


A Career Lieutenant and Fire Fighter/Paramedic Die in a Hillside Residential House Fire – California
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2011-13 Date Released: March 1, 2012
Executive Summary
On June 02, 2011, a 48 year-old career lieutenant and a 53 year-old fire fighter/paramedic died in a multi-level residential structure fire while searching for the seat of the fire. Note: The residential structure where the fatalities occurred was built on a significantly sloped hillside common throughout the city. The fire floor was one floor below street level. Six companies and three command chiefs were dispatched to a report of an electrical fire at a residential home. When Engine 26, staffed with a lieutenant, fire fighter/paramedic (the victims), and driver arrived at approximately 1048 hours, they noticed light smoke showing as they made entry through the front door, side A, street level, of the building. Minutes later, the incident commander (IC) tried contacting them over the radio, but received no response. A battalion chief (BC) assigned to "the fire attack group" followed the hoseline through the door and spoke to the victims on the street level floor. The lieutenant stated to the BC that the fire must be a floor below them. The BC stated they would attack the fire from the side B of the structure and exited the front door. The victims did not follow. A few minutes later the IC again tried to contact Engine 26 via radio with no response.

The side C of the fire structure - the balcony
is the fire floor which is below grade from street level.
(Photo courtesy of Fire Department)
The crew from Engine 24, assigned to back up Engine 26, and a split crew from Rescue 1 tried to make entry through the door in the garage but could not advance due to the heat. The BC went to the side B door, located one floor below street level, and forced the door with the Engine 11 crew on the hoseline. They immediately felt a blast of heat from the fully involved basement area. The Rescue 1 crew backed out of the garage and re-entered on side B after the Engine 11 crew knocked down the large room and contents fire. At about the same time, the Engine 24 crew also backed out of the garage and followed the Engine 26 crew's hoseline through the front door. In zero visibility conditions, separate members of the Engine 24 crew independently found a downed member of the Engine 26 crew. The Incident Commander was alerted of a downed fire fighter but, did not initially realize, until moments later that it was actually two downed fire fighters. Both victims were removed from the structure and immediate medical treatment was provided. The victims were transported to the local medical center where the lieutenant was pronounced dead and the fire fighter/paramedic died two days later.
Contributing Factors
- Construction features of the house built into a steep sloping hillside
- Natural and operational horizontal ventilation
- Ineffective size-up
- Fire fighters operating above the fire
- Ineffective fire command communications and progress reporting
- Lack of a personnel accountability system.
Key Recommendations
- Ensure that standard operating guidelines (SOGs) for coordinated operations are developed and implemented for hillside structures
- Ensure that an adequate size-up of the structure is conducted prior to crews making entry
- Ensure staffing levels are maintained
- Ensure that a personnel accountability system is established early and utilized at all incidents
- Ensure that fireground operations are coordinated with consideration given to the effect horizontal ventilation has on the air flow, smoke, and heat flow through the structure
- Ensure that the Incident Commander is provided a chief’s aide at all structure fires
- Ensure that an incident safety officer is assigned to all working structure fires
- Ensure that fire fighters are trained in Mayday procedures and survival techniques
Additionally,
- Continue research and efforts to improve radio system capabilities
- Adopt and enforce regulations for automatic fire sprinkler protection in new buildings and renovated structures.
Introduction
On June 02, 2011, a 48 year-old career lieutenant (victim #1) and a 53 year-old fire fighter/paramedic (victim #2) died in a residential house fire while searching for the seat of the fire. On June 06, 2011, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On June 12-17, 2011, a general engineer and an investigator from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to California to investigate this incident. The NIOSH investigators conducted an opening meeting with fire department officials. During the interview process NIOSH investigators met with a representative from the International Association of Fire Fighters local union. The NIOSH investigators visited the incident scene and conducted interviews with officers and fire fighters who were at the incident. The NIOSH investigators reviewed the fire department's standard operating guidelines, officers' and fire fighters' training records, dispatch audio tapes, and the city and county medical examiner's autopsy reports. NIOSH investigators also reviewed the Arson Investigation Report, dated November 6, 2011, once it was released.
Fire Department
This career fire department has 44 stations with 1,400 uniformed members serving a population of approximately 1,400,000 within an area of about 47.5 square miles. The fire department responds to approximately 110,000 emergency calls annually. Eighty percent of those emergency calls are medical calls. The fire department operates 9 battalions in 2 divisions. The fire department currently has 43 engine companies, 19 truck companies, 2 heavy rescue companies, 2 fire boats, 4 wildland/brush trucks, 45 EMS units, and a mobile mask service unit. Specialty units consist of swift water/surf rescue, cliff rescue, hazardous materials, and urban search and rescue. The fire department’s airport division staffs 3 fire stations with 95 personnel, 4 aircraft rescue and fire fighting vehicles, 2 engine companies, 1 truck company, 2 advanced life support medic units, and 1 command vehicle. All department members work a 24-hour duty shift with 48 hours off, and a 48.7 hour work week. Fire department apparatus are maintained by the city’s fleet Maintenance Division with annual testing of fire apparatus and ambulances conducted by qualified vendors. The fire department has written policies and procedures which are available to all department members within their stations. Policies and procedures on incident command structure, personnel accountability system, and truck operations were in place at the time of the incident.
Training and Experience
The state requires all career fire fighters to complete training equivalent to the National Fire Protection Association (NFPA) 1001, Standard for Fire Fighter Professional Qualifications, Fire Fighter I and Fire Fighter II.1 The fire department provides up to 17 months of recruit training to certify fire fighters to NFPA 1001, and a one year probationary period of supervised training for fire fighter certification. Additional training during the probationary period focuses on equipment and operations. Table 1 lists the training and experience of the primary fire fighters involved in the incident.
Table 1. Training and Experience of Key Personnel
Fire Fighter |
Training Courses |
Years experience |
|---|---|---|
Victim #1 |
Fire Fighter I and II, Hazardous Material Operations, Emergency Response to Terrorism Basic Concepts, Confined Space, Trench Operations, Wildland/Urban Interface, Rapid Intervention Crew Training, Live Fire Training, and various administrative and technical courses. |
21 |
Victim #2 |
Fire Fighter I and II, Live Fire Training, Rapid Intervention Training, Numerous Paramedic courses, and various administrative and technical courses. |
14 |
Lieutenant #1 |
Fire Fighter I and II, Emergency Response to Terrorism Basic Concepts, Live Fire Training, Hazardous Materials/Confined Space, H20 (Lieutenant) Academy, numerous Wildland courses, and various administrative and technical courses. |
7 |
Lieutenant #2 |
Fire Fighter I and II, Hazardous Material Operations, Emergency Response to Terrorism Basic Concepts, Live Fire Training, National Incident Management System (NIMS) IS-700, Trench Safety, Truss Systems, Firefighter Self Survival, (Lieutenant) Academy and various administrative and technical courses. |
18 |
Captain |
Fire Fighter I and II, Hazardous Material Operations, Emergency Response to Terrorism Basic Concepts, Rapid Intervention Crew courses, Rescue Systems, Truss Systems, Trench Safety, Firefighter Self Survival, Multi-Casualty Management, Wildland/Urban Interface, Live Fire Training, and various administrative and technical courses.
|
22 |
Fire Fighter |
Training Courses |
Years experience |
Battalion Chief 6 |
Fire Fighter I and II, Hazardous Material Operations, Weapons of Mass Destruction Incident Management Unified Command, NIMS IS-700, Disaster Preparedness, Rapid Intervention Crew courses, Rescue Systems, Truss Systems, Multi-Casualty Management, High Rise Hose and rescue, Wildland/Urban Interface, Live Fire Training, and various administrative and technical courses. |
19 |
Battalion Chief 9 Note: A Captain awaiting promotion to BC |
Fire Fighter I and II, Fire Officer Certified, Hazardous Material Operations and Certification, Weapons of Mass Destruction Incident Management Unified Command, NIMS IS-700, NIMS Train the Trainer, numerous Terrorism courses, Disaster Preparedness, Rapid Intervention Crew courses, Confined Space Training, Trench Safety, Multi-Casualty Management, High Rise Hose and rescue, Wildland/Urban Interface, Live Fire Training, and various administrative and technical courses. |
20 |
Division Chief Note: Acting District Chief for 21 months and was promoted on 6/14/11 |
Fire Fighter I and II, Hazardous Material Operations, Weapons of Mass Destruction Incident Management Unified Command, NIMS IS-700, Advanced Incident Command Structure (ICS-400), Safety Officer, Chief Officer Certified, Strike Team Leader, Standardized Emergency Management System Instructor, Operational Section Chief, Plans Section Chief, numerous Terrorism courses, Disaster Preparedness, Rapid Intervention Crew courses, Trench Safety, Truss Systems, Multi-Casualty Management, Wildland/Urban Interface, numerous Wildland courses, Live Fire Training, Firefighter Self Survival, and various administrative and technical courses. |
29 |
Structure
The incident involved a four-story residential structure that was completed in 1976 (see Diagrams #1, #2, and #3). The structure was built on a hillside with a significant slope and has two stories above the street level and two stories below the street level. The top two stories provided 1,468 square feet of living space. The first floor (street level) contained 3 bedrooms, 2 bathrooms, and a 2 car garage. The second floor contained a living room, dining room, kitchen, family room, and a deck over the garage. A laundry area was located on a large landing on the stairs between the first floor and basement (see Diagram #4 and #5). The basement (first level below the street) contained a finished living area with a large utilities area. The basement was accessible from an exterior door on side B of the structure and an interior set of stairs. In addition, the basement had a balcony on side C (see Diagram #6). The sub-basement (second level below grade) contained a living area that was only accessible by an exterior door on side B and had no windows (see Diagram #7). The residential structure had a flat roof that consisted of a bitumen membrane roof. The exterior was primarily stucco with large windows on the top 3 stories of side C of the structure. Side D of the structure shared a common fire wall with another residential structure. This large multi-level structure had smoke alarms but no residential sprinkler system/automatic fire suppression. Note: The National Institute for Standards and Technology (NIST) will be doing a fire model on this incident which will be released in the future.

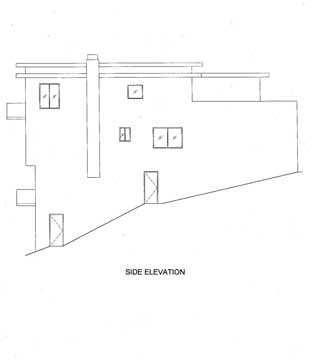
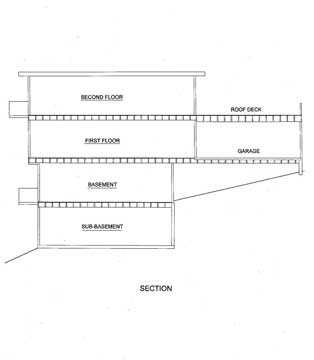
Diagram #1(left): Front (side A) and Rear (side C) of Fire Structure
Diagram #2(center): Side B of Fire Structure
Diagram #3 (right): Floor Levels and Grade
(Courtesy of Fire Department)
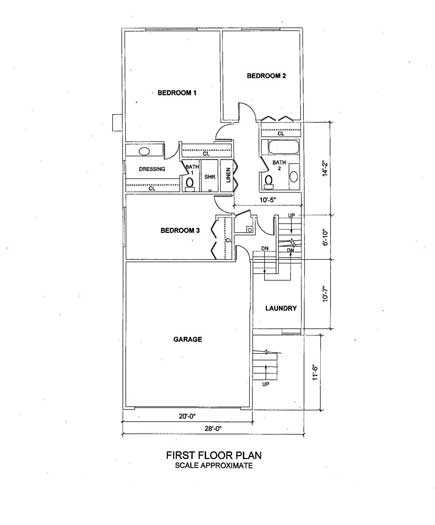
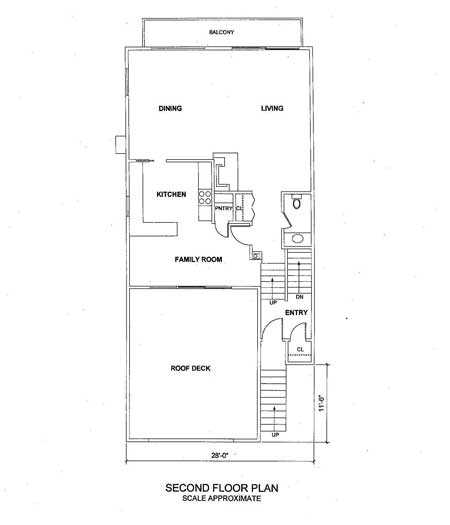
Diagram #4 (left): First Floor Layout (Street Level)
Diagram #5 (right): Second Floor Layout (Top Floor)
(Courtesy of Fire Department)
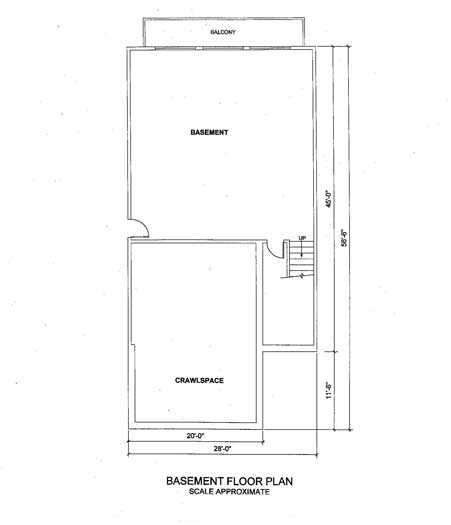
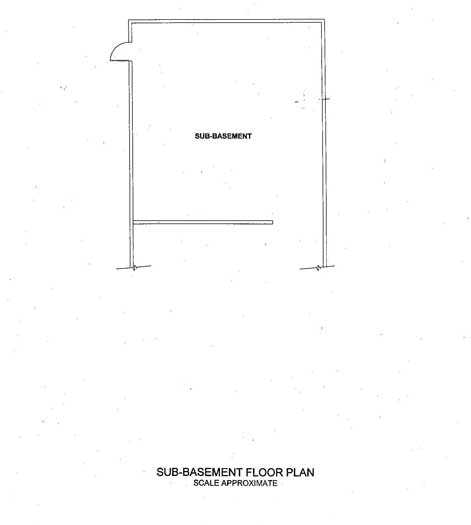
Diagram #6 (left): Basement Floor Layout (Below Grade; Fire Floor
Diagram #7 (right): Sub-Basement Floor Layout
(Courtesy of Fire Department)
Equipment and Personnel
The fire department dispatched three engines, two ladder trucks, a heavy rescue squad, three battalion chiefs, and a medic unit on the first alarm. Table 2 identifies the apparatus and staff dispatched on the first alarm, along with their approximate dispatch and arrival times on-scene (rounded to the nearest minute).
Table 2. First Alarm Equipment and Personnel Dispatched
Resource Designation |
Staffing |
Dispatched |
On-Scene (rounded to minute) |
|---|---|---|---|
Engine 26 (E26) |
Lieutenant (Victim #1) |
1045 hrs |
1048 hrs |
Engine 11 (E11) |
Lieutenant |
1045 hrs |
1052 hrs |
Engine 24 (E24) |
Lieutenant |
1045 hrs |
1051 hrs |
Truck 11 (T11) |
Captain |
1045 hrs |
1055 hrs |
Truck 15 (T15) |
Captain |
1045 hrs |
1056 hrs |
Battalion Chief 6 (BC6) Shift Relief BC |
Battalion Chief |
1045 hrs |
1052 hrs |
Battalion Chief 9 (BC9) |
Battalion Chief |
1045 hrs |
1053 hrs |
Battalion Chief 10 (BC10) Initially cancelled by DC3 then recalled |
Battalion Chief |
1045 hrs Redispatched 1155 hrs |
1246 hrs |
Resource Designation |
Staffing |
Dispatched |
On-Scene (rounded to minute) |
Rescue Squad 1 (RS1) |
Captain |
1045 hrs |
1054 hrs |
Medic 74 |
Paramedic |
1045 hrs |
1052 hrs |
Division Chief 3 (DC3) |
Division Chief |
1047 hrs |
1056 hrs |
Engine 32 (E32) |
Lieutenant |
1045 hrs |
1058 hrs |
Timeline
An approximate timeline summarizing the sentinel events of the incident is listed below. The times are approximate and were obtained by studying available dispatch records, photos, run sheets, witness statements, and fire department records. The times are rounded to the nearest minute. The timeline is not intended, nor should it be used, as a formal record of events.
- 1045 Hours
Dispatch for curtain fire due to an electrical short at a residential structure. E26, E11, E24, T11, T15, BC6, BC9, BC10 (cancelled by DC3, then DC3 self-dispatched), RS1, M74, and A16 assigned. - 1048 Hours
E26 arrives on scene and reports 3 story wood frame house and light smoke; E26 making entry at front door with 1 ¾" hoseline. - 1051 Hours
E24 on scene. - 1052 Hours
E11, BC6, and M74 on scene. The IC (BC6) tries to contact E26 via radio with no response. - 1053 Hours
BC9 on scene and assigned fire attack group. - 1054 Hours
RS1 on scene; BC9 follows E26 hoseline in front door; has a face to face discussion with victims on the first floor (street level); Victim#1 states fire is below them; BC9 tells victims, "We'll attack fire from side B"; the E24 crew checks for access through the garage and thinks they hear SCBA bottles hitting the floor inside the door to the foyer. - 1055 Hours
T11 on scene. - 1056 Hours
T15, DC3, and E32 on scene; DC3 assumes command. E32 initial rapid intervention crew (RIC); T15 assigned to ventilate roof; RS1 splits crew; BC6 speaks to occupant of home on the street about the layout; BC9 sizes up B/C corner by looking around corner and observes smoke but no fire. - 1057 Hours
E24 and RS1A enter garage in an attempt to back up E26. BC9 goes to side B and forces sub-basement door and sees light smoke. - 1058 Hours
E32 on scene; Fire self-vents at C/D corner of basement when glass door fails. E24 and RS1A try to make entry at garage man door to attack the fire but are forced back by extreme heat and heavy black smoke; BC9 meets up with E11 on a 1 ¾" hoseline at basement door. - 1059 Hours
BC9 forces basement door on side B. E11 tries to make entry but are forced back by heat. BC9 radios IC," heavy fire and smoke" and requests second hoseline. E32 (Rapid Intervention crew (RIC)) is reassigned to back-up E11; The IC special calls another RIC. - 1100 Hours
BC6 has face-to-face with IC on structure's layout and notices severe change in conditions (heavy black smoke coming out of garage). - 1101 Hours
Heavy fire and black smoke observed on side C; IC tries several times to contact E26 via radio with no reply; IC thinks E26 is with BC9; E20 dispatched as RIC. - 1102 Hours
E32 crew with second line makes entry behind E11into basement; IC assigns BC6 to take T11 and search top 2 floors. BC6, T11 meet up with RS1B and E24 at front door. - 1105 Hours
T15 requests to ventilate roof. IC instructs to do so. BC6, E24, T11, and RS1B make entry through the front door; RS1A makes entry on side B with E11 and E32 to conduct search of basement. - 1107 Hours
BC6 has a thermal imaging camera (TIC) but zero visibility in the interior; E24 crew gets separated at bottom of first floor stairs in hallway. - 1108 Hours
E24 lieutenant finds Victim #1 in first floor foyer to basement and garage. Seconds later E24 FF finds Victim #2 in first floor hallway. - 1109 Hours
Conditions clearing and victims are brought out of garage. - 1110 Hours
IC requests 2 medic units. - 1111 Hours
IC requests a second alarm.
Personal Protective Equipment
The victims were wearing structural fire fighting coat and pants, gloves, hood, boots, structural fire fighting helmet with eye protection, self-contained breathing apparatus (SCBA) equipped with an integrated personal alert safety system (PASS), and a radio. Note: The remote speaker microphones (lapel mikes) were exposed to extreme temperatures which made them inoperable, primarily due to the cords burning through. The "push to talk" button on the radios would have had to been used to communicate. The National Personal Protection Technology Laboratory (NPPTL) evaluated the SCBAs and the summary evaluation report is included as Appendix One. The full report can be provided upon request. The victims' structural fire fighting gear and PPE were also examined by NPPTL to determine conformity to NFPA voluntary consensus standards. Note: This evaluation report will be added to this report as Appendix Two, when completed. NIOSH investigators do not believe that the PPE had any direct contribution to the two fire fighter deaths.
Weather
The weather was cloudy with an approximate temperature of 57°F. The relative humidity was 59% and the wind was from the south at 5.8 miles per hour.2 The weather did not play a role in the incident.
Investigation
At approximately 1045 hours, 3 engine companies, 2 truck companies, 1 heavy rescue squad, and 3 battalion chiefs were dispatched to a report of curtains on fire due to an electrical short at a single family residential structure. E26, with Victim #1 and Victim #2, arrived at approximately 1048 hours, positioned just north of the front door on side A of the fire structure on the narrow street. Victim #1 initially grabbed the CO2 extinguisher because of a reported electrical fire. After consulting with the occupant, Victim #1 and Victim #2 pulled a 1 ¾" hoseline off the engine and made entry through the front door (side A street level), noticing light smoke. Victim #1 radioed on the fireground channel that "smoke was showing and we have a working fire below grade." The transmission was acknowledged by both BC6 and DC 3.
E24 arrived at approximately 1051 hours and positioned down the hill to allow T11, who was still en route, to get around them. At approximately 1052 hours, E11and BC6 (shift relief BC with no assigned aide), traveling north with a view of side C of the structure, noticed no smoke or fire visible. E11 caught the hydrant just north of the structure and laid 3" supply lines to both sides of E26. BC6 drove around E11 and parked in a neighboring driveway just north of the fire structure. BC6 (initial IC) radioed E26 for their location and they replied they were trying to locate the fire. The IC walked to the front of the fire structure and radioed E26 again about their status but got no response. The E11 crew was in the process of building a wye, when the IC instructed them to get a 1 ¾" hoseline and some irons and go down the exterior wooden stairway of side B and make entry at the door that was below grade (see Diagram #8). At approximately 1053 hours, BC9 arrived on scene and was assigned to supervise fire attack group responsibilities per protocol as second due BC. BC9 followed the E26's hoseline through the front door and encountered the E26 crew (the victims) operating in the front hallway on the street level floor near the entrance to the garage and stairway to the basement. Victim #1 stated that the fire must be a floor below them. BC9 stated they would attack the fire from the B-side of the structure and exited the front door, but the victims did not follow. At approximately 1054 hours, the E24 crew made entry into the garage to check for access and attempt to intercept the E26 crew. They thought they heard what could have been SCBA cylinders clanging and hitting the floor just inside the doorway.
At approximately 1056 hours, T15 and DC3 arrived on scene. DC3 took command as IC. The IC assigned T15 to the roof for ventilation. RS1 signaled to command they were going to split their crew per their normal protocol while operating with an engine company: 2 crew members going on first floor (RS1A) and 2 crew members going to the second floor (RS1B). The IC acknowledged. The RS1A entered the garage and headed for the door in the right corner of the garage to meet up with E24, but struggled since the door was blocked by vehicles and storage boxes inside the garage. The IC did a face-to-face with BC6 and instructed BC6 to get a layout of the fire structure from a resident.
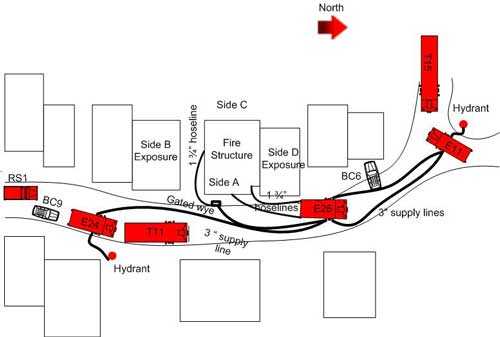
Diagram #8: Initial Apparatus and Hoseline Placement
At approximately 1057 hours, BC9 went down a debris filled path along the outside of the structure on side B to the wooden stairs connecting the basement door to the sub-basement door. He went to the sub-basement and forced the door open (see Photo 1). After seeing the room filled with light smoke, he looked around the B/C corner and saw smoke but no fire. BC6 located an older woman on the street, who resided at the fire structure and tried to get an understanding of the layout. At this point, dark smoke was observed about 2 feet off the ceiling in the garage. The smoke was not turbulent. At approximately 1058 hours, BC9 headed to the basement level man door. The fire self-vented out the glass door near the C/D corner (see Photo 2). BC9 forced the barred security door open with his halligan bar and then kicked the door open. The E11 crew advanced into the basement with the 1 ¾" hoseline. At the door, they felt a blast of heat and observed heavy smoke in the fully involved room. The heat forced the E11 fire fighter operating the nozzle to back up. BC9 radioed, "We have heavy fire and smoke and need a second line on side B." (see Photo 3).
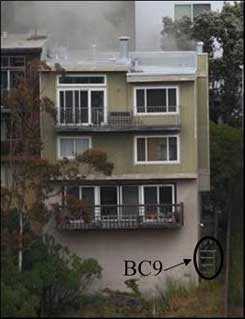

Photo 1 (left): BC9, lower right at bottom of external wooden stairs, kicking sub-basement door open. Light smoke showing at side A of fire structure.
Photo 2 (right): Fire self-vents out the glass door of the basement balcony near the C/D corner. Note: Fire highlighted in white.
(Courtesy of Fire Department)


Photo 3 (left): BC9 and E11 open exterior basement door.
Photo 4 (right): Heavy fire and smoke increased as E11 tried to make entry through the basement man-door. RS1A and E24 tried to make entry through garage.
(Courtesy of Fire Department)
E32 had arrived on scene and reported to "Command" minutes earlier as RIC but the IC reassigned them to back up E11 on side B. The IC requested another RIC company from dispatch. At approximately 1100 hours, the E24 crew and RS1A were in the garage trying to make entry into the house but were unable to get past the doorway due to the extreme heat (see Photo 4). BC6 went to the IC to explain the layout and had noticed the dramatic change in the smoke (i.e., from gray to dark in color, lofting to pressurized speed, and medium to heavy volume) coming out of the garage covering the command post in the street. The IC tried again to radio E26 but received no response. The IC radioed E26 again and heard a garbled response. The IC thought the E26 crew was on the hoseline and near BC9. At approximately 1102 hours, the E32 crew had deployed a charged 1 ¾" hoseline down to side B and made entry behind E11's crew and began to fight the fire (see Photo 5). The IC assigned BC6 to Division 3 (the second floor) and the crew from T11 to make entry at the front door to search the upper floors. When the T11 crew approached the door, RS1B had just come out. The two crews regrouped to go back in with BC6. E24 and RS1A backed out of the garage. RS1A proceeded to side B, E24 proceeded to the front door and met up with BC6, T11, and RS1B.

Photo 5: Water is getting on the fire.
(Courtesy of Fire Department)
At approximately 1105 hours, T15 radioed the IC that they were ready to vertically ventilate. The IC gave T15 the go ahead. At about that same time, RS1A made entry on side B after the E11 crew knocked down the large room and contents fire. RSA1 radioed command that they were conducting a primary search. E24, T11 and RS1B regrouped at the front door, BC6 instructed T11 to stay at the front door and help feed the hoseline as BC6, E24 and RS1B made entry. After entering the front door, BC6, E24 and RS1B followed the E26 hoseline. BC6 had a thermal imaging camera, but the soot and smoke were so heavy he could not see the camera screen in the zero visibility. In zero visibility conditions, the E24 crew advanced to the bottom of the stairs of the first floor hallway. The E24 lieutenant followed E26's hoseline which led him to a metal door to the foyer which led to the garage and basement stairs. He pushed open the door and found Victim #1 in the first floor foyer at the top of the stairs to the basement. Then seconds later, E24's fire fighter/paramedic found Victim#2 a few feet away in the first floor hallway just past the doorway to the foyer (see Diagram #9). Note: Victim #1 was found on his knees with his arms in a hunched over position in the foyer at the top of the basement stairs. Victim #2 was found face down in the hallway toward the bedroom. The E26 hoseline was found in the foyer with Victim #1 and the door partially closed on it (see Diagram #10).
About this time dispatch contacted command and stated that an E20 fire fighter’s radio emergency alarm bottom had been activated. Note: E20 was the replacement RIC and was en route. The IC didn’t see E20 on scene and knew that they hadn’t reported to command. The E24 crew could hear a PASS device going off. BC6 heard someone say we found a downed fire fighter and heard PASS alarms going off so he radioed a “Mayday” and reported that there was a downed fire fighter. Note: The Mayday by BC6 was overridden by dispatch’s information about E20’s emergency alarm. The lieutenant from RS1A came up the stairs from the fire floor and assisted the E24 lieutenant in carrying Victim #1 out the garage man door. While going along the garage wall and a vehicle, the victim’s low pressure SCBA hose and facepiece got caught underneath the vehicle’s tire. RS1A’s fire fighter cut the hose to expedite the extrication. The E24 fire fighter/paramedic moved Victim #2 into the foyer doorway to the garage then the fire fighter/paramedic came out of garage and yelled, “Need help, fire fighters down.” The fire fighter from RS1A came up the stairs from the fire floor to the foyer and assisted a T11 fire fighter with carrying Victim #2 outside through the garage. At approximately 1110 hours the IC radioed dispatch and urgently requested 2 medic units be sent; the IC requested a second alarm one minute later. The IC radioed BC6 and BC9 to report to the command post. The victims were transported to the local medical center where the lieutenant was pronounced dead. The fire fighter/paramedic died two days later from his injuries.
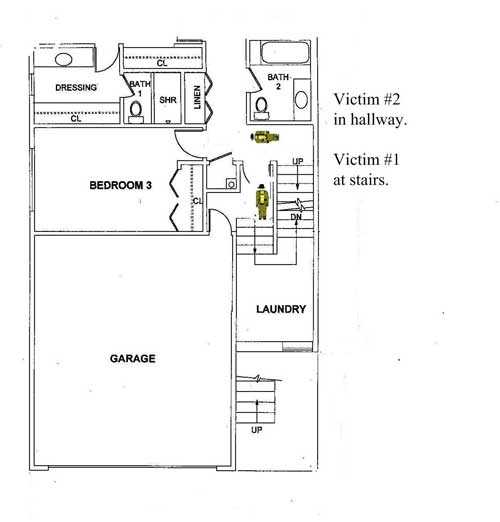
Diagram #9: Location of Victims Found on First Floor, side A of Structure
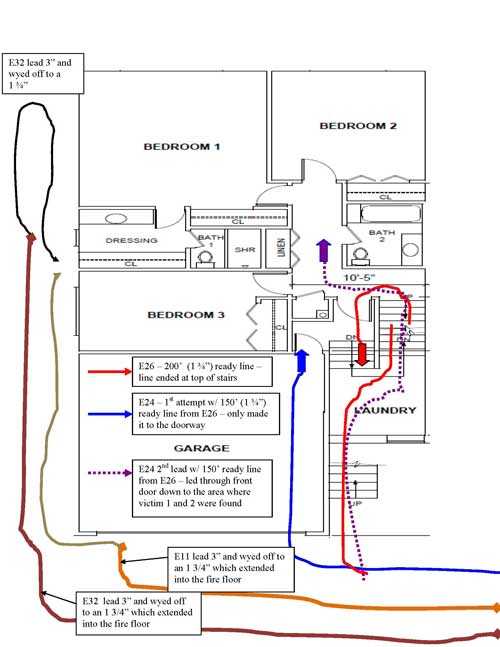
Diagram #10: Hose Placement in and around Structure up to the of Time of Incident
(Courtesy of the Fire Department)
Cause and Origin
According to the fire department's arson unit report, the fire originated in the basement on C side of the room. The ignition was likely a non-specific electrical sequence in the electrical wiring or appliances in that area. Forensic testing on possible electrical ignition sources are pending but this fire is currently being listed as accidental.3
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Construction features of the house built into a steep sloping hillside
- Natural and operational horizontal ventilation
- Ineffective size-up
- Fire fighters operating above the fire
- Ineffective fire command communications and progress reporting
- Lack of a personnel accountability system.
Cause of Death
The medical examiner's (ME) report stated that both firefighters died from complications from thermal injuries. Carbon monoxide was present in both fire fighters along with soot in their throats and lungs. Note: Both victims were found with their SCBA facepieces on and tests showed they were functional and would seal properly. No air was found in either SCBA but Victim #1's SCBA mask mounted regulator line was cut into during extrication. Victim #1 had 40-50% burns to his body and Victim #2 had 30-40% burns to his body. The burns around their faces are consistent with them wearing a facepiece and hood. The burns to the bodies were in areas protected by their PPE coats and pants, although, the PPE seemed to be in good condition. Note: Analysis of the PPE estimated that the victims were exposed to temperatures around 550 - 750 degrees F. The ME was not able to tell if the burns were from steam or heat.
Recommendations
Recommendation #1: Fire departments should ensure that standard operating guidelines (SOGs) are developed and implemented for hillside structures.
Discussion: Many cities and towns have structures built on hillsides that are community fire risk issue and pose a danger to fire fighters. Fires that occur in the below street level floors of these structures should be fought like basement fires. Generally, homes constructed on hillsides or sloping terrain have exterior doors or windows on the below grade floors which should be considered for use in the direct attack on the fire. Opening these below grade doors or windows to vent the floor may result in the fire intensifying but it confirms the location of the fire and provides an initial point of outside attack. Any stairwells above the fire will naturally serve as a chimney for the fires hot gases. Any fire fighter entering or caught in the stairwell will be exposed to the extreme heat and gases, and placed at extreme risk.
Placing an engine company at the top of the stairwell to the below grade fire floor to protect exposures and stop extension may prove effective as long as the crew is not in the stairwell and exposed to hot gases or fire that travels up the stairs due to the chimney effect.
Written SOGs enable individual fire department members an opportunity to read and maintain a level of assumed understanding of operational procedures. SOG's also serve as baseline reference documents for training and officer development. Conversely, fire departments can suffer when there is an absence of well-developed SOGs. The NIOSH Alert: "Preventing Injuries and Deaths of Fire Fighters" identifies the need to establish and follow firefighting policies and procedures.4 Guidelines and procedures should be developed, fully implemented and enforced to be effective. Periodic refresher training should also be provided to ensure fire fighters know and understand departmental guidelines and procedures.
During this incident, the E26 officer knew the fire was below him but he was unaware of just how many floors. If an adequate size-up had been conducted, or had the E26 officer obtained more intelligence information from the resident of the home that he spoke to briefly upon arrival, it may have facilitated a more rapid determination of the location of the fire floor.
Recommendation #2: Fire departments should ensure that an adequate size-up of the fire structure is conducted prior to crews making entry.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial 360 degree situational size-up of the incident.5 A proper size-up begins from the moment the alarm is received and it continues until the fire is under control. The size-up should include an evaluation of factors such as the fire size and location, access or barriers, length of time the fire has been burning, conditions on arrival, occupancy type, building construction and floor plan of the structure, fuel load and presence of combustible or hazardous materials, exposures, time of day, available staffing on scene or en route, and weather conditions. Information on the structure itself should include size, construction type, age, condition (e.g., evidence of deterioration, weathering), renovations, lightweight construction, loads on roof and walls (e.g., air conditioning units, ventilation ductwork, utility entrances), and available preplan information - all key information which will allow the IC to accurately determine the correct strategy, offensive or defensive, to be employed. The size-up should also include a continuous risk-versus-gain assessment during incident operations (especially after primary searches have been conducted6-11), periodic situational awareness check, and a survivability profile assessment, in order to keep the action plan current, size-up should be a continuous process as fire conditions change throughout the event.
Even before an officer takes command of an incident he will be faced with having to determine what critical tasks are going to have to be performed to bring the incident under control. He will use current knowledge and previous experience to formulate a plan for his arriving apparatus and personnel. When the IC arrives he needs to ascertain as much information as possible to make a determination whether the initial officer's plan is still working. The IC may be faced with several priorities such as an entrapped civilian, a larger scale incident then previously determined, and the fire environment itself. These additional considerations are part of the initial situational size-up and the risk assessment. These assessments will constantly change as the incident progresses until the incident is brought under control. The IC should be willing to prioritize and change his strategy and plan based on these assessments. Situational awareness is a highly critical aspect of human decision making that includes: the understanding of what is happening around you, projecting future situation events, comprehending information and its relevance, being realistic, and an individual's perception.12 Conducting accurate risk assessments and receiving interior/exterior status updates is critical to the safety of fire fighters in the incident, rescue/recovery efforts, and overall control of the incident. "The decision to commit interior fire-fighting personnel should be made on a case-by-case basis with proper risk-benefit decisions being made by the incident commander. The commitment of firefighters' lives for saving property and an unknown or marginal risk of civilian life must be balanced appropriately."13
Another tool that the IC should consider using is survivability profiling. Survivability profiling uses the knowledge learned of fire behavior and spread, smoke (i.e., color, condition, movement), and building construction to examine a situation and make an intelligent decision of whether to commit fire fighters to life saving and/or interior operations.14 In other words, survivability profiling involves assessing the probability that a trapped occupant is still alive and can safely be rescued with the current or impending conditions. The NIOSH publication Preventing Deaths and Injuries of Fire Fighters Using Risk Management Principles at Structure Fires15 states that the IC must make a determination that offensive (interior) operations may be conducted without exceeding a reasonable degree of risk to fire fighters before ordering an offensive attack and must be prepared to discontinue the offensive attack if the risk evaluation changes during the fire-fighting operation. The fireground is very dynamic, and conditions can either improve or deteriorate based on fire suppression activities and available resources. Most importantly, assessments/size-ups of the incident are necessary to detect a change on the fireground.5
In this incident, if an effective size-up would have been conducted several factors may have changed the first arriving companies’ tactics. The B side door would have been an option for initial entry. If the small window below the front door would have been noticed perhaps the fire could have been seen on the basement floor; or if more intelligence information would have been gathered from the occupant initially they could have identified that the fire was on the basement floor and how to access the floor.
Recommendation #3: Fire departments should ensure staffing levels are maintained.
Discussion: The National Fire Protection Association (NFPA) 1710 Standard identifies the minimum resources for an effective firefighting force to perform critical tasks. These tasks include establishing water supply, deploying an initial attack line, ventilating, performing search and rescue, and establishing a RIC. NFPA 1710 recommends that the minimum staffing levels for an engine company to perform effective and efficient fire suppression tasks is four.16 In addition, a recently released study by the National Institute for Standards and Technology (NIST), Report on Residential Fireground Field Experiments, concluded that a three-person crew started and completed a primary search and rescue 25 percent faster than a two-person crew and that four or five-person crews started and completed primary search and rescue 6 percent faster than a three-person crew.17
It is essential that staffing levels are sufficient to have a dedicated RIC at every fireground and that any on scene assignments will not hamper the RIC team's immediate response to the firefighter down or Mayday situation.5, 16, 18 The RIC, as well as being a dedicated crew, must have specialized rapid intervention equipment dedicated to the priorities of locating the downed firefighter, determining respiratory needs, supplying air if needed, conducting extraction from the IDLH environments if possible and/or protecting trapped fire fighters in place if necessary.19 The RIC training should comply with NFPA 1407.
The greatest enemy for the firefighter in a Mayday situation is typically time without air. This means that the strictest discipline and training to reduce the loss of time is critical for the fire fighter in trouble. Many RIC operations take far longer to extricate the victim to the outside than anticipated. The battle of time without air can be minimized by establishing air (use of rescue air) as a prerequisite to extrication. Then the RIC can focus on how to get the victim out or protect them in place.
During this incident, E32 was originally assigned as RIC then re-assigned fire fighting duties to back up E11. E20 was dispatched as RIC but did not arrived on scene until after the victims were recovered.
Recommendation #4: Fire departments should ensure that a personnel accountability system is established early and utilized at all incidents.
Discussion: An important aspect of an accountability system is the personnel accountability report (PAR). A PAR is an organized on-scene roll call in which each supervisor reports the status of his crew when requested by the IC or emergency dispatcher.6 The use of an accountability system is recommended by NFPA 1500 Standard on Fire Department Occupational Safety and Health Program20 and NFPA 1561 Standard on Emergency Services Incident Management System.21 A functional personnel accountability system requires the following:
- development of a departmental SOP
- training all personnel
- strict enforcement during emergency incidents.
The function of personnel accountability should be assigned to personnel who are responsible for maintaining the location and status of all assigned resources at an incident. This is a separate role from the duties of the Incident Commander. The Incident Commander is responsible for overall command and control of the incident. Due to the importance of responder safety, this function would be assigned to a Personnel Accountability Officer or Resource Status Officer. This function can be staffed by the chief’s aide, staff assistant, field incident technician, chief officer, or other responder familiar with the department’s accountability system.
There are many different methods and tools for accounting of resources. Some examples are:
- Tactical worksheets
- Command boards
- Apparatus riding lists
- Electronic bar-coding systems
- Accountability tags or keys (e.g. PASSPORT System).
The intent of each method is to track the fire fighters and first responders by function and location. The components of the personnel accountability system should be modular and expand based on the size and complexity of the incident.21
Another critical element that is essential to the success of the personnel accountability system is effective fireground or incident scene communications. The fire department should have a communications standard operating procedure (SOP) coupled with an effective training program. These procedures include the use of clear text (specifically, no “10 codes”, or other terms that may be unfamiliar to other responders) and providing a separate radio channel for dispatch and a separate tactical channel to be used initially during the incident. When a tactical level management unit is implemented, the fire department shall provide a dispatch channel, a command channel, and a tactical channel. The fire department shall provide the necessary number of radio channels relating to incidents with multiple tactical channels and the complexity of these incidents. NFPA 1500, section 8.2.2, states that a standard terminology will be established for transmitting information, strategic modes of operation, situation reports, and emergency notification of imminent hazards. The fire department should have procedures for the announcement of emergency conditions, using the term “emergency traffic” as a designation to clear radio traffic.20 Emergency traffic should be declared by the incident commander, tactical level management unit, or member who identifies a high risk situation on the fireground (i.e. power lines down, signs of impending collapse, etc.), or to be used to alert members that the IC is ordering the evacuation of the building. The term “Mayday” should be reserved for only those situations where a fire fighter is in trouble or facing a life threatening emergency.
The fire department should develop procedures when an emergency traffic or Mayday declaration is made. Standard operating procedures should also be developed for telecommunicators (dispatchers) to provide support to emergency incident operations. Telecommunicators should be trained to function effectively within the incident management system and should meet the requirements of NFPA 1061, Standard for Professional Qualifications for Public Safety Telecommunicator. NFPA 1500, section 8.2.4.1, states that the dispatch center should providethe incident commander with elapsed time-on-scene at emergency incidents in 10-minute intervals.
As the incident escalates, additional staffing and resources may be needed, adding to the burden of tracking personnel. The tactical worksheet or incident command board should be established early with an assigned accountability officer or aide. As a fire escalates and additional fire companies respond, a chief’s aide or accountability officer assists the incident commander with accounting for all firefighting companies at the fire, at the staging area, and at the rehabilitation area. With an accountability system in place, the incident commander may readily identify the location and time of all fire fighters on the fireground. A properly initiated and enforced accountability system that is consistently integrated into fireground command and control enhances fire fighter safety and survival by helping to ensure a more timely and successful identification and rescue of a disoriented or downed fire fighter.5 This department has developed and implemented SOPs governing accountability and even assigns an accountability officer to the IC to assist with radio transmissions and PARs.
In this incident, BC6 and the IC tried to radio E26 with no response and it was assumed they were with BC9 or that BC9 knew what they were doing. An additional supporting component to fireground accountability is frequent progress reporting. When the IC fails to get a response after 3 attempts, or he receives a garbled response, action must be taken to determine the crew’s status. A worst case scenario must be assumed until their status can be confirmed.
Recommendation #5: Fire departments should ensure that fireground operations are coordinated with consideration given to the effect horizontal ventilation has on the air flow, smoke, and heat flow through the structure.
Discussion: NFPA 1021, Standard for Fire Officer Professional Qualifications, section 4.6.1 and A.4.6.1(A), requires that all fireground operations conducted are based upon the overall strategy and incident action plan (IAP) developed by the IC. The essential element is to ensure that fireground operations (strategy, tactics and tasks) are coordinated and communicated so that everyone understands the plan. Strategy is the overall goal or goals of managing the incident. Tactics are selected and based on strategic goals and employed through tried and true fireground objectives — such as rescue, exposures, confinement and extinguishment of the fire, overhaul, ventilation and salvage. Based on size-up findings, the IC needs to prioritize the delivery of these tactics to put out the fire, ensure it stays out and conserves as much property as the complexity and fire size allows. The IC must train and prepare to develop a strategy and IAP based upon information acquired and factors observed for every incident. This practice provides the basis for a standard incident management approach to every incident. Decisions made and the actions they produce can be no better than the information on which they are based. A standard information management approach is the launching pad for effective incident decision making and successful operational performance. The IC must develop the habit of using the critical factors in their order of importance as the basis for making the specific assignments that make up the IAP.22 This standard approach becomes a huge help when it is hard to decide where to start.
The IC must create a standard information system and use effective techniques to keep informed at the incident. Information is continually received and processed so that new decisions can be made and old decisions revised based on new data and information received. The IC can never assume action-oriented responders engaged in operational activities will just naturally stop what they are doing so they can feed the IC a continuous supply of top-grade objective information. It is important that if the IC or Supervisor requests a progress report from a company with no response they should continue to make contact until they get a satisfactory report. The IC must do whatever is required to stay effectively informed.
During most critical incident situations, the IC many times must develop an IAP based only on the critical factor evaluation information available at the beginning stage of operations. Many times, that information is incomplete. Even though the IC will continue to improve the IAP's quality, the IC will seldom function during the fast, active periods of the event with complete or totally accurate information on all factors.
This is most evident during confused, time-compressed initial operations. This continual improvement in the accuracy and timeliness of incident information becomes a major IC function. The ability of the IC and the tactical and task level officers to quickly be informed and perform an analysis of the critical factors that can cause major physical and emotional setbacks to the responders and the customers will have a great impact on the health and longevity of the fire fighters, other first responders, the customers and their property.23, 24
With the amount of plastics and hydrocarbon-based products found in homes today and coupled with engineered building products, the increased intensity of fire growth and heat paths can have a significant impact on interior crews and their safety.25 Interior crews can face significant heat when searching for the seat of the fire, especially in an environment where minimal ventilation causes the retention of heat.26 This then poses the danger of a flashover when adequate ventilation occurs. Note: Crews mentioned the extreme amount of heat and black smoke that was at the garage man door which was in close proximity to where the victims were found.
At this incident, the officer on E26 realized that they had a fire somewhere in the structure, probably underneath them. The victims from E26 had deployed a 1¾” hoseline to the ground floor of the structure attempting to locate the fire. BC9 came into the structure and met them during their investigation of the ground floor. Victim #1 advised BC9 that the fire was underneath them. BC9 agreed to this and decided to take a crew down side B and attack the fire through the exterior doorway on side B at the basement level. BC9 and the IC discussed and agreed on this tactic. E26 did not receive any further instructions and did not leave the structure but attempted to go to the basement via the interior stairs. E26 did not provide any radio reports to the fire attack group supervisor (BC9) or the IC of their location or actions.
When an incident transitions from an investigation mode to an offensive fire attack mode, the IC should ensure that all companies have and understand their assignments, and are accounted for in the Personnel Accountability System. This information should be collected on a tactical worksheet to ensure that all companies have an assignment and are accounted for.
Recommendation #6: Fire departments should ensure that the Incident Commander is provided a chief's aide at all structure fires.
Discussion: A chief's aide, staff assistant, or field incident technician (FIT) is a position designed to assist an IC with various operational duties during emergency incidents. The chief's aide is an essential element for effective incident management and fire fighter safety. At an emergency incident, the staff assistant can support key incident management functions including: managing the tactical worksheet; maintaining personnel accountability of all members operating at the incident (resource status and deployment location); monitoring radio communications on the dispatch, command, and fireground channels; control information flow by computer, fax, or telephone; and, access reference material and pre-incident plans. .
The personnel accountability system is a vital component of the fire fighter safety process. The system is designed to account for and track personnel as they perform their fireground tasks. In the event of a "mayday," the personnel accountability system must be able to provide the rapid accounting of all responders at the incident. This is one of the chief's aide's essential responsibilities. Another important function is the role of a driver in addition to their role as part of the command team. Chief Officers are required to respond quickly to emergency incidents. In their response, they have to be fully aware of traffic conditions, construction detours, traffic signals, and other road hazards while they attempt to monitor, comprehend and answer radio traffic to assess which companies are responding, what is happening on the incident scene, develop a strategy for the incident based upon input from first arriving officers, develop and communicate an incident action plan which defines the strategy of the incident. A chief's aide can assist the chief officer in processing information without distraction and complete the necessary tasks en route to the scene.27 In the case of this incident, the BC was a relief officer and was not assigned an aide. Thus, the individual is responsible for operation of the vehicle during emergency response in any of the department's 9 battalions.
Departments should consider the aide to be an individual that has the experience and authority to conduct the required tasks. Other potential roles for the chief's aide include assisting with the initial size-up, completing a 360-degree size-up, and coordinating progress reports from group/division officers. The aide position can be used as a training position to help facilitate officer development.
In this incident, a chief’s aide may have helped the IC to establish and manage the tactical worksheet early in the incident, track the deployment location of the E26 crew, and monitor transmissions on the fireground channels.
Recommendation #7: Fire departments should ensure that an incident safety officer is assigned to all working structure fires.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System, "The incident commander shall have overall authority for management of the incident and the incident commander shall ensure that adequate safety measures are in place." This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the incident commander is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.21 According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program,20 "as incidents escalate in size and complexity, the incident commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) to assess the incident scene for hazards or potential hazards." These standards indicate that the incident commander is in overall command at the scene, but acknowledge that oversight of all operations is difficult. On-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO. Additionally, the incident commander relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk versus gain and offensive-versus-defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and the incident commander. NFPA 1521 Standard for Fire Department Safety Officer defines the role of the ISO at an incident scene and identifies duties such as recon of the fireground and reporting pertinent information back to the incident commander; ensuring the department's accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.28 Larger fire departments may assign one or more full-time staff officers as incident safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the incident commander. The presence of an incident safety officer does not diminish the responsibility of individual fire fighters and fire officers for their own safety and the safety of others. The ISO adds a higher level of attention and expertise to help the fire fighters and fire officers. The ISO must have particular expertise in analyzing safety hazards and must know the particular uses and limitations of protective equipment.8
In this incident, for the size of the fire department and responsible coverage area, there is an insufficient number of incident safety officers (ISO) and/or qualified personnel (certified to NFPA 1521) to act as an ISO within the fire department. The ISO should be of a rank worthy of the significant responsibility.
Recommendation #8: Fire departments should ensure that fire fighters are trained in Mayday procedures and survival techniques.
Discussion: The fire fighter needs to maintain situational awareness at all times while operating on the fireground. Fire fighters must understand that when they are faced with a life threatening emergency there is a very narrow window of survivability. Knowledge and skill training on how to prevent a Mayday situation or how to call a Mayday should begin and be mastered before a fire fighter engages in fireground activities or other immediately dangerous to life and health (IDLH) environments.5 Fire fighter training programs should include training on such topics as: air management; familiarity with an SCBA, a radio, and PPE; crew integrity; reading smoke, fire dynamics and behavior; entanglement hazards; building construction, and signs of pending structural collapse. If a fire fighter finds themself in a questionable position (dangerous or not), they must be able to recognize this and be trained on procedures for when and how a Mayday should be called. A fire fighter's knowledge, skill, and ability to declare a Mayday must be at the mastery level of performance. This performance level should be maintained throughout their career through training offered more frequently then annually.29
The ability of a fire fighter to call a Mayday is a complicated behavior that includes the affective, cognitive, and psychomotor domains of learning and performance.30 Any delay in calling a Mayday reduces the chance of survival and increases the risk to other fire fighters trying to rescue the downed fire fighter.
There are no rules on when a fire fighter must call a Mayday, and Mayday training is not included in NFPA fire fighter 1 or 2 standards.1 It is up to each authority having jurisdiction to develop rules and performance standards for a fire fighter to call a Mayday. The National Fire Academy Mayday courses present specific Mayday parameters or rules for when a fire fighter must call a Mayday. The courses may help fire departments in developing and teaching Mayday procedures for fire fighters.
The National Fire Academy has two courses addressing the fire fighter Mayday Doctrine: Q133 Firefighter Safety: Calling the Mayday, which is a 2-hour program covering the cognitive and affective learning domain of the fire fighter Mayday Doctrine; and, H134 Calling the Mayday: Hands-on Training which is an 8-hour course that covers the psychomotor learning domain of the fire fighter Mayday Doctrine. These courses are based on the military methodology used to develop and teach fighter pilots ejection doctrine. A training CD is available to fire departments free of charge from the U.S. Fire Administration Publications office.30-31 Also, the IAFF Fire Ground Survival program is another resource fire departments can use and was developed to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers, and chief officers.29
In this incident, there were no indications by either fire fighter that they were in trouble.
Additionally,
Recommendation #9: First responder radio manufacturers, research/design facilities and standard setting bodies should continue research and efforts to improve radio system capabilities.
Discussion: The use of personal protective equipment and an SCBA make it difficult to communicate, with or without a radio.32-33 Several NIOSH Fire Fighter Fatality Investigation Reports have cited issues with portable radio communication, and the International Association of Fire Chiefs has released an interim report concerning possible communications problems involving digital two-way portable radios in close proximity to common fireground noise.34
To facilitate communication, equipment manufacturers have designed facepiece-integrated microphones, intercom systems, throat mikes, and bone mikes worn in the ear or on the forehead.33, 35The National Institute for Standards and Technology (NIST) has recently tested portable radios in simulated fire fighting environments and has identified that radios are vulnerable to exposures to elevated temperatures. Some degradation of radio performance was measured at elevated temperatures ranging from 100 to 260 degree C, with the radios returning to normal function after cooling down. Additional research is needed in this area.36
During this incident, several issues occurred involving the radio, such as: garbled and unintelligible radio transmissions heard by the IC; the Mayday from BC6 being walked on by the dispatch; and the Victims' remote microphones being damaged by thermal environment.
Recommendation #10: States and municipalities should adopt and enforce regulations for automatic fire sprinkler protection in new buildings and renovated structures.
Discussion: The International Code Council's International Residential Code and the NFPA 101, Life Safety Code, require sprinkler protection in all new one-and two-family dwellings and in most other properties.37-38 Fire development beyond the incipient stage is one of the greatest hazards that fire fighters are exposed to. This exposure and risk to fire fighters can be dramatically reduced when fires are controlled or extinguished by automatic sprinkler systems. NFPA statistics show that most fires in sprinklered buildings are controlled prior to fire department arrival by the activation of one or two sprinkler heads. The presence of automatic fire sprinklers also reduces the exposure risk to fire fighters in rescue situations by allowing the safe egress of building occupants before the fire department arrives on scene. Finally, by controlling fire development, the exposure to hazards such as building collapse and overhaul operations are greatly reduced, if not eliminated.
References
- NFPA [2008]. NFPA 1001: Standard for Fire Fighter Professional Qualifications, Fire Fighter I and Fire Fighter II. 2008 ed. Quincy, MA: National Fire Protection Association.
- Weather History http://www.wunderground.com/cgi-bin/findweather/getForecast?query=zmw:94101.1.99999
- Arson Investigation Report [2011].
- NIOSH [1994]. NIOSH Alert: Preventing Injuries and Deaths of Fire Fighters. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No.# 94-125.
- IAFC Safety, Health, and Survival Section [2010]. Rules of engagement of structural firefighting (poster). International Association of Fire Chiefs, Safety, Health and Survival Section [http://websites.firecompanies.com/iafcsafety/files/2013/10/ROE_Poster_FINAL1.pdf]. Date accessed: January 2012. (Link Updated 1/14/2014)
- IFSTA [2008]. Essentials of Fire Fighting. 5th ed. Stillwater, OK: Fire Protection Publications, International Fire Service Training Association.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook NJ: Fire Engineering Books and Videos.
- Dunn V [2000]. Command and control of fires and emergencies. Saddle Brook, NJ: Fire Engineering Book and Videos.
- Brunacini AV [1985]. Fire command. Quincy, MA: National Fire Protection Association.
- Dunn V [1998]. Risk management and lightweight truss construction. With New York Firefighters (WNYF) 58(1).
- NIOSH [1999]. NIOSH alert: request for assistance in preventing injuries and deaths of firefighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 99-146.
- Endsley MR, Garlan J [2000]. Situational awareness analysis and measurement. Mahwah, NJ: Lawrence Erlbaum Associate.
- Jones J [2001]. No empty threat. Fire Chief Nov 1 [http://firechief.com/mag/firefighting_no_empty_threat/]. Date accessed: November 2011.
- Marsar S [2010]. Survivability profiling: are the victims savable? Fire Engineering Apr 4. [http://www.fireengineering.com/articles/2009/12/survivability-profiling.html]. (Link Updated 8/16/2012) Date accessed: November 2011.
- NIOSH [2010]. NIOSH alert: preventing deaths and injuries of fire fighters using risk management principles at structure fires. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health (NIOSH) Publication No. 2010-153.
- NFPA [2010]. NFPA 1710: Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations, and Special Operations to the Public by Career Fire Departments. 2010 ed. Quincy, MA: National Fire Protection Association.
- NIST [2010]. Report on Residential Fireground Field Experiments. NIST Technical Note 1661, April 2010. http://www.nist.gov/customcf/get_pdf.cfm?pub_id=904607. Date accessed: November 2011.
- IAFC Safety, Health, and Survival Section [2010]. Rules of Engagement of Structural Firefighting. [http://websites.firecompanies.com/iafcsafety/files/2013/10/Rules_of_Engagement_short_v10_2.12.pdf]. Date Accessed: November 2011. (Link Updated 1/14/2014)
- NFPA [2010]. NFPA 1407: Standard for Training Fire Service Rapid Intervention Crews. 2010 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 Standard on Fire Department Occupational Safety and Health Program. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1561 Standard on Emergency Services Incident Management System. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1021 Standard for Fire Officer Professional Qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- FEMA [1996]. Risk Management Practices in the Fire Service, 1996. Washington, DC: Federal Emergency Management Agency.
- Brunacini AV and Brunacini N [2004]. Command Safety. Across the Street Publications.
- Lee, M [2008]. Fireground Tactics Priorities – RECEO VS. FireRecruit.com. http://www.firerecruit.com/articles/426027-Fireground-Tactical-Priorities-RECEO-VS. Date accessed: August 23, 2011.
- Lee, M [2007]. Be Alert to Basement Fire Hazards. FireRescue1. Com. http://www.firerescue1.com/fire-attack/articles/291024. Date accessed: August 23, 2011.
- Ciarrocca M & Harms T [2011]. Help on the scene. FireRescue Magazine. February 2011, vol 29, issue 2. Pp 40-48.
- NFPA [2008]. NFPA 1521 Standard for Fire Department Safety Officer. 2008 ed. Quincy, MA.
- IAFF. IAFF Fire Ground Survival Program. International Association of Fire Fighters. [http://www.iaff.org/HS/FGS/FGSIndex.htm]. Date accessed: January 2012.
- Clark, BA [2005]. 500 Maydays called in rookie school. [http://www.firehouse.com/article/10498807/500-maydays-called-in-rookie-school]. (Link Updated 8/16/2012) Date accessed: January 2012.
- Clark BA [2008]. Leadership on the line: firefighter mayday doctrine where are we now? Radio@Firehouse.com [http://www.firehouse.com/podcast/10459336/leadership-on-the-line-firefighter-mayday-doctrine-where-are-we-now]. (Link Updated 8/16/2012) Date accessed: January 2012.
- Davis WD, Donnelly MK, Selepak MJ [2006]. Testing of portable radios in a fire fighting environment. Gaithersburg, MD: National Institute of Standards and Technology, Building and Fire Research Laboratory, NIST Technical Note 1477.
- USFA/FEMA [1999]. Improving firefighter communications. Emmitsburg, MD: United States Fire Administration, USFA-TR-099.
- International Association of Fire Chiefs [2008]. Interim Report and Recommendations: Fireground Noise and Digital Radio Transmissions, http://www.iafc.org/associations/4685/files/digProj_DPWGinterimReport.pdf, Accessed June 3, 2009.
- TriData Corporation [2003]. Current status, knowledge gaps, and research needs pertaining to fire fighter radio communication systems (http://www.cdc.gov/niosh/fire/RadComSy.html) Arlington, VA: TriData Corporation. Report prepared for NIOSH. Date accessed June 3, 2009.
- NIST [2007]. Advanced fire service technologies program. Proceedings of the 2007 NIST Annual Fire Conference. Gaithersburg, MD: National Institute of Standards and Technology, Building and Fire Research Laboratory.
- International Code Council [2009]. International Residential Code for One and Two-Family Dwellings. 500 New Jersey Avenue, NW, 6th Floor, Washington, DC 20001.
- NFPA [2010]. NFPA 101: Life Safety Code. 2010 ed. Quincy, MA: National Fire Protection Association.
Investigator Information
This incident was investigated by Matt E. Bowyer, General Engineer and Murrey Loflin, Investigator, with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. Expert technical reviews were provided by John Tippett, Deputy Chief, Charleston Fire Department and Gary Morris, Fire Chief (Retired) and Consultant. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
APPENDIX ONE
Status Investigation Report of Two
Self-Contained Breathing Apparatus
Submitted By the
Fire Department
NIOSH Task Number 17888
(Note: Full report is available upon request)
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate two SCBA identified as Scott Health and Safety model AirPak, 4.5, 4500 psig, 45-minute, self-contained breathing apparatus (SCBA). This SCBA status investigation was assigned NIOSH Task Number 17888. The NIOSH Division of Safety Research (DSR) was advised that NIOSH/NPPTL/TEB would provide a written report of the inspections and any applicable test results. The SCBA units, contained within corrugated cardboard boxes, were delivered to the NIOSH facility in Bruceton, Pennsylvania, on June 22, 2011. After their arrival, the packages were taken to building 20 and stored under lock until the time of the evaluations.
SCBA Inspection
The packages were opened initially in the General Inspection Area (building 20) on August 24 and 25, 2011, and an initial visual inspection was conducted by Tom Pouchot, General Engineer at the National Personal Protective Technology Laboratory (NPPTL), Technology Evaluation Branch (TEB). The SCBA identified as Victim #1’s unit was labeled by NPPTL as SCBA Unit #1. The SCBA identified as Victim #2’s unit was labeled by NPPTL as SCBA Unit #2. The units were identified as the Scott Health and Safety Company model AirPak, 4.5, 45-minute, 4500 psig unit, NIOSH approval number TC-13F-0212. These SCBA units were examined, component by component, in the condition received to determine the conformance of the unit to the NIOSH-approved configuration. The visual inspection process was documented photographically.
Appendix I in the complete report summarizes the complete SCBA inspections. Appendix III in the complete report shows the condition of each major component of the SCBA that was photographed with a digital camera.
It was judged that only Unit #2 could be safely pressurized and tested, using a replacement cylinder.
SCBA Testing
The purpose of the testing was to determine the conformance of each SCBA to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing was conducted to provide an indication of the conformance of each SCBA to the National Fire Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of 42 CFR 84):
1. Positive Pressure Test [§ 84.70(a)(2)(ii)]
2. Rated Service Time Test (duration) [§ 84.95]
3. Static Pressure Test [§ 84.91(d)]
4. Gas Flow Test [§ 84.93]
5. Exhalation Resistance Test [§ 84.91(c)]
6. Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981, 1997 Edition):
7. Air Flow Performance Test [Chapter 5, 5-1.1]
Unit #2 was tested on September 18 and September 26, 2011.
Appendix II contains the complete NIOSH and NFPA test reports for Unit #2 SCBA. Tables One and Two summarize the NIOSH and NFPA test results.
Summary and Conclusions
Two SCBA units were submitted to NIOSH by the NIOSH Division of Safety Research for the San Francisco, California, Fire Department for evaluation. The SCBA units were delivered to NIOSH on June 22, 2011, and inspected on August 24 and 25, 2011. The units were identified as a Scott Health and Safety model AirPak 4.5, 4500 psig, 45-minute, SCBA (NIOSH approval number TC-13F-0212). The units suffered minimal heat damage, exhibited other signs of wear and tear and the units were covered with soot. The cylinder valves as received, Unit #1 was in the closed position and Unit #2 was in the closed position. The cylinder gauges read approximately 0 psig on Unit #1 but could not be read on Unit #2. The cylinder valve hand-wheels could be turned. The regulator and facepiece mating and sealing areas on the units were relatively clean and there was very little debris on the inside of the facepieces. The rubber faceseals were in good shape. The harness webbing on the units was in good condition with no fraying or tears but the webbing was dirty. The low pressure hose on Unit #1 was cut through. The PASS device on the units functioned. The SCBA NFPA approval labels on the units were present and readable. Visibilities through the lens of the unit facepieces were poor as the lenses were covered with soot and black.
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH “Fire Fighter Fatality Investigation and Prevention Program” which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research