


Volunteer Fire Fighter Dies During Attempted Rescue of Utility Worker From a Confined Space -New York
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2010-31 Date Released: December 12, 2011
Executive Summary
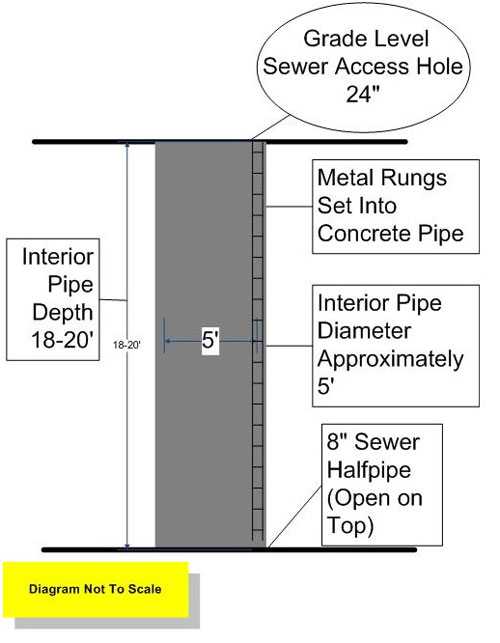
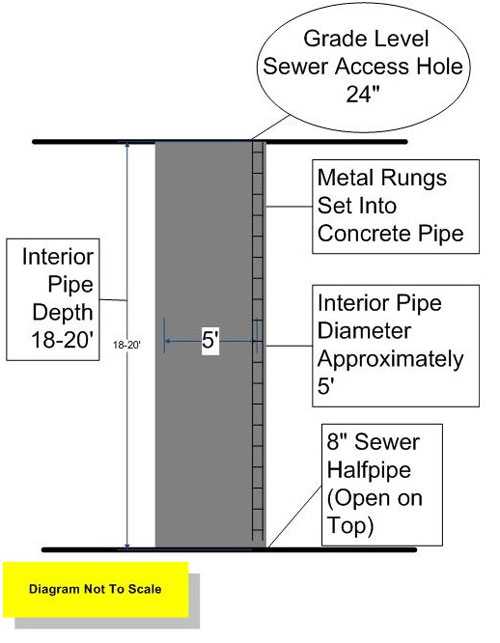
On September 6, 2010, a 51-year-old male volunteer fire fighter (victim) died after being overcome by low oxygen and sewer gases while climbing down into a sewer manhole in an attempt to rescue a village utility worker. The utility worker had entered the manhole to investigate a reported sewer problem and was overcome by low oxygen and sewer gases (see diagram 1). The incident occurred behind the fire station in an underground sewer line that ran under the fire station. The local utility company contacted the chief of the village's volunteer fire department and requested that a piece of fire apparatus be moved out of the station so they would not block it in while accessing a manhole. The fire chief responded to the station to move fire apparatus so it would not be blocked by the utility trucks. The victim and another fire fighter also arrived at the station to assist. A utility worker entered the manhole behind the station to clear a sewer backup and was overcome by a lack of oxygen and sewer gases and then fell unconscious inside the manhole. The victim then entered the manhole without any personal protective equipment to help the utility worker and was also overcome by the low oxygen level and sewer gases. The victim and the utility worker were later removed from the sewer manhole by fire department personnel and transported to a local hospital where they were pronounced dead. The medical examiner reported the cause of death as asphyxia due to low oxygen and exposure to sewer gases. Note: The death of the utility worker was investigated by the New York State Department of Health, Bureau of Occupational Health, Fatality Assessment and Control Evaluation (FACE) program. A link to the New York FACE report will be included in this report when completed. The New York State Department of Labor, Division of Safety and Health also conducted an investigation of this incident.
 |
|
Sewer Access Site |
Contributing Factors
- Unrecognized hazards involved with a confined space
- Lack of Standard Operating Procedures (SOP's) for confined space technical rescue operations
- In-effective incident management system for a confined space technical rescue operation.
Key Recommendations
- Ensure that fire fighters are properly trained and equipped to recognize the hazards of and participate in a confined space technical rescue operation
- Ensure that standard operating procedures regarding technical rescue capabilities are in place and a risk benefit analysis is performed to protect the safety of all responders
- Ensure that an effective incident management system is in place that supports technical rescue confined space operations
- Ensure that a safety officer properly trained in the technical rescue field being performed is on scene and integrated into the command structure.
 |
|
Diagram 1. Sewer pipe and access dimensions. |
Introduction
On September 6, 2010, a 51-year-old male volunteer fire fighter died after being overcome by low oxygen and sewer gases while climbing down into a sewer manhole in an attempt to rescue a village utility worker. On September 7, 2010, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On September 27- October 1, 2010, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program in Morgantown WV and an Industrial Hygienist from the NIOSH Health Hazard Evaluation Program located in the Division of Surveillance, Hazard Evaluations and Field Studies in Cincinnati Ohio, traveled to New York to investigate this incident. The NIOSH investigators conducted an opening meeting with the Fire Chief, assistant fire chief and the village administrator. The NIOSH investigators also met with representatives of the New York State Department of Labor, Public Employee Safety and Health Bureau (PESH), and the supervisor of the village public works crew involved in this incident. NIOSH investigators also spoke with the county deputy commissioner of emergency services. The NIOSH investigators visited the incident scene and conducted interviews with officers and fire fighters of the involved department who were present during the incident. The NIOSH investigators reviewed the fire department's standard operating procedures, the victim's training records, incident dispatch audio tapes, and photographed the incident scene.
Fire Department
The victim's department is a volunteer department and has 6 stations with 185 members that serve a population of approximately 12,000 residents within an area of about 4 square miles. The fire department responds to approximately 500 emergency incidents per year. The 6 stations house 4 engines, 2 ladders, 1 fireboat and 1 zodiac rescue boat. The department does not provide emergency medical services. The department is under the direction of the Chief Engineer (Fire Chief), 1st Assistant Chief, and 2nd Assistant Chief. Each of the Chiefs serves a term of 1 year and are elected by the membership. The fire department requires its members to provide medical clearance from their own doctor and also provides annual physicals for those members classified as interior structural fire fighters. The department issues 2 accountability tags to its members consisting of a photo ID on a colored tag with a green background for interior fire fighters and a red background for exterior fire fighters. These tags are kept on the member's turnout gear and helmet and collected on an incident scene by the incident commander.
Training and Experience
The victim had 33 years of service with the department. The victim had over 150 hours of documented training including classes in emergency control of hazmat incidents, fire fighting essentials, fire ground safety, driver training, pump operations, and equipment safety checks. The victim was considered an exterior fire fighter and according to department procedures, not permitted inside of an IDLH atmosphere.
The victim's department conducts in-house training and participates in joint training sessions with neighboring fire departments. Members also attend training provided by the state office of fire prevention and control. The victim's fire department requires members wishing to serve as an interior fire fighter to attain a minimum level of training of Fire Fighter 1 within 1 year of membership. Note: Fire Fighter 1 training met the criteria for National Fire Protection Association (NFPA) 10011, Standard for Fire Fighter Professional Qualifications, Fire Fighter I. The fire department then provides mask fit testing. Members that do not have medical clearance or Fire Fighter 1 training would be considered by the department an exterior fire fighter. Note: The department standard operating procedures (SOPs) describe two levels of authorized participation depending on the member's medical clearance and training. These are described as an interior fire fighters who possess at least Fire Fighter 1 training and has medical clearance and been mask fit tested within the past year and be medically certified as capable of handling interior duties, and exterior fire fighters who provide fire fighting support duties relegated to operations outside of a structure or incident not requiring respiratory protection such as SCBA. Exterior fire fighters are not permitted inside of an IDLH atmosphere. Any member who does not wish to be an interior fire fighter for any reason can declare themselves an exterior fire fighter.
The county department of emergency services offers scheduled fire fighter training (including technical rescue confined space training) throughout the year and that training is made available to all departments in the county through notices emailed to the Chiefs in the county and is also posted on their web site. The department involved in this incident has since met with the department of emergency services and scheduled fire fighter confined space awareness training.
Incident Timeline
The timeline for this incident is limited to the initial response of Fire Departments A and B with fire apparatus to a structure fire on June 17, 2011.
- 1552 Hours
Village public works notified of sewer back up at residence. Department of Public Works (DPW) workers bring in a vacuum truck and begin working in a number of locations to solve the sewer backup problem including an area with three manholes near the fire station (see photo 1). - Between 1552 and 1836 Hours
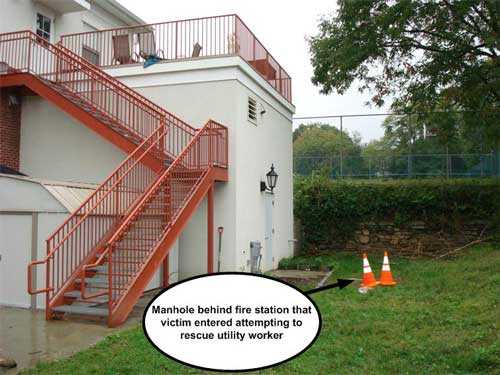
The DPW workers isolate the area of the backup to the firehouse and phone the Fire Chief to move a piece of fire apparatus. The Fire Chief arrives at the firehouse. The victim and another fire fighter also arrive at the firehouse to assist. Fire apparatus are moved and attempts to clear the clog are made with the vacuum truck in the manhole in front of the firehouse (see photo 1) and in the manhole inside the firehouse. The DPW workers and fire fighters then move to the manhole behind the firehouse (see photo 2) and clear away grass to access the manhole. The DPW workers then call for a smaller vacuum truck to respond to the scene due to the location preventing the use of the large vacuum truck. The DPW worker removes the manhole cover and grabs a shovel and enters the manhole. Soon after, fire fighters notice the DPW worker lying at the bottom of the pipe and believe he fell while descending. DPW supervisor asks the Chief to call for an ambulance. Note: there are no recorded times available for the events between 1552 and 1836 hours due to the events leading up to the Chief's phone call not being part of an emergency communications response. The description of these events is based upon witness interviews. - 1836 Hours
Chief of department phones 911 and requested an ambulance be dispatched to fire station for a man that has fallen into a manhole. - 1837 Hours
Village ambulance dispatched to respond to fire station for a man who has fallen in a manhole. - 1838 Hours
Village police and fire department dispatched to respond to a man who has fallen into a manhole behind fire station. - 1841 Hours
Chief requests neighboring police department technical rescue team for two people unconscious at the bottom of a 15' hole. - 1843 Hours
Village dispatch calls neighboring police department to request technical rescue team. - 1906 Hours
Technical rescue team from neighboring police department responds. - 1918 Hours
Technical rescue team arrives on scene. - 1919 Hours
The fire fighter and public works victim reported to be removed from manhole.
 |
|
Photo 1. Front of firehouse, sewer line ran underneath building. |
 |
|
Photo 2. Manhole behind fire station that victim entered |
Personal Protective Equipment
The victim was reported to be wearing civilian clothing with no PPE or SCBA. The DPW worker was not wearing any PPE or SCBA.
Weather Conditions
At the time of the incident (approximately 1637 hours), the weather was clear with an approximate temperature of 78°F. The relative humidity was 34% and the wind was SSW at 3 mph.2
Investigation
On September 6, 2010, a 51-year-old male volunteer fire fighter died after being overcome by low oxygen and sewer gases while climbing down into a sewer manhole attempting to rescue a village utility worker. The utility worker climbed down into the manhole to investigate a reported sewer problem and was overcome by low oxygen and sewer gases. The incident occurred behind the fire station in an underground sewer line that ran under the fire station.
The Fire Chief received a phone call from a department of public works (DPW) employee who told him that there was a sewer back up at the fire station and that the employee needed access to the fire station. The Fire Chief responded to the station to move a piece of fire apparatus out of the fire station so the apparatus would not be blocked by the utility trucks in the event of an emergency. The victim and another fire fighter learned of the sewer problem and also responded to the station to assist. Note: There were three sewer access manholes at the fire station, one in front of the apparatus bay, one inside the fire station on the apparatus floor (see photo 1),and one in the back of the fire station (see photo 2). The utility workers reportedly isolated the sewer problem to an area behind the fire station and located the manhole behind the fire station (see photo 2). A DPW supervisor reported that the public works employee opened the manhole, grabbed a shovel, and entered the manhole (Photo 2) while the supervisor was on the phone. The utility worker did not don any PPE or SCBA prior to entry. The victim and another fire fighter walked over to the manhole and saw the public works employee at the bottom of the hole and thought that the employee had fallen while descending the access ladder (see Diagram 1). The second fire fighter reportedly suggested to the DPW supervisor that he go in and get the downed utility worker and the DPW supervisor reportedly said no and told the fire fighters to get boots, rope and the gas meter from the fire truck. The Fire Chief saw the volunteer fire fighter (the victim) yelling to the employee in the manhole. The Fire Chief reported that the DPW supervisor told him that the employee had fallen into the manhole and asked the Chief to call an ambulance. The Fire Chief called the village dispatcher and requested an ambulance and fire department response for a man who has fallen into a manhole. The second fire fighter brought the fire truck closer to the manhole and brought the rope and a meter to the DPW supervisor. The victim went to his pickup truck and put his boots on, then returned and entered the manhole before the gas meter was ready to be used. The victim entered the manhole, without PPE or SCBA, and made it half way down the access ladder and then fell to the bottom. The Fire Chief did not order or direct the victim to enter the manhole and was not aware of the victim entering the manhole. The DPW supervisor then told the Chief that a second man had fallen into the manhole and asked for a second ambulance. The Chief requested a second ambulance and also asked for the technical rescue team from a neighboring police department. The Chief told the DPW supervisor that no one else should go into the manhole. Both victims were unresponsive at the bottom of the manhole pipe. A gas detection meter was tied to a rope and lowered into the hole. Witness reports stated that the meter alarmed, one witness stating that the meter read 11.4% oxygen and another witness stating that the meter read 14% oxygen. Two engines and one ladder truck from the department involved were on scene and started to set up for a rescue attempt. Note: The sewer manhole opening was only 24 inches in diameter and opened up to a 5 foot diameter once through the opening. The depth to the bottom of the manhole was reported as 18 feet. A tripod was set up over the manhole and a fan put in service blowing fresh air into the manhole. One fire fighter donned an SCBA face piece while the SCBA cylinder and back pack were tied off and lowered with the fire fighter while he entered the manhole with a separate rope and descended down the vertical manhole pipe. An oxygen cylinder and mask for the victim was lowered in with the fire fighter. The fire fighter placed the oxygen mask on the victim and tied a rope on the victim and other fire fighters hoisted him out of the sewer pipe. The fire fighter assisted with the removal of the victim up the pipe and then exited through the same manhole. Fire fighters on the surface then started cardio pulmonary resuscitation (CPR) and emergency medical care to the victim and he was transported to a local hospital where he was pronounced dead. After the first victim was removed, another fire fighter donned an SCBA face piece, tied off his SCBA backpack and descended into the hole in the same manner as the first with other fire fighters lowering the SCBA backpack as he descended. When the fire fighter reached the public works victim, he tied the victim off with a separate rope to the surface and fire fighters on the surface hoisted him up while the fire fighter assisted from below. The DPW victim was then given CPR and emergency medical care and also transported to a local hospital where he was pronounced dead. The technical rescue team from a neighboring police department arrived after both victims had been removed. The technical rescue team members were a combination of police officers and fire fighters trained in confined space rescue at the technician level from a neighboring city. The technical rescue team reported that they established a unified command with the local fire department and ensured that the scene was secured and established a safe zone and ignition sources close to the manhole were removed. The team also asked the fire department to staff two hose lines for protection. The neighboring city also provided utility crews to address the blocked clogged sewer line.
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatalities:
- Unrecognized hazards involved with a confined space
- Lack of Standard Operating Procedures (SOP's) for confined space technical rescue operations
- In-effective incident management system for a confined space technical rescue operation.
Cause of Death
According to the county coroner, the cause of death was asphyxia due to low oxygen and exposure to sewer gases.
 |
|
Diagram 1. Sewer pipe and access dimensions. |
Recommendations
Recommendation #1: Fire departments should ensure that fire fighters are properly trained and equipped to recognize the hazards of and participate in a confined space technical rescue incident.
Discussion: Fire departments should provide confined space awareness training as a minimum requirement for all fire fighters and more advanced confined space training to those personnel who might be called on to perform confined space rescue work (see Photo 3, an example of a confined space sewer manhole training prop). According to NFPA 1670, the minimum training for an organization shall be the awareness level. Organizations expected to perform at a higher operational level shall be trained to that higher level. The authority having jurisdiction shall provide for the continuing education necessary to maintain all requirements of the organizations identified level of capability. 3
Fire departments need to ensure that their employees recognize the hazards involved in a confined space incident. A confined space refers to a space which by design has limited openings for entry and exit, unfavorable natural ventilation which could contain or produce dangerous air contaminants or oxygen deficiency, and which is not intended for continuous employee occupancy. Confined spaces include but are not limited to storage tanks, compartments of ships, process vessels, pits, silos, vats, degreasers, reaction vessels, boilers, ventilation and exhaust ducts, sewers, tunnels, underground utility vaults, and pipelines. According to data collected by the U.S. Department of Labor (USDOL), Bureau of Labor Statistics (BLS) Census of Fatal Occupational Injuries (CFOI) program, fatal injuries in confined spaces fluctuated from a low of 81 in 1998 to a high of 100 in 2000 during the five year period, from 1995 to 2000, averaging 92 fatalities per year.4
OSHA defines a “permit-required” confined space as:
- Is large enough for an employee to enter fully and perform assigned work;
- Is not designed for continuous occupancy by the employee; and
- has a limited or restricted means of entry or exit.
These spaces may include underground vaults, tanks, storage bins, pits and diked areas, vessels, silos and other similar areas.
By definition, a "permit- required" confined space has one or more of these characteristics:
- Contains or has the potential to contain a hazardous atmosphere;
- Contains a material with the potential to engulf someone who enters the space;
- Has an internal configuration that might cause an entrant to be trapped or asphyxiated by inwardly converging walls or by a floor that slopes downward and tapers to a smaller cross section;
- Contains any other recognized serious safety or health hazards. 5
Hazards associated with confined spaces have been well documented and employees who are required to work in confined spaces are mandated by the Occupational Safety and Health Administration (OSHA) to be trained in confined space hazards and safe work practices. OSHA 29 CFR 1910.1466 regulates permit required confined space entry and procedures and OSHA 1910.1347 regulates respiratory protection. Public service employees (fire fighters, police officers, rescue workers) that respond to emergency situations involving confined spaces should be trained in specific confined space hazards and rescue procedures.8
The following information and recommendations for employees who work in confined spaces is taken from the NIOSH ALERT, Request for Assistance in Preventing Occupational Fatalities in Confined Spaces.9 Specific recommendations for public service employees who might be called upon to rescue workers in a confined space are listed after the NIOSH Alert information.
Oxygen deficient and hazardous gas atmospheres are a common hazard to utility and rescue workers who enter a confined space. Confined spaces may be encountered in virtually any occupation; therefore, their recognition is the first step in preventing fatalities. Since deaths in confined spaces often occur because the atmosphere is oxygen deficient or toxic, confined spaces should be tested prior to entry and continually monitored. More than 60% of confined space fatalities occur among would-be rescuers; therefore, a well-designed and properly executed rescue plan is a must. NIOSH investigations indicate that workers usually do not RECOGNIZE that they are working in a confined space and that they may encounter unforeseen hazards. TESTING and EVALUATION of the atmosphere are typically not initiated prior to entry and MONITORING is not performed during the confined space work procedures. RESCUE is seldom planned and usually consists of spontaneous reaction in an emergency situation.9
Based on the information derived from these NIOSH fatality investigations,10 NIOSH concludes that these fatalities occurred as a result of encountering one or more of the following potential hazards:
- lack of natural ventilation,
- oxygen deficient atmosphere,
- flammable/explosive atmosphere,
- unexpected release of hazardous energy,
- limited entry and exit,
- dangerous concentrations of air contaminants,
- physical barriers or limitations to movement, or
- instability of stored product.9
Specific recommendations for public service employees.
Public service employees (fire fighters, police officers, rescue workers) that respond to emergency situations involving confined spaces should be trained in specific confined space hazards and rescue procedures.8 NFPA 1670 Operations and Training for Technical Search and Rescue Incidents,3 provides training recommendations for fire departments that might be called upon to perform technical rescue in confined space incidents. The standard identifies and establishes levels of functional capability for conducting operations at technical rescue incidents while minimizing threats to rescuers. The three levels of training are:
- Awareness level. This level represents the minimum capability of organizations that provide response to technical search and rescue incidents.
- Operations level. This level represents the capability of organizations to respond to technical search and rescue incidents and to identify hazards, use equipment, and apply limited techniques specified in this standard to support and participate in technical search and rescue incidents.
- Technician level. This level represents the capability of organizations to respond to technical search and rescue incidents and to identify hazards, use equipment, and apply advanced techniques specified in this standard necessary to coordinate, perform, and supervise technical search and rescue incidents.3
Fire Departments should be trained at a minimum to the awareness level.3 NFPA 1006 Standard for Technical Rescuer Professional Qualifications,11 provides information on the established general job performance requirements for a rescue technician as well as specific job performance requirements. These performance requirements include rope rescue, surface water rescue, vehicle and machinery rescue, confined space rescue, structural collapse rescue, and trench rescue.
In this incident, the victim and the public utility supervisor likely thought that the public utility worker had fallen after he entered the sewer and became unconscious from the fall. The victim possibly did not recognize the hazards of a confined space sewer such as low oxygen and a toxic atmosphere and made the decision to enter the manhole without any personal protective equipment or respiratory protection. If the victim had received the minimum awareness level confined space training, he possibly could have recognized the hazards and performed non-entry rescue operation procedures such as recognizing the need for confined space search and rescue, initiating contact and establishing communications with the victims if possible, recognizing and identifying the hazards associated with non-entry confined space emergencies, perform a non-entry retrieval, implementing the emergency response system for confined space emergencies, implementing site control and scene management.
Recommendation #2: Fire departments should ensure that standard operating procedures regarding technical rescue capabilities are in place and a risk benefit analysis is performed to protect the safety of all responders.
Discussion: It is important that fire departments establish SOP's that guide emergency responders to recognize the presence of a confined space hazards and respond accordingly and/or request the appropriate assistance of a qualified technical rescue confined space team. Some fire departments may not have the resources to support a confined space rescue team (a combination of individuals trained, equipped, and available to respond to confined space emergencies).3 Many communities rely on mutual aid or a combination of jurisdictional resources to provide response capabilities to complex technical rescue incidents such as high angle, hazardous materials response, trench or confined space, or other technical rescuer professional level operations. A single community might not possess sufficient resources to effectively and safely provide a response level that would satisfy all the components of a safe, efficient, and effective emergency incident response. A program that measures the risk versus benefit of a particular emergency operation is crucial to the safety of all emergency responders. A risk-benefit analysis must be performed on two levels: executive and on the scene. At the executive or strategic level, municipal and fire department leaders should identify their mission capabilities or plan for expanding their current capabilities through long-term funding, training, and continued support. Emergency incident risk-benefit analysis is performed on the scene, by the first arriving responders, and continued throughout the incident by the command structure. Fire department executives should perform a risk-benefit analysis and strategically plan for an emergency response that ensures the safety of all responders. For the more infrequent number of incidents requiring technical rescuer professional level operations, preplanning and strategic level risk-benefit analysis can identify the level of response that can be safely performed and alternatives such as mutual aid or multi-jurisdictional, multi-agency capabilities that can be utilized.12 NFPA 1250 Recommended Practice in Fire and Emergency Services Organization Risk Management, 2010 Edition13 provides recommendations to identify risk and develop risk analysis for fire and emergency services organizations. A risk assessment can identify existing and potential risks through and evaluation of operational activities, exposure situations and prior loss experience. A risk analysis should employ techniques applicable to the type of loss exposure or the hazard involved.
In this incident, the fire department was contacted by the Department of Public Works to move apparatus from the fire station so they would not be blocked in by the utility trucks in case the fire department had an emergency call. The incident escalated from assisting the public utility crews by moving apparatus to witnessing one of the workers become unconscious and fall inside the sewer. The victim and others apparently did not recognize the hazards associated with a confined space sewer such as the toxic atmosphere and low oxygen and attempted a rescue of the public utility worker. The victim was overcome by toxic sewer gases and low oxygen, became unconscious, and fell to the bottom of the sewer. The Chief called for a technical rescue response from a neighboring police department and while they were responding other fire department personnel on the scene used ropes and SCBA lowered separately into the sewer and removed the two victims. Fire departments should have clear SOP's defining procedures that should be taken by response personnel when dealing with technical rescue incidents and also ensure that a risk-benefit analysis has been performed.
Recommendation #3: Fire departments should ensure that an effective incident management system is in place that supports technical rescue confined space operations.
Discussion: At all technical search and rescue incidents, the organization shall provide supervisors who possess skills and knowledge commensurate with the operational level identified in NFPA 1670 chapter 4.1.4.3 In the initial stages of a technical rescue, it is not uncommon for the Incident Commander to be playing catch-up implementing span of control and unity of command measures while expanding the command structure until enough management resources arrive on scene. An effective Incident Management System has two components: (1) the roles and responsibilities to be assumed by responders and (2) standard operating procedures to be used in the management and direction of emergency incidents and other functions.14 The incident management system should be tailored to the department's resources and the likely types of response needed in the jurisdiction. Personnel should be thoroughly trained in and understand the incident management system and how they are to operate within the incident action plan. In his book, Fire Department Safety Officer 2nd ed.,15 Chief Dodson defines freelancing as "a failure to work within the framework of an incident action plan. Fire fighters have been killed and seriously injured while engaged in a freelance operation, that is, an operation or task being performed unknown to the incident commander or other working crews." Responders should understand that the check-in process allows incident command to maintain accountability and to ensure the safety of all responders.
In this incident, the Chief and other fire fighters responded to the fire station to assist the Department of Public Works in a non-emergency event. The incident escalated to an emergency incident that they believed was a medical event with the public utility worker and then further escalated to a confined space rescue event after the victim entered the manhole. The Fire Chief requested the assistance of a technical rescue team from a neighboring police department after the victim had entered the sewer and was overcome. The Chief did not order or direct the victim to enter the manhole and was not aware of the victim entering the manhole. While waiting for the technical rescue team to arrive, a rescue mission was conducted by fire fighters entering the sewer using SCBA (Note: Fire fighters climbed into the sewer through the 24" manhole with their face pieces on and the SCBA lowered on a rope separate from the fire fighters. They performed this one at a time and were able to secure a rope on the victim and the utility worker and crews hoisted the victims out of the sewer). An effective incident management system was not in place to recognize the hazards or prevent the victim or other fire fighters from entering the sewer without proper procedures in place. The responding technical rescue team had the proper training (technician level), skills and equipment to extricate the victim and the utility worker from the sewer. Although the two fire fighters who entered the sewer and others who assisted on the surface performed a heroic and brave operation to extricate the victim and the utility worker, the operation required a higher level of training, more personnel and equipment, and an effective incident management system to adequately ensure the safety of the responders. Rescuers cannot perform a safe and effective rescue when they become victims, as well.
Recommendation #4: Fire departments should ensure that a safety officer properly trained in the technical rescue field being performed is on scene and integrated into the command structure.
Discussion: At technical search and rescue training exercises and in actual operations, the incident commander shall assign a safety officer with the specific knowledge and responsibility for the identification, evaluation and where possible, correction of hazardous conditions and unsafe practices.3 Safety officers assigned to special operations incidents need to have the expertise in the specific technical rescue field to effectively evaluate hazards and provide direction with respect to the safety of all personnel. A qualified fireground safety officer might not possess the expertise in confined space technical rescue and, therefore, might not recognize or understand capabilities of the team members, limitations and hazards to rescue workers, the need for specialized equipment (i.e. haul systems [to remove victim], hazardous atmosphere monitors, supplied air breathing apparatus vs. self contained breathing apparatus etc.) problems with equipment, or performance issues of personnel [i.e. under trained for the mission]. NFPA 1521 Standard for Fire Department Safety Officer, 2008 edition,16 notes, in cases where the designated incident safety officer does not possess the technician-level training, appointing a technician level trained assistant or technical specialist with the necessary training will help satisfy the safety needs of the technician-level members. A fire department safety officer properly trained in the technical rescue field being performed can also help prevent a fire fighter from attempting a skill beyond their level of training.
In this incident, the event escalated from a non-emergency event to a suspected emergency medical event and then to a confined space rescue event. A fire department response was eventually initiated that included a request for a technical rescue team from a neighboring police department. A fire department safety officer qualified in confined space rescue could have provided the incident commander with information that could have minimized the threat to other emergency personnel assisting in the operation.
 |
| Photo 3. Example of a sewer access training prop for confined space evolutions. (NIOSH photo) |
References
- NFPA [2008]. NFPA 1001: Standard for Firefighter Professional Qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- Weather Underground [2010]. Weather history for New York, September 6, 2010. http://classic.wunderground.com/weatherstation/WXDailyHistory.asp?ID=KNYTARRY3&month=9&day=6&year=2010 Date Accessed: March 1, 2011.
- NFPA [2009]. NFPA 1670: Standard on Operations and Training for Technical Search and Rescue Incidents. 2009 ed. Quincy, MA: National Fire Protection Association.
- Centers for Disease Control, NIOSH Confined Spaces, http://www.cdc.gov/niosh/topics/confinedspace/. Date accessed 4/29/2011.
- OSHA 3138-01R 2004 Permit-Required Confined Spaces, https://www.osha.gov/Publications/osha3138.pdf Date accessed 4/29/2011.
- Occupational Safety and Health Standards 1910.146, General Environmental Controls, Permit- Required Confined Spaces, https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=standards&p_id=9797 Date assessed 4/29/2011.
- Occupational Safety and Health Standards 1910.134, Personal Protective Equipment, Respiratory Protection, https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_id=12716&p_table=standards Date accessed 4/29/2011.
- NIOSH FACE Report FACE 87-06: Worker Deaths in Confined Spaces, Two Dead, Five Injured in Confined Space Incident in Oregon, http://www.cdc.gov/niosh/face/in-house/full8706.html Date accessed 4/29/2011.
- NIOSH ALERT: January 1986 DHHS (NIOSH) Publication No. 86-110. Request for Assistance in Preventing Occupational Fatalities in Confined Spaces.
- NIOSH: January 19994 DHHS (NIOSH) Publication No. 94-103. Worker Deaths in Confined Spaces, A Summary of NIOSH Surveillance and Investigative Findings.
- NFPA [2008]. NFPA 1006 Standard for Technical Rescuer Professional Qualifications. Quincy, MA: National Fire Protection Association.
- NIOSH [2008]. Career fire fighter dies while diving for a civilian drowning victim - Rhode Island Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, Fatality Assessment and Control Evaluation (FACE) Report F2008-32 http://www.cdc.gov/niosh/fire/reports/face200832.html. Date accessed: February 10, 2011.
- NFPA [2010]. NFPA 1250 Recommended Practice in Fire and Emergency Services Organization Risk Management. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
- Dodson D [2007]. Fire department incident safety officer. 2nd ed. New York: Delmar Publishers.
- NFPA [2008]. NFPA 1521 Standard for fire department safety officer. Quincy, MA: National Fire Protection Association.
Investigator Information
This incident was investigated by Stephen Miles and Virginia Lutz, Safety and Occupational Health Specialists with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV, and Scott Brueck, Industrial Hygienist from the NIOSH Health Hazard Evaluations Program located in the Division of Surveillance, Hazard Evaluation and Field Studies, in Cincinnati Ohio. An expert technical review was provided by Brian P. Kazmierzak, EFO, MABAS Division 201 Tactical Rescue Team Task Force Leader. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Additional Information
- IAFF Confined Space Training Program, http://www.iaff.org/et/hw/PDF/Course_Description_CSR.pdf
- IAFC asks for stand-down to pursue confined space training, http://www.fireengineering.com/articles/print/volume-163/issue-8/departments/news-in_brief/iafc-asks-for-stand-down-to-pursue-confined-space-training.html
- IAFC Technical Rescue Resources, Department Preparations, http://www.iafc.org/Operations/content.cfm?ItemNumber=1303
- IAFC Suggested Technical Rescue Response Preparation Activities, http://www.iafc.org/files/safety_TechRescueRecommendedActs_SHS.pdf
- American Society of Safety Engineers, http://www.asse.org/broadcasts/confined-spaces-techbrief9-24-09.html
- United States department of Labor, Occupational Health and Safety Administration, Confined Space Standard 1910-146, https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=standards&p_id=9797.
- United States department of Labor Safety and Health Topics, Confined Spaces, https://www.osha.gov/SLTC/confinedspaces/index.html.
- New York Department of Labor Public Employee Safety and Health Bureau (PESH) report, http://tarrytown.patch.com/articles/state-releases-reports-on-manhole-deaths#pdf-4003195 http://tarrytown.patch.com/articles/state-releases-reports-on-manhole-deaths#pdf-4003196. (Links no longer available 5/28/2013)
- CDC/NIOSH Workplace Safety and Health Topics, http://www.cdc.gov/niosh/topics/confinedspace/
- A summary of NIOSH Surveillance and Investigative Findings, http://www.cdc.gov/niosh/docs/94-103/.
- NIOSH Fatality Assessment and Control Evaluation (FACE) Program, http://wwwn.cdc.gov/NIOSH-FACE/Default.cshtml?state=ALL&Incident_Year=ALL&Category2=0004⊂mit=Submit (Link Updated 5/13/2015)
- NIOSH State based Fatality Assessment and Control Evaluation (FACE) Program, http://wwwn.cdc.gov/NIOSH-FACE/Default.cshtml?Category=0004&Category2=ALL⊂mit=Submit. (Link Updated 5/13/2015)
- Occupational Health and Safety, What Can go Wrong in Confined Spaces? Part 1 http://ohsonline.com/articles/2011/02/01/what-can-go-wrong-in-confined-space-rescues.aspx?sc_lang=en
- Occupational Health and Safety, What Can go Wrong in Confined Spaces? Part 2 http://ohsonline.com/articles/2011/08/01/what-can-go-wrong.aspx
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH "Fire Fighter Fatality Investigation and Prevention Program" which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
|
For further information, visit the program Web site at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
This page was last updated on 01/12/2012.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research