34 liters)] within the addition for his personal use. It is not known if the oxygen within these bottles contributed to the growth and behavior of the fire.
Weather
The weather was clear with an approximate temperature of 53°F. Fire personnel at the incident stated wind was not a factor.
Investigation
On March 30, 2010, the victims department and auto aid departments were dispatched for a chair on fire within a residence with a paralyzed subject on oxygen in the chair. Police officers on scene advised incoming fire apparatus that a civilian was still in the house and there was heavy fire to the rear of the home.
T1220 arrived on scene first and reported that the one-story dwelling was involved. FF2 and FF3 immediately received reports from bystanders and police that the trapped civilian was last seen within the family room of the house. Note: This area was fully involved with fire and had spread to the garage which contained a vehicle. Also, the IC may not have been aware of the exact location of the civilian. FF2 and FF3 immediately suited up to gain entry into the house and perform their primary search. As they were walking up to the front A-side door, E534 and A564 arrived on scene (see Diagram 1 ). Upon arrival to the scene, the officer of E534 took command of the incident and gave a brief size-up to dispatch from E534. Note: Prior to arrival, due to the heavy volume of fire viewed from the rear of the structure while still en route to the incident, FF1, the officer (IC), and engineer talked about deploying a 2½-inch hoseline for their initial attack line. The IC, FF1, and engineer on E534 still agreed with the hoseline choice after the E534 was positioned in front of the house, and the IC assisted FF1 in flaking out and taking the hoseline to the front door of the house (A-side). Note: The 2½-inch hoseline with pre-connected smoothbore nozzle was paired with a 1¾-inch hoseline as a skid load, requiring the 1¾-inch section of hose to be disconnected. The IC assisted FF2 and FF3 in breaching the front door. FF2 and FF3 then made entry into the house, without a hoseline, and performed a left-handed search and noted moderate smoke conditions banked down to waist level. The engineer immediately charged the 2½-inch hoseline with tank water and received assistance from T1220s roof man in obtaining a 5-inch water supply from a hydrant located near-by.
The victim and injured fire fighter/paramedic quickly geared up and made their way up to the front door where the IC and FF1 were preparing to make entry into the structure. The IC then paired FF1 with the victim and injured fire fighter/paramedic. Their job was to assist the search and rescue operations being performed by T1220 and fire suppression.
The IC then walked along the B-side of the house towards the C-side to size-up fire conditions. Note: Following this size-up, the IC returned to the front of the house where he became occupied with monitoring multiple radio frequencies on different radios, including the dash-mounted radio in E534.
FF1 took the nozzle, followed by the victim and the injured fire fighter/paramedic who assisted with pulling the hoseline into the house approximately 12 feet (see Diagram 3). FF2 and FF3 passed the hoseline crew in the living room as they continued their search through the living room and towards the D-side. All fire fighters within the structure recall that thick, black smoke had banked down and that the heat within the house was increasing (see Diagram 4).
E1340 arrived on scene and reported directly to command for assignment. They sent one fire fighter to the roof to assist the engineer of T1220 in venting the roof, and additional crew members were tasked with protecting exposures and ventilating windows at ground level. The officer of E1340 retrieved a 1¾-inch hoseline from E534 to protect the D-side exposure. One fire fighter from his crew received orders from the IC to vent the D-side windows and another fire fighter from E1340 was tasked with venting the B-side windows.
While exterior crews were preparing for exposure protection and performing horizontal ventilation, the hoseline crew (FF1, victim, and injured fire fighter/paramedic) had made it into the kitchen when FF1 had to back off the 2½-inch hoseline for a placement issue with his protective hood. Fire was beginning to breach the C-side of the house with thick, black smoke banked down inches from the floor and heat increasing. FF1 advised NIOSH investigators that he handed the nozzle over to the victim and advised him to open and close the bale of the nozzle quickly. FF1 backed out to the front doorway to fix his hood that had exposed some facial area. FF2 and FF3 recall heat intensifying and then going back to the hoseline, but stated they could hear the steam conversion from the nozzle being opened and closed. FF2 and FF3 decided to search the bedrooms on the D-side of the home. It is believed that at the same time this occurred, the D-side window to the back bedroom and B-side window of the kitchen were broken out by crew members from E1340. The injured fire fighter/paramedic remembered hearing someone above her ventilating the roof with a saw. Note: The roof crew was having difficulty making cuts due to smoke and roof material and the roof vent was not able to be louvered open. FF2 and FF3 made it to the front bedroom on the D-side when they felt heat intensify in the hallway and then a rollover occurred at the end of the hallway, coming toward them (see Diagram 5). Note: This hallway led to a bathroom and rear bedroom that had access to the addition. They quickly turned, headed back into the living room looking for the hoseline so they could find their way out, and yelled to the hoseline crew to get out. The injured fire fighter/paramedic did not recall how much fire was within the kitchen, but she felt like she was getting extremely hot. She turned to look behind her and the living room lit up with fire. FF2 and FF3 had just found the hoseline and made it out the front door when the house flashed. The injured fire fighter immediately yelled for the victim, with no response, as she turned around to follow the hoseline out the front door. She stated she made it 4 feet from the door before her gear had melted to the living room carpet. FF2 and FF3 could see her from the front doorway and quickly reentered and pulled her out. Following the flashover, the IC ordered the roof crew down from the roof. The injured fire fighter/paramedic told FF2, FF3, and the IC that the victim was still inside.
The IC grabbed a second 1¾-inch from E534 with assistance from FF1. FF2 and FF3 took the second 1¾-inch hoseline from them and reentered the house to find the victim. Note: The engineer from E534 also deployed his deck gun toward the rear of the house, but he could not reach the fire, so it was repositioned to protect the D-side exposure. The choice to use an elevated master stream was not decided until after the downed fire fighter (victim) was removed from the house. They followed the 2½-inch hoseline into the structure and discovered that it had ruptured. They sprayed water on furniture that was on fire as they made their way to the end of the 2½-inch hoseline. When they made it into the kitchen and laundry area, they discovered the victim entangled in the hoseline and not wearing his helmet or facepiece. They quickly grabbed him and removed him from the house. Members from T1145 assisted with caring for the victim immediately after he was removed. They noticed that he was not wearing his facepiece; however, it was still connected to his regulator. They also noticed that he did not have a hood on. The victim went into respiratory arrest and then lost his pulse. The victim was cared for on scene and prepared for transport well before an additional ambulance had arrived on scene. Once the ambulance arrived on scene he was transported to a local hospital where he was pronounced dead.
Note: The accountability system was never set in place and a personnel accountability report (PAR) was not conducted following the incident.
Fire Behavior
Photos 3-10 show the sequence of changes in fire and smoke conditions during the initial fire suppression and search and rescue efforts. It is believed that crews made entry at approximately 2104 hours. Exact times for changes in the fire and smoke conditions could not be determined, but the flashover occurred within 8 minutes of apparatus arrivalapproximately 2109 per ICs radio traffic.

|
|
Photo 3. Looking toward the A/B corner, the victim, FF1, and injured fire fighter/paramedic are operating the 2 ½ inch hoseline inside the structure, and FF2 and FF3 are searching the house. Crews are preparing to ventilate the roof. Large volume of fire and smoke noted at rear of home, C-side. Thick, black smoke can be scene billowing out the front door, A-side. A-side picture windows are covered in soot. |

|

|

|
|
Photo 6. Looking toward the A/B corner, the fire fighter has vented the B-side kitchen window. Note the horizontal flow of thick, black smoke from window. This is characteristic of being under extreme pressure. Smoke continues to billow from the front door. Crews are still operating inside and on the roof. |

|
|
Photo 7. Looking toward the A/B corner, thick, black smoke continues to push out the B-side window that was vented. The volume of smoke venting from the front door has increased, so has fire on C-side. FF1 can be seen in front doorway. Crews are still operating inside and on the roof. |

|

|

|
|
Photo 10. Looking toward the A-side front door, the flashover has just occurred. FF1 is pulling on the 2½-inch hoseline and FF2 and FF3 are attempting to pull the injured fire fighter/paramedic from the house. She is just inside the door way and the downed fire fighter (victim) is still in the house. (Photo courtesy of Warren Skalski.) |
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Well involved fire with entrapped civilian upon arrival
- Incomplete 360 degree situational size-up
- Inadequate risk-versus-gain analysis
- Ineffective fire control tactics
- Failure to recognize, understand, and react to deteriorating conditions
- Uncoordinated ventilation and its effect on fire behavior
- Removal of self-contained breathing apparatus (SCBA) facepiece
- Inadequate command, control, and accountability
- Insufficient staffing.
Cause of Death and Injury
According to the autopsy report, the victim died from carbon monoxide intoxication due to inhalation of smoke and soot from a house fire. The carboxyhemoglobin (COHb) level for the victim was approximately 30%.
The injured fire fighter/paramedic received 2nd- and 3rd-degree burns to her lower back/buttocks and right wrist.
Recommendations
Recommendation #1: Fire departments should ensure that a complete 360 degree situational size-up is conducted on dwelling fires and others where it is physically possible and ensure that a risk-versus-gain analysis and a survivability profile for trapped occupants is conducted prior to committing to interior fire fighting operations.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial 360 degree situational size-up of the incident. A proper size-up begins from the moment the alarm is received, and it continues until the fire is under control. The size-up should include an evaluation of factors such as the fire size and location, length of time the fire has been burning, conditions on arrival, occupancy, fuel load and presence of combustible or hazardous materials, exposures, time of day, available staffing on scene or en route, and weather conditions. Information on the structure itself should include size, construction type, age, condition (e.g., evidence of deterioration, weathering), renovations, lightweight construction, loads on roof and walls (e.g., air conditioning units, ventilation ductwork, utility entrances), and available preplan information-all key information that can affect whether an offensive or defensive strategy is employed. The size-up should also include a risk-versus-gain assessment during incident operations, especially after primary searches have been conducted1-6, situational awareness, and a survivability profile.
Even before the IC takes command of an incident he will be faced with having to determine what critical tasks are going to have to be performed to bring the incident under control. He will use current knowledge and previous experience to formulate a plan for his arriving apparatus and personnel. When the IC arrives he needs to ascertain as much information as possible to make a determination whether his plan will still work. The IC may be faced with several priorities such as an entrapped civilian, a larger scale incident then previously determined, and the fire environment itself. This is additionally part of the initial situational size-up and the risk assessment, which will constantly change as the incident progresses until it is brought under control. The IC should be willing to prioritize and change his strategy and plan based on these assessments. Situational awareness is a highly critical aspect of human decision making: the understanding of what is happening around you, projecting future situation events, comprehending information and its relevance, being realistic, and an individuals perception.7 Conducting accurate risk assessments and receiving interior/exterior status updates is critical to the safety of fire fighters in the incident, rescue/recovery efforts, and overall control of the incident. The decision to commit interior fire fighting personnel should be made on a case-by-case basis with proper risk-benefit decisions being made by the incident commander. The commitment of firefighters lives for saving property and an unknown or marginal risk of civilian life must be balanced appropriately.8
Another tool that the IC should consider using is survivability profiling. Survivability profiling uses the knowledge learned of fire behavior and spread, smoke (i.e., color, condition, movement), and building construction to examine a situation and make an intelligent decision of whether to commit fire fighters to life saving and/or interior operations.9 In other words, survivability profiling involves assessing the probability that a trapped occupant is still alive and can safely be rescued with the current or impending conditions. The NIOSH publication Preventing Deaths and Injuries of Fire Fighters Using Risk Management Principles at Structure Fires10 states that the IC must make a determination that offensive (interior) operations may be conducted without exceeding a reasonable degree of risk to fire fighters before ordering an offensive attack and must be prepared to discontinue the offensive attack if the risk evaluation changes during the fire fighting operation. The fireground is very dynamic, and conditions can either improve or deteriorate based on fire suppression activities, and available resources. Most importantly, assessments/size-ups of the incident are necessary to detect a change on the fireground.
During this incident, the responding departments were made aware while en route that there was a paralyzed civilian entrapped in the structure. His wife advised 911 and arriving units that the chair he was sitting in caught fire with him still in it. Units arrived on scene 6 minutes after the 911 call to find heavy fire conditions to the addition on the C-side of the house where the entrapped civilian was last seen by his wife sitting in the chair. Prior to a complete 360 degree situational size-up, decisions were made to send a hoseline crew through the A-side front door to assist with search and rescue, and to locate and attack the fire (located on the C-side in the addition and garage). Fire fighters entering the house from the A-side were initially met with moderate smoke conditions banked down to waist level, which quickly changed to thick, black smoke conditions that went to the floor due to the fire being uncontrolled and spreading into the house from the C-side. The victim and injured fire fighter/paramedic were eventually exposed to a flashover. The civilian was not rescued. A full range of factors must be considered in making the risk evaluation including a realistic evaluation of the ability to execute a successful offensive fire attack with the resources that are available and a realistic evaluation of occupant survivability and rescue potential.10
Fire departments should be aware of the recently released 2010 International Association of Fire Chiefs (IAFC) Rules of Engagement (ROE) of Structural Firefighting.11 These guidelines recommend that ICs conduct or obtain a 360 degree situational incident size-up, determine the occupant survival profile, and conduct an initial risk assessment.
Recommendation #2: Fire departments should ensure that interior fire suppression crews attack the fire effectively to include appropriate fire flow for the given fire load and structure, use of fire streams, appropriate hose and nozzle selection, and adequate personnel to operate the hoseline.
Discussion: An assessment and decision of suppression methods must be made before attacking a fire in hopes of extinguishing it and keeping fire fighters safe while doing so. To accomplish such tasks, ICs, officers, and fire fighters need to consider such factors as fire load and flow, hose and nozzle selection, placement and use of fire streams, and required staffing. Fire load, or heat released from combustible materials, will directly affect how the fire develops throughout the incident and how long and severely it may burn. The more combustible materials involved, the greater the heat that will be produced requiring additional fire flow. Fire flow is the calculated amount of water in gallons per minute needed to extinguish a fire in a specific structure. To assist fire fighters in calculating the fire flow, one of three formulas could be used: the Iowa Rate-of-Flow Formula, the National Fire Academy (NFA) Formula, and the Insurance Services Office Formula. The Iowa Rate-of-Flow and NFA Formulas were designed to be used on the fireground because they allow fire fighters to mentally compute the fire flow with relative ease by estimating such things as the square footage (area) of a structure or the cubic footage (volume) of a room, and percentage involved, then inputting that data into a predetermined formula.12
Iowa Rate-of-Flow Formula:
rate of fire flow=volume of room in cubic feet÷100
NFA Formula:
fire flow in gallons per minute for one floor at 100% involvement=(length ×width)÷3
If less than 100% involvement,then multiply answer by estimated percentage of involvement.
The fire stream, or water stream, is an important aspect both for fire fighter safety and tactical considerations. The wrong choice of fire stream can place a fire fighter and crew in a bad situation. Also, the wrong type of fire stream will affect the tactical outcome of the incident in regards to how quickly the fire is controlled. To produce an effective fire flow, there must be a viable water supply; sufficient water pressure; a means to transport the stream to the desired point (fire); and trained, competent personnel to deploy these three elements.12 These elements are applied through the use of a fire hose and nozzle. The diameter of the fire hose can affect how much water is flowed on a fire, but the larger the diameter, the more potential to max out the delivering pumps capacity, and additional personnel will be needed to handle the hoseline. The nozzle will allow the water to leave its mechanical hold within the hoseline to produce the desired fire stream. Typical fire streams include solid, fog, and broken, and each have their own characteristics, advantages/disadvantages, and application. Proper training on all these aspects will greatly influence fire fighters knowledge on the fireground, provide for quicker control and extinguishment of the fire, and increase overall fire fighter safety.
During this incident, arriving fire departments were faced with a large volume of fire and an entrapped civilian. Prior to the flashover, the fire was burning uncontrolled at the rear of the house (house addition and garage) and spreading into the house. FF1, the victim, and injured fire fighter/paramedic were tasked with advancing a charged 2½-inch hoseline into the house to assist with the search and for fire suppression. They were able to advance this hoseline approximately 12 feet into the house, but advancing and operating a large-diameter hoseline within tight quarters may be extremely cumbersome even if adequate staffing is available to accomplish this task. Note: When FF1 had a problem with his PPE, he handed the nozzle over to the victim, and eventually backed out of the structure, that left only two personnel available to operate the hoseline. Fire fighters and officers need to understand that while a 2½-inch hoseline provides a greater flow, fire fighters need to be able to move the line quickly and efficiently interiorly, especially when performing a search and experiencing deteriorating fire conditions. An alternate decision to advancing the 2½-inch hoseline into the small house could have been to deploy and advance a 1¾-inch hoseline(s), which would have been easier to maneuver within the house.
Due to the large volume of fire at the C-side that was extending into the house, the 2½-inch hoseline(s) could have been deployed exteriorly to the B- and/or D-sides to combat the fire, paying close attention to directly attack the fire, an elevated master stream (carefully directed on fire burning uncontrolled within the addition and garage) could have been deployed early into the fire had the assessment been made that the entrapped civilian (last reported to be in the addition) could not be saved, thus possibly stopping further progression of fire and volatile smoke into the house. Additionally, a lightweight portable master stream, placed exteriorly at the B- and/or D-sides, which is fairly easy to deploy by using a 2½- to 3-inch supply line, may only require one fire fighter to operate once in position. These types of water delivery appliances are capable of delivering a large volume of water that will assist in extinguishing the fire from an exterior position, especially when conditions are deteriorating interiorly, which could place fire fighters safety at risk.
An incident commander needs to constantly assess whether his strategies and tactics to control and extinguish the fire are working, paying close attention to fire and smoke conditions/changes, the affects from ventilation performed by fire fighters and occurring naturally as the fire progresses, and to fire fighter safety.
Recommendation #3: Fire departments should ensure that fire fighters maintain crew integrity when operating on the fireground, especially when performing interior fire suppression activities.
Discussion: Fire fighters should always work and remain in teams whenever they are operating in a hazardous environment.1 Team integrity depends on team members knowing who is on their team and who is the team leader; staying within visual contact at all times (if visibility is low, teams must stay within touch or voice distance of each other); communicating needs and observations to the team leader; and rotating together for team rehab, team staging, and watching out for each other (e.g., practicing a strong buddy system). Following these basic rules helps prevent serious injury or even death by providing personnel with the added safety net of fellow team members. Teams that enter a hazardous environment together should leave together to ensure that team continuity is maintained.2 The 2010 IAFC ROE of Structural Firefighting states, Go in together, stay together, come out together. 11
Recommendation #4: Fire departments should ensure that fire fighters and officers have a sound understanding of fire behavior and the ability to recognize indicators of fire development and the potential for extreme fire behavior.
Discussion: Reading fire behavior indicators and recognizing fire conditions serve as the basis for predicting likely and potential fire behavior. Reading the fire requires recognition of patterns of key fire behavior indicators. It is essential to consider these indicators together and not to focus on the most obvious indicators or one specific indicator (e.g., smoke).13, 14 Identifying building factors, smoke, wind direction, air movement, heat and flame indicators are all critical to reading the fire. Focusing on reading smoke may result in fire fighters missing other critical indicators of potential fire behavior. One important concept that must be emphasized is that smoke is fuel and must be viewed as potential energy. Smoke that is thick, black and pressurized can emit from a structure at a high rate. This is indicative of a potentially under-ventilated structure or a ventilation controlled fire. This smoke is fuel-rich and is termed black fire. It can potentially do as much damage as fire itself, but it is an indicator that some type of extreme fire behavior may occur.
Since the IC should be staged at a designated command post (outside), the interior conditions should be communicated by interior company officers (or the member supervising the crew) as soon as possible to their supervisor (e.g., IC, division supervisor). Knowledge of interior conditions could change the ICs strategy or tactics. Interior crews can aid the IC in this process by providing reports of the interior conditions as soon as they enter the fire building and by providing regular updates. In addition to the importance of communicating reports on fire conditions, it is essential that fire fighters recognize what type of information is important. Command effectiveness can be impaired by excessive and extraneous information as well as from a lack of information. In the case of communicating observations related to fire behavior, this requires development of fire fighters skill in recognition of key fire behavior indicators and reading the fire.
During this incident, FF1 made a decision to quickly open and close the smooth bore nozzle (water applied as a solid stream) while aiming at the ceiling. It is believed this was done in an attempt to cool the thermal (hot gas) layer, a common practice, in hopes of preventing a potential flashover. Ceiling temperatures can be reduced through carefully considered fire control actions, such as applying short bursts of water spray into the hot gas layer, or directly applying water onto the fire itself which will limit the release of unburned products of combustion as well as reduce ceiling temperature.1
Also, the search and rescue crew (operating without the protection of a hoseline) were able to make a quick determination that the conditions within the house were imminent to flashover. They made an attempt to alert the victim and injured fire fighter/paramedic, but were too late. If conditions are right for a flashover, there are only seconds to make a decision. Fire fighters will be met with a sudden increase in heat and rollover within the ceiling level. The injured fire fighter/paramedic was unaware that the conditions she was operating in deteriorated quickly. She remembers thick, black smoke pushing down to the floor while in the structure and then the room and everything in it caught fire. Prior to the flashover, windows on the B-side were vented and thick, black and heavily pressurized smoke billowed from these windows. The IC, and individuals working on the exterior, need to recognize this as a potential for extreme fire behavior and evacuate interior crews. Obtaining proper training and hands-on experience through the use of a flashover simulator may assist interior fire fighters in making sound decisions on when to evacuate a structure fire.
Recommendation #5: Fire departments should ensure that incident commanders and fire fighters understand the influence of ventilation on fire behavior and effectively coordinate ventilation with suppression techniques to release smoke and heat.
Discussion: Ventilation is the systematic removal of heated air, smoke, and fire gases from a burning building and replacing them with cooler air.1 The two types of ventilation are vertical and horizontal. During vertical ventilation the natural convection of the heated gases creates upward currents that draw the fire and heat in the direction of the vertical opening. Horizontal ventilation allows for heat, smoke, and gases to escape by means of a doorway or window but is highly influenced by the location and extent of the fire, and special caution should be taken if the fire is in the attic.1
Properly coordinated ventilation can decrease the rate the fire spreads, increase visibility, and lower the potential for flashover or backdraft. Proper ventilation reduces the threat of flashover by removing heat before combustibles in a room or enclosed area reach their ignition temperatures. Proper ventilation can reduce the risk of a backdraft by reducing the potential for superheated fire gases and smoke to accumulate in an enclosed area. Properly ventilating a structure fire will reduce the tendency for rising heat, smoke, and fire gases, trapped by the roof or ceiling, to accumulate, bank down, and spread laterally to other areas within the structure. The ventilation opening may produce a chimney effect, causing air movement from within a structure toward the opening. These air movements help facilitate the venting of smoke, hot gases, and products of combustion but may also cause the fire to grow in intensity and may endanger fire fighters who are between the fire and the ventilation opening. For this reason, ventilation should be closely coordinated with hoseline placement and offensive fire suppression tactics. Close coordination means the hoseline is in place and ready to operate, so that when ventilation occurs, the hoseline can overcome the increase in combustion, which is likely to occur. If a ventilation opening is made directly above a fire, fire spread may be reduced, allowing fire fighters the opportunity to extinguish the fire. If the opening is made elsewhere, the chimney effect may actually contribute to the spread of the fire.1
ICs and fire fighters need to consider the following and how it will affect ventilation and overall control of the fire:
- Who will ventilate (knowledge and skills)?
- What type of ventilation?
- When to ventilate?
- Where to ventilate?
- Why ventilate?
- How to properly and safely ventilate?
- What are the expected results from ventilation?
Fire development in a compartment may be described in several stages, although the boundaries between these stages may not be clearly defined.1 The incipient stage starts with ignition, followed by growth, fully developed, and decay stages. The available fuel largely controls the growth of the fire during the early stages. This is known as a fuel-controlled fire, and ventilation during this time may initially slow the spread of the fire as smoke, hot gases, and products of incomplete combustion are removed. As noted above, increased ventilation can also cause the fire to grow in intensity as additional oxygen is introduced. Effective application of water during this time can suppress the fire but if the fire is not quickly knocked down, it may continue to grow.
If the fire grows until the compartment approaches a fully developed state, the fire is likely to become ventilation controlled. Further fire growth is limited by the available air supply as the fire consumes the oxygen in the compartment. Ventilating the compartment at this point will allow a fresh air supply (with oxygen to support combustion), which may accelerate the fire growth, resulting in an increased heat release rate. If coordinated fire suppression activities do not quickly decrease the heat release rate, a ventilation induced flashover can occur.1 Considering that most fires beyond the incipient stage are or will quickly become ventilation controlled, changes in ventilation are likely to be some of the most significant factors in changing fire behavior.
During this incident, uncoordinated ventilation occurred while the hoseline and search and rescue crews were inside the house. The victim and other fire fighters, within the small house, were between the fire and the ventilation source. One fire fighter accounts heavy, turbulent, black smoke pushing from a window on the B-side after it was broken. Shortly after, the house sustained an apparent ventilation-induced flashover.
Recommendation #6: Fire departments should ensure that fire fighters use their self-contained breathing apparatus (SCBA) and are trained in SCBA emergency procedures.
Discussion: Fire fighters are tasked at times to operate within environments which pose inhalation hazards (e.g., toxic smoke and oxygen deficiency),15 defined by the Occupational Safety and Health Administration (OSHA) as immediately dangerous to life and health (IDLH). Proper training along with an implemented and enforced policy or procedure will assist fire fighters with proper maintenance, use, and removal of a SCBA. OSHA 29 CFR 1910.134 (g)(4)(iii) states, The employer shall ensure that all employees engaged in interior structural firefighting use SCBAs.16
According to the autopsy report, the victim died from carbon monoxide intoxication due to inhalation of smoke and soot. The medical examiner also indicated that the victims COHb level (a measure of carbon monoxide in the bloodstream) was 30%. Even if nothing but carbon dioxide, water vapor, and nitrogen were present in the fire products and these were to mix with the air being breathed by a fire fighter, then the oxygen percentage would be reduced below the normal 21%. At 15% oxygen, fire fighters can experience lethargy, poor coordination, and confused thinking. The two principal toxins in smoke—carbon monoxide and hydrogen cyanide—act to deprive the brain of oxygen, and their effects would be enhanced due to the lower levels of oxygen in the air.17 The victim was discovered with his facepiece off, but still connected to his regulator. Due to the smoke conditions, the victim would have had to have been on air when entering the structure. It has not been determined why the victim was found without his facepiece on.
Emergencies created by, or associated with, SCBA can be overcome in several ways. Fire departments can develop and implement a comprehensive respiratory protection program18 that includes fire fighter fitness, training, and competency and skill assessments in SCBA and emergency procedures. Firefighters should remember the first rule in any emergency situation-to not panic. Panic causes an increased breathing rate and consequently, an increase in air consumption; and an inability to focus on emergency procedures. If fire fighters become lost, trapped, or disoriented, they need to focus on managing remaining air in their SCBA cylinder until other fire fighters can make a rescue attempt. Removing ones facepiece in an IDLH atmosphere can immediately expose the respiratory system to a potentially fatal environment, thus incapacitating an individual. Choosing to leave ones SCBA facepiece on may be the best chance in providing additional time for a fire fighter to be rescued. Fire fighters should follow their departments SOPs regarding emergency SCBA procedures and emergency communications.
Recommendation #7: Fire departments should ensure that adequate staffing is available to respond to emergency incidents.
Discussion: NFPA 1710 Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Career Fire Departments contains recommended guidelines for minimum staffing of career fire departments.19 NFPA 1710 states the following: On-duty fire suppression personnel shall be comprised of the numbers necessary for fire-fighting performance relative to the expected fire-fighting conditions. These numbers shall be determined through task analyses that take the following factors into consideration:
- Life hazard to the populace protected.
- Provisions of safe and effective fire-fighting performance conditions for the fire fighters.
- Potential property loss.
- Nature, configuration, hazards, and internal protection of the properties involved.
- Types of fireground tactics and evolutions employed as standard procedure, type of apparatus used, and results expected to be obtained at the fire scene.
The NFPA standard states that both engine and truck companies shall be staffed with a minimum of four on-duty personnel. The standard also states that companies shall be staffed with a minimum of five or six on-duty members in jurisdictions with tactical hazards, high-hazard occupancies, high-incident frequencies, geographical restrictions, or other pertinent factors identified by the authority having jurisdiction.
During this incident, the victims department responded with three personnel on the engine and two personnel on the ambulance, but the Still assignment also consisted of an engine, two ladder trucks, and a squad, with four fire personnel on each. It was routine to have an ambulance respond with an engine on a first due fire assignment. Due to short staffing, the ambulance personnel were tasked with fire suppression activities, thus taking them out-of-service as a medical unit. Also, due to short staffing, the lieutenant/acting officer (IC) was required to ride and operate as the officer of E534. This removed him from his command response vehicle which would have allowed him to command at a tactical level versus having to potentially perform tasks.
Recommendation #8: Fire departments should ensure that staff for emergency medical services is available at all times during fireground operations.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. Emergency medical care and transportation for injured or ill fire fighters should be immediately available on the scene of working structure fires. Many fire departments incorporate an automatic dispatch of an EMS unit to working structure fires. Automatic dispatch can help to ensure that qualified emergency medical care and transportation for injured or ill fire fighters is available without having to call and wait for a unit after a medical emergency or injury has occurred.
During this incident, the victim and the injured fire fighter/paramedic responded in an ambulance. Upon their arrival to the scene, the IC immediately tasked them with interior operations due to staffing issues. The IC did not request an additional ambulance to respond to the scene for medical care until after the victim was down within the house. Additional resources (e.g., apparatus and personnel) arrived minutes after the ambulances arrival.
Recommendation #9: Fire departments and dispatch centers should ensure they are capable of communicating with each other without having to monitor multiple channels/frequencies on more than one radio.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. It is important that fire service personnel have an efficient means of communicating during an emergency incident. The use of radio communications provides fire fighters on scene with the ability to communicate to individuals they cannot see or to receive vital information about the incident. To assist with this, localities should ensure that communications can occur without having to utilize different radios and/or monitor multiple channels/frequencies.
During this incident, the IC had to monitor more than one radio and even had to go to the cab of his engine to accomplish this task. Having to monitor multiple radios and potentially take your eyes off the scene for a moment could be extremely detrimental to the management of the incident.
Recommendation #10: Fire departments should ensure that the incident commander, or designee, maintains close accountability for all personnel operating on the fireground.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. The use of an accountability system is recommended by NFPA 1500 Standard on Fire Department Occupational Safety and Health Program20and NFPA 1561 Standard on Emergency Services Incident Management System.21 A functional personnel accountability system requires the following:
- Development of a departmental SOP
- Training all personnel
- Strict enforcement during emergency incidents
As the incident escalates, additional staffing and resources may be needed, adding to the burden of tracking personnel. At this point, an accountability system should be in place which includes an incident command board that is established and maintained by an assigned accountability officer or aide. A properly maintained incident command board allows the IC to readily identify the location and time of all fire fighters on the fireground. As a fire escalates and additional fire companies respond, a chiefs aide or accountability officer assists the IC with accounting for all fire fighting companies at the fire, at the staging area, and at the rehabilitation area. The personnel accountability report (PAR) is an organized on-scene roll call in which each supervisor reports the status of his crew when requested by the IC or emergency dispatcher.1 A properly initiated and enforced accountability system on every response, which is consistently integrated into fireground command and control, enhances fire fighter safety and survival by helping to ensure a more timely and successful identification and rescue of a disoriented or downed fire fighter.
During this incident, the accountability system was never set in place and a PAR was not conducted following the Mayday.
Recommendation #11: Fire departments should ensure that fire fighters wear a full array of turnout clothing and personal protective equipment appropriate for the assigned task while participating in fire suppression.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. NFPA 1500 Standard on Fire Department Occupational Safety and Health Program states, The fire department shall provide each member with protective clothing and protective equipment that is designed to provide protection from the hazards to which the member is likely to be exposed and is suitable for the tasks that the member is expected to perform protective clothing and protective equipment shall be used whenever a member is exposed or potentially exposed to the hazards for which the protective clothing (and equipment) is provided.20 NFPA 1971 Standard on Protective Ensembles for Structural Fire Fighting and Proximity Fire Fighting has established minimum requirements for structural fire fighting protective ensembles and ensemble elements designed to provide fire fighting personnel limited protection from thermal, physical, environmental, and bloodborne pathogen hazards encountered during structural fire fighting operations.22These requirements will assist in protecting firefighters, but only if they wear the PPE as recommended by the manufacturer.
During this incident, the victim was discovered without a hood over his head or rolled down on his neck. NIOSH investigators could not determine whether this equipment was properly donned prior to the incident.
Recommendation #12: Fire departments should ensure that a separate incident safety officer, independent from the incident commander, is appointed at each structure fire.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. According to NFPA 1561 Standard on Emergency Services Incident Management System,21 The incident commander shall have overall authority for management of the incident and the incident commander shall ensure that adequate safety measures are in place. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the incident commander is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.21 According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program,20 as incidents escalate in size and complexity, the incident commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) to assess the incident scene for hazards or potential hazards. These standards indicate that the incident commander is in overall command at the scene but acknowledge that oversight of all operations is difficult. On-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO. Additionally, the incident commander relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk versus gain and offensive-versus-defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and the incident commander. NFPA 1521 Standard for Fire Department Safety Officer defines the role of the ISO at an incident scene and identifies duties such as recon of the fireground and reporting pertinent information back to the incident commander; ensuring the departments accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.23 Larger fire departments may assign one or more full-time staff officers as safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the incident commander. The presence of a safety officer does not diminish the responsibility of individual fire fighters and fire officers for their own safety and the safety of others. The ISO adds a higher level of attention and expertise to help the fire fighters and fire officers. The ISO must have particular expertise in analyzing safety hazards and must know the particular uses and limitations of protective equipment.3
Recommendation #13: Fire departments should ensure that all fire fighters are equipped with a means to communicate with fireground personnel before entering a structure fire.
Discussion: Although there is no evidence that this recommendation would have prevented this fatality, it is being provided as a reminder of a good safety practice. NFPA 1561 Standard on Emergency Services Incident Management System states, To enable responders to be notified of an emergency condition or situation when they are assigned to an area designated as immediately dangerous to life or health (IDLH), at least one responder on each crew or company shall be equipped with a portable radio and each responder on the crew or company shall be equipped with either a portable radio or another means of electronic communication.21 Radio communications on the fireground are imperative for the IC to command and control the incident and for fire fighters to work effectively and safely within a structure fire. Fire fighters within a structure are unable to see all areas affected by fire and whether the structure is maintaining its stability. Having radio communications can enhance fire fighter safety and health by providing fire fighters a means to communicate with other crew members or with the IC when they find themselves in need of assistance.
During this incident, the victim did have a radio, but it was positioned in the back pocket of his station pants. Thus, when he donned his bunker pants, his radio became inaccessible during the incident.
Recommendation #14: The National Fire Protection Association (NFPA) should consider developing more comprehensive training requirements for fire behavior to be required in NFPA 1001 Standard for Fire Fighter Professional Qualifications and NFPA 1021 Standard for Fire Officer Professional Qualifications.
Discussion: Structural fires frequently display indicators and warning signs of rapid fire development such as flashover, backdraft, and fire gas ignition for which many fire fighters and officers may not have been sufficiently trained to recognize or understand. It is imperative that fire fighters and officers develop the understanding and skills necessary to identify and interpret the indicators so that they can anticipate the potential for extreme fire behavior and immediately communicate their findings to the IC. 1, 24 This requires comprehensive training in fire behavior (theory) and practical application inclusive of realistic live fire training. 1, 25
NFPA 1001 Standard for Fire Fighter Professional Qualifications26 and NFPA 1021 Standard for Fire Officer Professional Qualifications27 were developed to ensure that fire fighters and officers have the skills necessary to perform their job, also known as job performance requirements (JPRs). Currently, these JPRs include language that individuals have requisite knowledge on such topics as heat transfer, principles of thermal layering, advantages and disadvantages of different types of ventilation, and fire behavior in a structure. These standards do not include guidance on how many hours or what available scientific information will be used to verify that an individual has a sound understanding of the physical, chemical, and thermal behavior of fire and how to make a connection between fire dynamics/behavior and the influence of tactical operations (e.g., fire flow, types of ventilation) and external factors (e.g., wind). These JPRs are taken by curriculum developers and formatted into educational content. Standard setting agencies, states, curriculum developers, and other authorities having jurisdiction should consider developing a nationwide curriculum so that fire fighters and officers receive fundamental and refresher training on how to: recognize and interpret fire behavior and indications of impending extreme fire behavior (e.g., flashover, back draft, smoke explosion); and, anticipate what could or should happen when a tactical operation is performed (e.g., ventilation, fire flow). Standard setting agencies and curriculum developers should also consider providing guidelines (e.g., required topics and hours) for instructors to deliver such information and recommendations for verifying an individuals learning and retention.
According to documented training reviewed by NIOSH investigators, the victim, injured fire fighter/paramedic, and IC had a combined 24 hours of fire behavior training out of 5,654 total combined training hours. Additional fire behavior training to include such areas as theory, chemistry, physics, smoke reading, current research, and the cause and effects of tactics during fire suppression operations may improve fire fighter safety.
References
- IFSTA [2008]. Essentials of fire fighting. 5th ed. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and control of fires and emergencies. Saddle Brook, NJ: Fire Engineering Book and Videos.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Dunn V [1998]. Risk management and lightweight truss construction. With New York Firefighters (WNYF) 58(1).
- NIOSH [1999]. NIOSH alert: request for assistance in preventing injuries and deaths of firefighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 99-146.
- Endsley MR, Garlan J [2000]. Situational awareness analysis and measurement. Mahwah, NJ: Lawrence Erlbaum Associate.
- Jones J [2001]. No empty threat. Fire Chief Nov 1 [http://firechief.com/mag/firefighting_no_empty_threat]. Date accessed: September 2010. (Link Updated 1/28/2013)
- Marsar S [2010]. Survivability profiling: are the victims savable? Fire Engineering Apr 4. [http://www.fireengineering.com/articles/2009/12/survivability-profiling.html]. Date accessed: June 2010. (Link Updated 1/28/2013)
- NIOSH [2010]. NIOSH alert: preventing deaths and injuries of fire fighters using risk management principles at structure fires. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 2010-153.
- IAFC Safety, Health, and Survival Section [2010]. Rules of Engagement of Structural Firefighting. [http://www.iafcsafety.org]. Date Accessed: September 2010.
- Wieder M [2005]. Fire service hydraulics and water supply. Stillwater, OK: Fire Protection Publications.
- Grimwood P, Hartin E, McDonough J & Raffel S [2005]. 3D firefighting: training, techniques, and tactics. Stillwater, OK: Fire Protection Publications.
- Hartin E [2009]. Reading the Fire: Building Factors. Fire behavior indicators-a quick review. [http://cfbt-us.com/wordpress/?p=620]. Date accessed: June 2010.
- Klinoff R [2003]. Introduction to fire protection. 2nd ed. Clifton Park, NY: Thomas Delmar Learning.
- Occupational Safety and Health Administration (OSHA). 29 CFR 1910. 134 Respiratory Protection [https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=12716]. Date accessed: June 2010.
- Friedman R [1998]. Principles of fire protection chemistry and physics. Quincy, MA: National Fire Protection Association.
- NFPA [2006]. NFPA 1404 standard for fire service respiratory protection training. 2006 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2010]. NFPA 1710 standard for the organization and deployment of fire suppression operations, emergency medical operations, and special operations to the public by career fire departments. 2010 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1561 standard on emergency services incident management system. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1971 standard on protective ensembles for structural fire fighting and proximity fire fighting. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521 standard for fire department safety officer. 2008ed. Quincy, MA: National Fire Protection Association.
- Firetactics.com [2007]. Rapid fire phenomenon. [http://www.firetactics.com/RAPID%20FIRE%20PHENOMENA%202007.pdf]. Date accessed: June 2010.
- Firetactics.com [1999]. Realistic live fire training to deal safely with flashover and backdraft. [http://www.firetactics.com/SHAN%20RAFFEL%20IFE.htm]. Date accessed: June 2010.
- NFPA [2008]. NFPA 1001: standard for firefighter professional qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1021: standard for fire officer professional qualifications. 2003 ed. Quincy, MA: National Fire Protection Association.
Investigator Information
This investigation was conducted by Stacy C. Wertman, Safety and Occupational Health Specialist, and Matt Bowyer, General Engineer, with the Fire Fighter Fatality Investigation and Prevention Program, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. This report was authored by Stacy C. Wertman. An expert technical review was provided by Deputy Fire Chief William Goldfeder of the Loveland-Symmes (OH) Fire Department and editor of www.FireFighterCloseCalls.com. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Tom Pouchot, NIOSH General Engineer, National Personal Protective Technology Laboratory, conducted an evaluation of the victims and injured fire fighter/paramedics SCBA. Angie Shepherd, NIOSH General Engineer, National Personal Protective Technology Laboratory, conducted an evaluation of the victims and injured fire fighter/paramedics protective clothing.
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
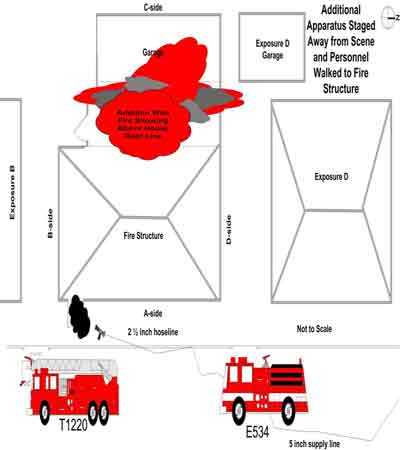
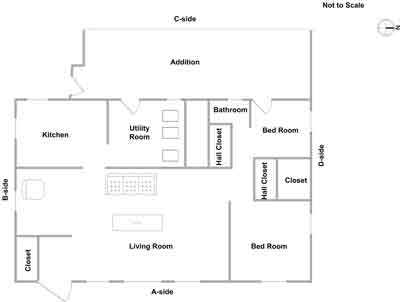
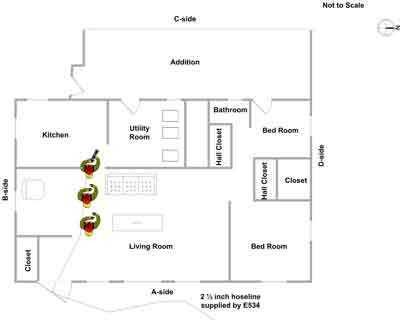
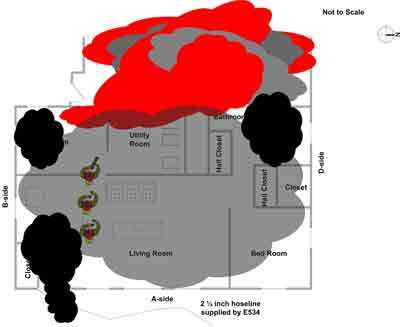
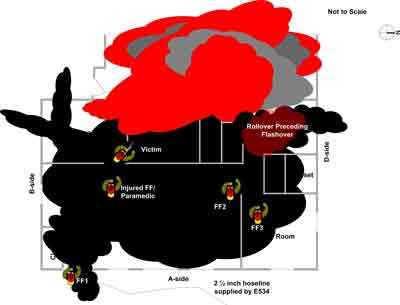
APPENDIX
Status Investigation Report of Two
Self-Contained Breathing Apparatus
NIOSH Task Number 16968
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate two SCBA identified as MSA, 4500 psi, 30-minute, self-contained breathing apparatus (SCBA). This SCBA status investigation was assigned NIOSH Task Number 16968. The fire department was advised that NIOSH would provide a written report of the inspections and any applicable test results. The SCBAs, contained within two large evidence paper bags, were delivered to the NIOSH facility in Bruceton, Pennsylvania on April 12, 2010. After its arrival, the packages were taken to building 108 and stored under lock until the time of the evaluation.
SCBA Inspection
The packages were opened in the Firefighter SCBA Lab Area (building 37) and a complete visual inspection was conducted by Eric Welsh, Engineering Technician, NPPTL. The first SCBA was inspected on August 2, 2010 and was designated as Unit #1. The second SCBA, designated Unit
#2 was opened and inspected on August 4, 2010. The SCBAs were examined, component by component, in the condition as received to determine their conformance to the NIOSH-approved configuration. The visual inspection process was photographed. The SCBAs were identified as the model FireHawk M7 Airmask, 30 minute, 4500 psi units, NIOSH approval no. TC-13F-548CBRN. The condition of each major component was also photographed with a digital camera. It was judged that these units could be safely pressurized and tested using a substitute cylinder for Unit #2 only.
SCBA Testing
The purpose of the testing was to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the SCBA’s conformance to the National Fire Protection
Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-
Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of
42 CFR 84):
- Positive Pressure Test [§ 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [§ 84.95]
- Static Pressure Test [§ 84.91(d)]
- Gas Flow Test [§ 84.93]
- Exhalation Resistance Test [§ 84.91(c)]
- Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981,
1997 Edition):
- Air Flow Performance Test [Chapter 5, 5-1.1]
Units # 1 and # 2 were tested on August 9 and August 23, 2010 using a substitute cylinder for Unit #2. The inspection of the units was documented by photographic means.
Summary and Conclusions
Two SCBA were submitted to NIOSH by the fire department and police department for evaluation. The SCBA were delivered to NIOSH on April 12, 2010 and the inspection and testing were completed on August 23, 2010. The units were identified as the MSA FireHawk M7 Airmask, 4500 psi, 30-minute, SCBA (NIOSH approval number TC-13F-548CBRN). Both units have suffered some heat damage, exhibited other signs of general wear and tear, along with the presence of dirt, grime, foreign particulate material and soot. The cylinder valves as received were in the open position on both units. The gauge read zero pressure for Unit #1. The cylinder gauge for Unit #2 was damaged by heat and was un-readable. The regulator and facepiece mating and sealing areas on both units were relatively clean and there was a small amount of debris inside the facepiece of Unit #1. The outside of the Unit #1 facepiece had the presence of excessive dirt and grime. Unit # 2 did not have the communications system mounted onto the facepiece, only the unit bracket was present. The harness webbing was in generally good condition with only some minor evidence of wear and slight heat damage. The PASS devices on both units did not function upon initial inspection. The PASS performed properly on Unit #1 only after the batteries were replaced. The batteries on the Unit #2 PASS could not be checked or replaced as the power module battery compartment was damaged by heat and could not be opened. The NFPA approval label on Unit # 1 was slightly abraded and the NFPA edition could not be determined. Visibility through the lens of Unit # 1 was fair and visibility through the lens of Unit #2 was fair to good. The air cylinder on Unit # 1 had a manufacture date of 7/08. The air cylinder on Unit # 2 had a manufacture date of 7/08. Under the applicable DOT-E-10945-4500 exemption, these air cylinders are required to be re-tested every 5 years after July 1, 2008. Therefore it appears that the cylinders on these units were due for re-hydro testing before the end of July, 2013 and these cylinders were within the required certification time. The Unit # 2 cylinder also was heavily damaged and gouged exposing the composite material. The Unit #1 cylinder was in good condition with the exception of the presence of dirt and grime, and was utilized for the testing of both units. No other maintenance or repair work was performed on the units at any time.
Unit # 2 failed to meet the requirements of the NIOSH Static Pressure Test, Exhalation Resistance Test and the Remaining Service Life Indicator Test. Both units failed to meet the requirements of the NFPA Air Flow Performance Test as the electronic end of service time indicators for the units failed to operate.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part at this time. Following inspection and testing, the SCBA were returned to storage pending return to the fire department.
If the units are to be placed back in service, they must be repaired, tested, and inspected by a qualified service technician, including such testing and other maintenance activities as prescribed by the schedule from the SCBA manufacturer. Typically a flow test is required on at least an annual basis.
|
The National Institute for Occupational Safety and Health (NIOSH) initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agencys recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim.
|
For further information, visit the program Web site at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
This page was last updated on 11/17/2010.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research