


Volunteer Lieutenant Killed and Two Fire Fighters Injured Following Bowstring Roof Collapse at Theatre Fire – Wisconsin
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2012-08 Date Released: October 11, 2012
Executive Summary
On March 4, 2012, a 34-year-old male volunteer lieutenant (the victim) lost his life at a theatre fire after the roof collapsed, trapping him within the theatre. At approximately 1215 hours, an on-duty patrol officer (also chief of the victim's fire department) radioed dispatch for a structure fire (flames visible). The 1st due fire department arrived on scene, set up operations on the A-side of the structure, and directed the incoming mutual aid department (victim's department) to the rear of the structure. No fire was visible from the rear. Both departments attacked the theatre fire from opposite sides (A-side and C-side) of the structure establishing their own incident commander/officer in charge, fireground operations, and accountability systems. The 1st due fire department initially fought the fire defensively from the A-side, while the victim and two additional fire fighters (FF1 and FF2) entered through the C-side, advancing a hoseline until they met A-side fire fighters near the theatre's lobby (area of origin). The 1st due fire department eventually placed an elevated master stream into operation, directing it into the lobby and then onto the roof while fire fighters were operating inside. Roof conditions deteriorated until the roof collapsed into the structure trapping the victim, FF1, and FF2. FF1 and FF2 recalled speaking with the victim immediately following the collapse, but nothing was heard from the victim following the activation of a personal alert safety system device (PASS). All three were eventually located, removed from the structure, and transported to a local hospital, but the victim had already succumbed to his injuries.

Incident scene when fire was first discovered.
(Photo courtesy of Julie Miklaszewicz.)
Contributing Factors
- Initial arriving units not establishing/performing/implementing an incident management system, an overall incident commander, an incident action plan (IAP), and a 360-degree situational size-up
- Risk management principles not effectively used
- Fireground and suppression activities not coordinated
- Fire ground communications between departments not established
- Incident safety officer (ISO) role ineffective
- Rapid intervention crew (RIC) procedures not followed and/or implemented
- Bowstring roof truss construction not recognized by departments
- Fire burned undetected within the roof void space for unknown period of time
- Uncoordinated master stream operations
- Location of victim following roof collapse not immediately known.
Key Recommendations
- Fire departments should ensure that an effective incident management system is established with a designated incident commander not involved with fire suppression activities
- Fire departments should ensure that a complete situational size-up is conducted on all structure fires
- Fire departments should use risk management principles at all structure fires
- Fire departments should work together to develop mutual aid standard operating procedures for fireground operations that support interagency operability and accountability and train on those procedures
- Fire departments should ensure that the incident safety officer (ISO) position, independent from the incident commander, is appointed and effectively utilized at every structure fire meeting the requirements within NFPA 1521 Standard for Fire Department Safety Officer
- Fire departments should ensure that a rapid intervention crew (RIC) is readily available, on scene, and prepared to respond to fire fighter emergencies.
Introduction
On March 4, 2012, a 34-year-old male volunteer lieutenant (the victim) lost his life at a theatre fire after the roof collapsed, trapping him within the theatre. On March 5, 2012, the U.S. Fire Administration notified the National Institute for Occupational Safety and Health (NIOSH) of this incident. On March 12 through March 17, 2012, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program traveled to Wisconsin to investigate this incident. The NIOSH investigators met with the two fire departments' fire chiefs, Wisconsin occupational safety and health inspectors, and a state fire prevention coordinator.
Interviews were conducted with the incident commanders (IC) for the 1st due department, the officers in charge for the mutual aid department, fire department members directly involved with the incident, and one of the theatre's owner. The NIOSH investigators visited, documented, and photographed the fire scene and structure. The NIOSH investigators reviewed photographs and video taken by law enforcement, bystanders, and the theatre insurance adjuster. The NIOSH investigators also reviewed available training records for the victim, the ICs, and fire fighters working with the victim at the time of the collapse; dispatch radio transcripts; medical examiner's cause of death; and individual departmental standard operating guidelines (SOGs) for each department.
The NIOSH investigators documented the condition and took photographs of the victim's personal protective equipment (PPE) and self-contained breathing apparatus (SCBA). The victim's PPE and SCBA were sent to NIOSH's National Personal Protective Technology Laboratory (NPPTL) for further evaluation. The NIOSH investigators also reviewed available SCBA maintenance records for both departments.
Fire Departments
At the time of this incident, the 1st due fire department was operating from a single fire station with 26 members serving a population of approximately 2,300 within an area of about 22 square miles. This fire department had an engine, two tankers, a ladder truck (pump capable), a rescue truck, a brush truck, and two ambulances. The department provided fire and EMS services within its jurisdiction, responding to approximately 50 calls per year (approximately two structure fires per year). Members within the department received an hourly rate per call and officers received a monthly stipend. At the time of this incident, this fire department was rated as a Class 5 by the Insurances Services Organization (ISO).a In the ISO rating system, Class 1 represents exemplary fire protection, and Class 10 indicates that the area's fire-suppression program does not meet ISO's minimum criteria. This department provided annual medical evaluations and respiratory fit testing for its members.
At the time of this incident, the mutual aid fire department (victim's department) was operating from a single fire station with 25 members serving a population of approximately 2,500 within an area of about 99 square miles. The department also had a substation housing additional apparatus. This department had two engines, two tanker/engines, three tankers, a brush truck, and two ambulances. The department provided fire and EMS services within its jurisdiction, responding to approximately 40 calls per year (one or two structure fires per year). Members within this department received an hourly rate per call and officers above the rank of lieutenant received a monthly stipend. In 2010, this fire department received an ISO Class 5 rating. The victim's department does not provide medical evaluations or respirator fit testing.
Both departments had a designated safety officer who coordinated the departmental medical and safety and health issues of their members. When available, this safety officer or a designated safety officer would be utilized as an incident safety officer at emergency incidents.
The NIOSH investigators reviewed written standard operating guidelines for the 1st due fire department and the suggested operations guide for the mutual aid fire department (victim's department). Most if not all procedures/guidelines included within these documents are listed below and some procedures/guidelines were expanded upon within this report as it related to this incident.
The 1st due fire department’s SOGs1 (revised in 2008) contained the following information:
- Fire department general requirements
- Job descriptions
- Officer duties
- Member responsibilities
- Orientation program
- Protective clothing
- SCBA units
- Engine operations
- Communications
- Plain language
- Provide size-up
- Advise incoming mutual aid departments of incident type
- Know radio frequencies
- Auto accidents
- Driver training program
- Driving regulations
- Training
- Hazardous materials
- Alarm guidelines
- Quadrant system
- Responding
- Size-up
- Rescue
- Vehicle fires
- Auto accident with injuries
- Chimney fires
- Structure fires
- General
- A single long horn blast and/or three pulses in water pressure on the hose indicates to anyone inside the structure should exit immediately.
The mutual aid fire department's (victim's department) suggested operations guide2 contained the following information:
- Ordering equipment and supplies
- Emergency/Nonemergency carbon monoxide response
- Fire ground officer duties
- Mutual aid incident commander (IC) (pertains to EMS incidents only)
- Accountability
- Use a single identification tag
- Red – Attack Team
- Blue – Support Team
- Yellow – Truck Team
- Remove identification tag after arrival on scene
- Place in front seat of primary engine, rescue, or first truck on scene
- Mutual aid incidents
- Follow same procedure (above mentioned)
- Safety officer maintains communication with mutual aid department’s safety officer so that information on member whereabouts can be shared
- Use a single identification tag
- Receiving emergency calls
- Ambulance response
- Emergency equipment mutual aid response
- Apparatus emergency response, safe operation, and placement
- Incident commander (effective date 1995)
- Assigned at all emergency scenes
- Working knowledge of incident command system (ICS)
- Mutual aid incidents
- Primary jurisdiction will be the IC
- Incident command system (effective date 1993)
- Establishing command and command post
- Command functions
- Initial report and size-up
- Responsibilities
- Command options
- Level I and II staging
- Use of sectors
- Safety
- Incident command system fireground safety (effective date 1993)
- Positioning of operating companies
- Opposing fire streams
- Combining interior/exterior fire attack, front/rear fire attack, and roof/interior fire attack (utilize radio or face-to-face communications to coordinate)
- Under involved roof structures
- Where fire can move behind fire fighters
- Notify and evacuate interior crews before ladder pipe operations go into operation
- Structural collapse
- Always a possibility when support members are exposed to fire and heat, especially in peaked or domed roofs
- Age and type of building
- Search and Rescue
- Efficient, well planned procedure
- Personnel familiar with search and rescue plan before entering
- Accountability
- Positioning of operating companies
- Personal alert safety system (PASS) (effective date 1993)
- SCBA (effective date 1993)
- PPE (effective date 1993)
- Live fire training (effective date 1993)
- Safety officer (effective date 1993)
- Emergency evacuation of hazardous areas (effective 1993)
- “Code Red Signal”
- “Code red, code red” transmitted over pa system
- Sound siren and horn of apparatus for 30 uninterrupted seconds
- Personnel respond to primary engine for accountability
- Rapid intervention teams (RIT) (effective 2011)
- Follow National Fire Protection Association (NFPA) 1407 Standard for Fire Service Rapid Intervention Crews3
- Shall be activated at all structure fires
- Personnel should be entry level fire fighters and participate in monthly RIT training
The two departments' written SOGs and/or suggested guidelines that were reviewed were generic and provided minimum guidance for fireground operations. The two departments had developed these documents for their individual departments, but no mutual aid SOGs for emergency incidents (e.g., fireground operations/communications, evacuation, accountability) had been developed. Neither fire department had policies, guidelines, or procedures related to a Mayday, engine/truck company operations, building construction, fire behavior, or risk management principles; and neither department was aware of NFPA 1500 Standard on Fire Department Occupational Safety and Health Program.4 All fire and EMS departments within the county had signed a mutual aid agreement. Neither of the departments' safety officers (SO) had any formal incident safety officer training.
The Wisconsin Department of Safety and Professional Services standard SPS 330 Fire Department Safety and Health Standards5 enforce safety and health standards for public sector fire department employees. This document included the following subchapters:
- Purpose and scope
- Definitions
- Administration and enforcement
- Adopted standards
- NFPA 1001 Standard for Fire Fighter Professional Qualifications6 (1997 ed.)
- NFPA 1002 Standard for Fire Apparatus Driver/Operator Professional Qualifications7 (1998 ed.)
- NFPA 1021 Standard for Fire Officer Professional Qualifications8 (1997 ed.)
- NFPA 1403 Standard on Live Fire Training Evolutions in Structures9 (1997 ed.)
- NFPA 1901 Standard on Automotive Fire Apparatus10 (1999 ed.)
- NFPA 1911 Standard for Service Tests of Pump Systems on Fire Department Apparatus11 (1997 ed.)
- NFPA 1914 Standard for Testing Fire Department Aerial Devices11 (1997 ed.)
- NFPA 1971 Standard on Protective Ensemble for Structural Fire Fighting12 (2000 ed.)
- NFPA 1981 Standard on Open-Circuit Self-Contained Breathing Apparatus for the Fire Service13 (1997 ed.)
- NFPA 1982 Standard on Personal Alert Safety Systems14 (1998 ed.)
- NFPA 1983 Standard on Fire Service Life Safety Rope and System Components15 (2001 ed.)
- Organization
- Training and education
- Vehicles and equipment
- Protective clothing and protective equipment
- Emergency operations
- Facility safety
- Medical
- Member assistance referral program
- Miscellaneous activities
- Hazardous materials
- Confined spaces
- Diving operations
- Miscellaneous hazardous situations
aThe Insurances Services Organization (ISO) is an independent commercial enterprise that helps customers identify and mitigate risk. ISO can provide communities with information on fire protection, water systems, other critical infrastructure, building codes, and natural and man-made catastrophes. ISO's Public Protection Criteria program evaluates communities according to a uniform set of criteria known as the Fire Suppression Rating Schedule. More information about ISO and their Fire Suppression Rating Schedule can be found at http://www.isogov.com/about/.
Training and Experience
The victim had been with his department for approximately 10 years. He held certifications in Fire Fighter I, meeting requirements of NFPA 1001 Standard for Fire Fighter Professional Qualifications,6 emergency medical technician, IS-700 National Incident Management System (Federal Emergency Management Agency [FEMA]/Emergency Management Institute [EMI]), and LP gas emergencies. He had held the rank of lieutenant within the department for the past year. He was also a detective in the sheriff's department of a neighboring county. From 2010, until the day of the incident, the victim had attended approximately 30 training courses offered at the fire department and had responded to approximately 17 fire/EMS calls.
The initial IC for the 1st due fire department had been with this department for approximately 15 years, holding the rank of 2nd assistant chief for the past 2 years. He held certifications as a Wisconsin Entry Level Firefighter in 1999 (60 hours), Incident Safety Officer in 2004 (FEMA/EMI), Wisconsin Entry Level Driver Operator in 2003 (30 hours), OSHA 29 CFR 1910.120 Annual HAZWOPER, environmental response training, and first responder. He had also completed documented courses on the incident command system, such as IS-700 National Incident Management System in 2005 (FEMA/EMI); IS-100 Introduction to the Incident Command System in 2006 (FEMA/EMI); IS-800.a National Response Plan (NRP), An Introduction in 2006 (FEMA/EMI); Intermediate Incident Command System (ICS-300) in 2007 (Wisconsin Emergency Management); 12-hour Incident Command Systems 400 course in 2008 (local technical college); IS-200.a ICS for Single Resources and Initial Action Incidents in 2009 (FEMA/EMI).
The second IC for the 1st due fire department who assumed command of the scene during fire fighting operations and was in command at the time of the collapse had been with this department for approximately 22 years, holding the rank of fire chief for the past 2 years. He held certifications in Fire Fighter I (1996), Wisconsin Entry Level Driver Operator in 2003 (30 hours), Incident Safety Officer in 2004 (FEMA/EMI), and OSHA 29 CFR 1910.120 Annual HAZWOPER. He had also completed documented courses on ICS such as IS-100 Introduction to the Incident Command System in 2006 (FEMA/EMI); IS-800.a National Response Plan (NRP), An Introduction in 2006 (FEMA/EMI); Intermediate Incident Command System (ICS-300) in 2007 (Wisconsin Emergency Management); and a 12-hour Incident Command Systems 400 course in 2008 (local technical college).
Information related to training and experience for the mutual aid officers in charge was not readily available at the time of the NIOSH investigation.
Neither fire department had a fire training center or a formal fire recruit training academy for new members. Individuals wishing to become a volunteer fire fighter within the state of Wisconsin had to complete a state of Wisconsin Fire Fighter I course (equivalent to NFPA 1001) within a year of joining any volunteer department. During this time, entry into structure fires was prohibited. The Wisconsin Department of Safety and Professional Services requires fire departments to maintain a training and education program biannually or more often, if necessary, to prevent occupational accidents, deaths, injuries, and illnesses.5 Both departments usually acquired 1-3 structures a year to perform live burns for training. NFPA 1403 Standard on Live Fire Training Evolutions3 was followed during these training sessions. However, no mutual aid training between the two departments had been conducted.
Equipment and Personnel
The initial dispatched (by radio) assignment included the first due department with mutual aid assistance from the victim's department. The following units responded to the incident scene following the initial dispatch:
1st Due Fire Department
- Engine 1 (E1) with a driver, three fire fighters, and 2nd assistant chief (1st IC for 1st due department)
- Ladder 1 (L1) with the driver/operator and a fire fighter (accountability officer)
- Engine 5 (E5) with driver and 1st assistant chief
- Tanker 1 (T1) with the fire chief (2nd IC for 1st due department)
- Safety officer (SO) responded in the department’s rescue truck
- Additional support personnel responded by POV and/or department support units
Mutual Aid Fire Department (victim's department)
- Tanker/Engine 1 (TE1) with a driver/pump operator and the 1st assistant mutual aid chief (initial officer in charge for the victim’s department)
- Engine 2 (E2) with a driver, three fire fighters (one is FF1), and the 2nd assistant mutual aid chief (2nd officer in charge for the victim’s department)
- Engine/Rescue 1 (ER1) with a driver, a fire fighter (FF2), and lieutenant (the victim)
- Additional support personnel responded by POV and/or department support units
Following the collapse, two additional mutual aid fire departments, several ambulances, and an aeromedical unit were dispatched to assist with search/rescue, salvage/overhaul, and medical treatment.
Water Supply
The town's municipal water supply with hydrants was available during this incident; however, the 1st due fire department was delayed in establishing water to E1 because the 6-inch supply hose was charged while connected to other hose sections still bedded in E1's hose bed. The victim's department had no delay in supplying their apparatus from another hydrant located near the rear of the theatre.
Timeline
This timeline is provided to set out, to the extent possible, the sequence of events according to recorded and intelligible radio transmissions. Times are approximate and were obtained from review of the dispatch records, witness interviews, and other available information. Times have been rounded to the nearest minute. At the time of this incident, the 911 center did not monitor or record individual fire department fireground channels. Units responding to this incident marked en route as their perspective fire departments and may not have indicated their individual apparatus identification number. NIOSH investigators have attempted to include all intelligible radio transmissions, but some may be missing. This timeline is not intended, nor should it be used, as a formal record of events.
- 1215 Hours
The police dispatch center received emergency traffic over the police dispatch channel for a structure fire at a theatre. Note: The patrol officer who called in the theatre fire was also the fire chief for the mutual aid department (victim's department). - 1216 Hours
1st due department dispatched to a theatre fire. - 1217 Hours
1st due department dispatched again to the theatre fire.
A unit from this department acknowledged the call.
The dispatcher advised this unit that the first due mutual aid fire department had also been dispatched (at the request of the patrol officer on scene). - 1219 Hours
EMS units dispatched.
1st due department dispatched a third time. - 1220 Hours
Over the dispatch channel, the patrol officer advised dispatch and responding units that the theatre was empty and that the B/D-side exposures had been evacuated. - 1221 Hours
A unit from the 1st due department transmitted "flames showing." - 1223 Hours
A unit from the mutual aid department marked en route to incident.
L1 asked where to position their apparatus. - 1224 Hours
The patrol officer stated, "First due fire department IC, if you got a truck to go around to the east side there is an awful lot of smoke coming out the back end as well." - 1226 Hours
Patrol officer advised the mutual aid department to try and get their tanker/engine around the back side and into the alley. - 1238-1245 Hours
1st due fire department fire chief had several radio conversations with dispatch regarding utilities, who was responsible for them, and the need to have them turned off. - 1245 Hours
Victim and his crew entered into the theatre from the C-side. - 1257 Hours
The 1st due fire department fire chief (who is now the IC) requested full staffing from the next due mutual aid and EMS departments. Note: The roof had collapsed into the auditorium by this time but no mention of this or of trapped fire fighters was relayed to the dispatcher. - 1259 Hours
Next due mutual aid department for fire and EMS dispatched.
Patrol officer asked dispatch to page out an EMS unit from his department. - 1309 Hours
Next due mutual aid fire department on scene. - 1326 Hours
EMS unit transported one of the trapped fire fighters to the hospital. - 1328 Hours
An aeromedical unit was requested to respond to the scene. - 1329 Hours
The aeromedical unit was advised people are inside the "building." - 1337 Hours
A second EMS unit transported the second trapped fire fighter to the hospital.
Note: The dispatch records do not identify at what time the victim was discovered and then removed from the theatre.
Personal Protective Equipment
It was reported to NIOSH investigators that the victim, FF1, and FF2 entered the structure wearing a full array of personal protective clothing and equipment, consisting of turnout gear (coat and pants), gloves, boots, a hand-held radio (no extended mics), SCBA with an integrated PASS device, Nomex® hoods and helmet. Note: The hand-held portable radios did not have a programmed emergency button. The victim's facepiece was properly connected to his mask-mounted-regulator and was reported to be appropriately positioned about his face prior to the collapse and when located in the debris. The victim's facepiece showed signs of thermal degradation (see Photo 1) and the immediate pressure hose had been burned through. The victim's SCBA cylinder was empty. The last flow test on the SCBA was conducted in 2010 due to budgetary constraints.
The victim's SCBA was evaluated by the NIOSH National Personal Protective Technology Laboratory (NPPTL) to determine conformity to the NIOSH-approved configuration (see Appendix I). Information contained in the PASS device data logger was also downloaded with assistance from the SCBA manufacturer (see Appendix II). The victims' structural fire fighting gear and PPE were also examined by NPPTL to determine conformity to NFPA voluntary consensus standards (see Appendix III). Note: All evaluation reports will be added to this report when available.

Photo 1. Victim's facepiece showing thermal degradation.
(NIOSH Photo.)
Structure
The fire originated in the lobby of a movie theatre constructed in 1948. The theatre was of Type III construction and contained masonry block walls with a brick façade (A-side) and a bowstring roof truss system spanning over the auditorium (B-side to D-side) (see Photo 2 and Photo 3). The theatre measured approximately 50 feet by 100 feet, containing approximately 6,750 square feet (4,550 square feet above ground) (see Diagram 1). During this incident, the presence of the bowstring truss roof system was not identified by either of the departments.

Photo 2. A-side of the structure showing the front of the theatre.
(Photo courtesy of Mark D. Krueger.)

Photo 3. Photo taken from an aerial lift on the A-side of the structure showing the expansive area that the bowstring roof covered. Note the smoked dome outline, indicated by yellow arrows, on the far wall (C-side), indicating the location and span of the bowstring roof.
(Photo courtesy of state of WI.)
Access to the "attic" area was through the use of a straight ladder positioned at the rear of the movie screen. The theatre owner did not recall the size of wooden cords used to construct the bowstring roof, but he did state the construction was original and that he could walk on the rafters to change light bulbs. The theatre's lobby and auditorium contained a concrete floor. The concrete floor in the auditorium had a gradual downward slope from A-side to C-side.
In 1996, the theatre was purchased by the current owner and renovated. The auditorium was expanded to 220 seats, the movie screen was replaced with a 35-foot by 10-foot screen, side wall curtains were added, and a new ceiling (drop ceiling with tiles) was installed. The owner recalled that the new ceiling had been placed below the original ceiling (possibly 12 to 18 inches below). The new ceiling contained a total of six ceiling fans with lights (three lights suspended above each theatre aisle). Further details regarding the materials used to construct the new ceiling were not available to NIOSH investigators. The side wall curtains were placed over existing peg board and sound foam insulation (unprotected) that covered all exposed masonry walls within the viewing area (see Photo 4).
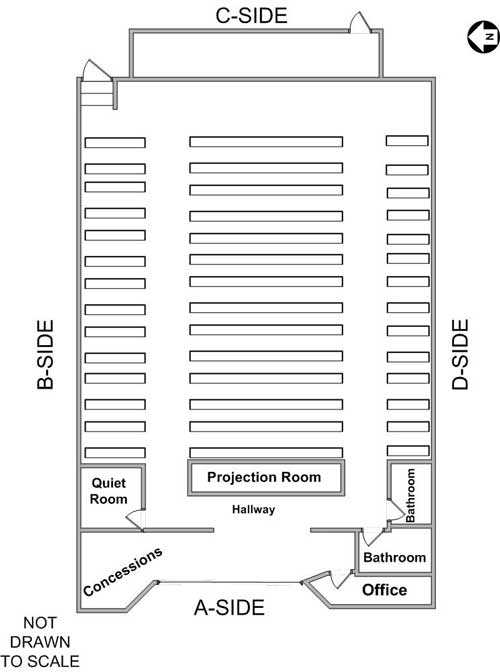
Diagram 1. Rendered floor plan of interior of theatre.

Photo 4. Interior auditorium walls, showing peg board, sound insulation, and wall curtains within the auditorium.
(Photo courtesy of Mark D. Krueger.)
In 2002, the theatre's rolled metal roof was damaged by a near-by tornado. The damaged roof was replaced with asphalt shingles. During 2007 – 2008, the theatre had a small electrical fire within the ceiling above the lobby area (minimal damage). The 1st due fire department had performed fire safety inspections of the theatre, but the theatre was never pre-planned.
Bowstring Truss Roof Construction
Bowstring truss roofs are easily identified by the roof's arched or curved outline (see Diagram 2). Bowstring truss roofs became popular in the 1930's. Prior to 1960, the bowstring truss roof design was one of the most common design types for large commercial and industrial structures. The bowstring truss roof was commonly used in facilities such as automobile dealerships and repair facilities, bowling alleys, grocery stores, and industrial complexes wherever large open floor spaces with limited interior supports were needed. The curved top chord members were made either by sawing straight lumber into curved shapes or laminating multiple smaller pieces bent over a jig to the desired shape. Bottom chord members were typically constructed with large, straight lumber members joined with either wood or metal bolted splice plates, located near mid-span, to achieve the required length. The top and bottom chord members were fastened together at the truss ends with U-shaped steel heels, or end shoes, bolted to both chord members.
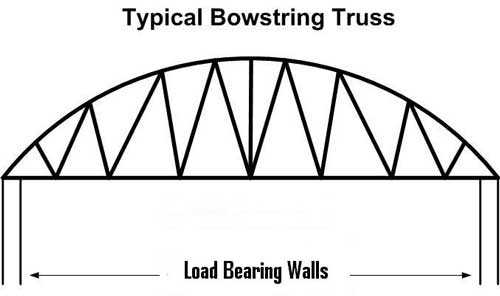
Diagram 2. Typical bowstring truss roof spanning between load bearing walls.
The principles of bowstring truss construction are similar to other types of truss construction in that web members are used to form multiple series of triangles that transfer tension from the bottom chord and compression from the top chord of the truss onto the load bearing walls. One big difference with the bowstring truss is that the compressional forces within the top chord act to force the load bearing walls outward as well as downward.
Bowstring truss roof systems may suffer from a little-known phenomenon related to inaccuracies in early industry-accepted truss design assumptions. One significant design deficiency involves the tensile strength of the bottom chord. Early truss designs assumed wood tensile strength could be defined by bending tests of small, straight-grained wood samples free of common wood defects. Prior to the 1960s, large-scale test facilities were uncommon, so full-size lumber tests were rarely conducted. During the 1960s, full-size lumber tests revealed that construction-grade lumber with natural imperfections (such as knots, checks and irregular grain) provides in-service tensile strength significantly less than that predicted by the earlier small-scale, clear wood tests. By 1968, lumber industry standards established a reduction factor of 0.55 to relate tensile strength to bending strength. Current building codes have increased this factor to 0.60, meaning the allowable tensile strength design values are only about 40 percent of those listed in the early codes. Thus, all trusses constructed prior to the late 1960s have a common code deficiency; the bottom chord members may have inadequate tensile strength to support code-prescribed roof loads.16
Weather
The incident occurred during a sunny, partly cloudy day with temperatures outside ranging in the 20s. This area of the state had seen varying amounts of snow the previous few months. NIOSH investigators could not determine the amount of snow and ice on the roof at the time of the incident, but photos taken by bystanders during the incident indicated there could have been several inches to potentially a foot or more of snow and ice remaining in the area (see Photo 5).

Photo 5. Photo taken from a field directly behind the C-side of the structure showing snow accumulations.
(Photo courtesy of Julie Miklaszewicz.)
Investigation
On March 4, 2012, at 1215 hours, an on-duty patrol officer (fire chief of victim's department) noticed heavy, black smoke in the sky within the town, followed by flames coming from the front of a theatre after turning down a side street. One of the theatre's owners had been at the theatre two hours before the fire had been discovered, and had turned on three thermostats and the popcorn butter machine in the lobby concessions area. Over the police radio channel, the patrol officer immediately notified dispatch of the incident's exact location before exiting his patrol car and evacuating the B/D-side exposures. He also requested dispatch to tone out his department since they were the next due fire department. He then returned to the A-side of the structure where he spoke with the theatre owners who confirmed no one was inside the structure. NIOSH investigators are unsure if this information was passed on to the initial arriving unit and/or officer in charge.
Activities of 1st Due Department Prior to Collapse
Prior to E1's arrival, the 2nd assistant chief's (initial officer in charge, or IC, for the 1st due fire department, although not identified over radio) initial action plan was to fight the fire defensively (not communicated to other personnel). Upon E1's arrival, personnel observed black smoke with heavy flames coming from under a canopy on the A-side of the structure. The 2nd assistant chief exited E1 and grabbed the 6-inch, large-diameter supply hose and walked it down to the hydrant, approximately 30 – 50 yards south of the fire building. After his SO brought him a fitting, he connected and charged the supply hose, not knowing it was still connected into the hose bed. After flowing water into the front of the theatre, E1, carrying 1,000 gallons of water, ran out of water (in about 2 – 5 minutes). He then shut down the hydrant and was assisted by the SO in breaking down the supply hose sections so that they could be drained and reconnected to E1. The SO also assisted with manning a hoseline on the A-side, removing debris from the lobby, and changing air bottles. The SO did not have a radio until after the collapse occurred.
While the 2nd assistant chief worked on the water supply, L1 arrived on scene with two personnel including the accountability officer (AO) followed by E5. The aerial operator briefly assisted the operator of E1 before he walked to the rear of the structure. He walked down the D-side of the theatre and observed no apparatus. The 2nd assistant chief then observed TE1 from the mutual aid department arriving on scene, so he advised them to go to the rear of the theatre. The 2nd assistant chief does not recall speaking with anyone operating on the C-side after their initial arrival on scene, except for when the patrol officer (victim's fire chief) was updating them about initial conditions. After the water supply was established for E1, the 2nd assistant chief walked back to the front of the fire building and observed two, two-man crews operating 1¾-inch hoselines defensively on the canopy and into the theatre's main entrance. The two hoselines were doing a good job of knocking down the heavy fire. He was then met by his fire chief who took over their command. They spoke briefly about current conditions and the 2nd assistant chief advised him that the mutual aid department was at the rear of the building. Note: The fire chief assumed that the mutual aid department would fight the fire from the rear. Throughout the incident, up to the point of the collapse, each department operated independently of the other with minimal face-to-face communication between the fire chief and the off-duty mutual aid chief (patrol officer). The fire chief and his aerial operator had a conversation about setting up the elevated master stream because fire was observed along the A-side roof line. The elevated master stream was going to be used in an attempt to stop the fire from progressing past the lobby (parapet wall) and into the theatre's auditorium. The 2nd assistant chief assisted in setting up the aerial ladder.
While the elevated master stream was being set up, one of the two-man hose-teams entered into the lobby of the theatre with a 1¾-inch hoseline. Although they had not been tasked with advancing the hoseline into the theatre, the two fire fighters on this hose crew stated to NIOSH investigators that they were shorthanded and "knew what had to be done" to extinguish the fire. They were able to make it to a hallway running between the B- and D-sides, which provided access to the left and right sides of seating within the auditorium. They decided to go left because they had observed an enclosed room with fire in it (believed to be a quiet room), but before they could get to it they were met by personnel from the victim's department (see Diagram 3). Note: This hose crew recalled hearing the mutual aid department dispatched for the incident, but they did not know that the victim and three other members from that department had entered the building. The two crews had a face-to-face conversation before the 1st due department turned around and went toward the other end of the hallway (bathrooms).
The fire chief, for the 1st due department, asked about accountability and the AO stated they would get into position. The 1st assistant chief, who had arrived on E5 and was originally working on disconnecting utilities on the C-side, had a face-to-face with the fire chief on A-side and advised him that the mutual aid department was operating on the C-side with positive-pressure-ventilation (PPV) fans and that he was having difficulty in securing the building's utilities. He stated to NIOSH investigators that he had a conversation with the victim's 1st and 2nd assistant chiefs regarding three of their personnel being in the theatre, accountability, and who was the mutual aid's officer in charge.
The fire chief remembered having conversations over the radio with dispatch regarding the utilities not being turned off. The fire chief decided to walk down the street, approximately 75 yards south of the fire building, to where one of the theatre owners worked, to verify who supplied their utilities. The amount of time taken to do this is unknown. He then returned to the A-side of the building to assist with aerial operations.
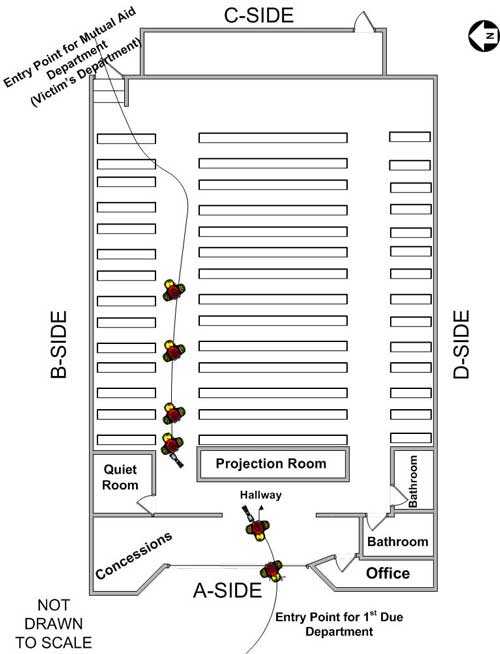
Diagram 3. Interior operations prior to collapse.
At the direction of the fire chief, the elevated master stream was initially operated manually from the ground and flowed water onto the canopy and the front side of the parapet wall. The elevated master stream was then blindly operated onto the theatre roof over the auditorium located behind the parapet wall. The fire chief then decided to send two fire fighters up the aerial ladder so that they could visually direct the master stream on any visible fire. He then turned aerial operations over to his aerial operator. After this, the fire chief walked over to the lobby area and observed one of his crews operating inside a hallway that led into the theatre's auditorium. The fire chief and his 2nd assistant chief then removed a large roof vent from the lobby area to give his hose crew additional space to work. Fire conditions were knocked down in this area, but moderate smoke was still emitting. The fire chief then took a moment to evaluate suppression activities on the A-side of the structure. The fire chief did not speak with the mutual aid department operating on the C-side of the structure and had not received updates from them either. Once the aerial crew was at the tip of the aerial ladder, they observed two separate burnt-through holes on the roof at the B- and D-side corners, directly behind the parapet wall, with fire emitting from both. This crew did not know the roof was bowstring roof construction. The B-side hole was approximately 4 feet in area and the D-side hole was approximately 2 feet in area. Due to the angle of their ladder and the height of the parapet wall, they could not direct the master stream directly into the holes and instead attempted to ricochet the water stream. The two fire fighters operating on the aerial ladder then decided to check the stability of the roof located behind the parapet wall by directing the elevated master stream all over the roof. This department's hose crew, which was operating in the area of the bathrooms, recalled debris falling on them from the drop ceiling and being able to see blue sky and water coming from outside. The aerial crew immediately observed the water turn into steam and felt the roof had been compromised. They immediately used the intercom system at the tip of the ladder to advise the aerial operator (on the ground) of their findings.
Activities of Mutual Aid Department (Victim's Department) Prior to Collapse
Upon arrival to the incident scene, the driver and 1st assistant mutual aid chief on TE1 observed the 1st due 2nd assistant chief standing in the roadway, directing them to the rear of the theatre. They turned down a side street just south of the D-side exposure before turning north to access the alley behind the theatre. The 1st assistant mutual aid chief observed black smoke rolling from the vents located on the C-side wall. These conditions were not communicated to the 1st due fire department operating on the A-side. Note: Initially, although not verbally stated but understood, the 1st assistant mutual aid chief was the officer in charge, or IC, for the mutual aid department. The 1st assistant mutual aid chief then advised E2 over their radio channel to lay in from the hydrant located just south of the theatre. E2 took the hydrant and the 2nd assistant mutual aid chief, riding as the officer, noticed that the fire appeared to be through the roof toward the A-side of the structure.
The 1st assistant mutual aid chief directed his driver/operator to open the door located on the C-side at the B/C corner. Black, gray smoke immediately rolled out the door. The 1st assistant mutual aid chief assisted E2 personnel in connecting the 5-inch supply line to TE1. FF1 pulled off a 2½-inch hoseline with a wye and took it to the opened door. He disconnected and replaced a 50-foot section of 2½-inch hose from the wye with 100 feet of 1¾-inch hoseline. Their fire chief (the on-duty patrol officer) met them at the rear and advised them to place two PPV fans at the open door and that the fire was located in the lobby area at the front of the theatre. Their fire chief (the on-duty patrol officer) then returned to the A-side of the structure to speak with the 1st due fire department personnel about the conditions at the rear.
The driver/operator of TE1, FF1, FF2, and the victim put on their PPE and SCBAs in preparation for advancing their 1¾-inch hoseline into the theatre from the C-side. According to the 1st assistant mutual aid chief, the reason their department had entered into the theatre from the rear (the unaffected side) was to stop any fire from coming further into the theatre. The 1st assistant mutual aid chief assumed that the 1st due department knew they were entering the building even though they had not communicated this to the 1st due department's officer in charge. The 1st assistant mutual aid chief then passed his command to the 2nd assistant mutual aid chief who had arrived on E2. The 1st assistant mutual aid chief was going to be the back-up for the four personnel he was sending into the building. The 2nd assistant mutual aid chief had been monitoring both fire department channels and stated to NIOSH investigators that he never heard any communications from the 1st due fire department.
The mutual aid interior four-man crew (driver/operator of TE1, victim, FF1, and FF2) entered the theatre advancing a 1¾-inch hoseline and carrying their individual radios in their coat pockets, but left their department's thermal imaging camera in the apparatus. After entering the theatre, the crew walked down 4 or 5 steps before reaching the floor of the auditorium. The interior crew noted how this area only contained whitish, gray smoke, thinking the PPV fans were working. They advanced the hoseline up the B-side aisle, noticing fire toward the front of the auditorium at the A/B corner. When they got to the rear of the auditorium, they noticed fire within a glassed-in room, possibly a "quiet room." They removed some wall curtains and broke out the glass before spraying water into this room. The fire had reached up into the ceiling of this room, but the room contents were quickly knocked down. Note: At this time, the 1st due aerial ladder crew observed fire through the roof in this area.
The mutual aid four-man crew noticed a hallway to the left of this room leading out to the lobby and advanced their hoseline a few feet down this hallway before they were met by a two-man hose crew from the 1st due department (see Diagram 3). The 1st due department crew then went back into the lobby area while the mutual aid crew stayed in this hallway, spraying water back and forth between the hallway ceiling and quiet room. They were also having a discussion about going to get pike poles to pull the ceiling in the quiet room when they were hit with water from the elevated master stream. At the same time, the 1st assistant mutual aid chief had just placed a ground ladder at the B/C corner when the elevated master stream struck him and also knocked masonry blocks off the parapet wall, striking a fire fighter in the head, who was wearing his helmet, and landing on the 2nd assistant mutual aid chief's foot, breaking it. It was then that the 1st assistant mutual aid chief realized that the "roof wasn't flat but rather arched."
The victim and driver/operator of TE1 decided to follow the hoseline out to get pike poles and talk to someone about getting the elevated master stream turned off. They both exited the building through the C-side. The victim waited at the doorway while the driver/operator of TE1 went to change his air bottle. They spoke to the 1st and 2nd assistant mutual aid chiefs about conditions, the need for pike poles, and turning off the elevated master stream. The 1st assistant mutual aid chief stated that he retrieved a pike pole for the victim but the victim had re-entered the building before getting the pole. While waiting next to the quiet room, FF1 and FF2 stated that the victim returned to them fairly quickly but without any pike poles. The victim pulled his radio from his coat pocket and had a discussion with FF1 and FF2 just before the roof collapse.
Collapse from 1st Due Department's Vantage Point
During this time, the fire chief had decided to walk down the D-side of the theatre because he had an "unsure" feeling about the fire. After walking a few yards down the D-side wall, he decided to evacuate the building. He called for an evacuation three times over his department's radio channel while he returned to the A-side of the building. The mutual aid department had the 1st due department's radio channel for fireground operations, but they did not remember hearing any radio transmissions to evacuate the building. Most of the mutual aid department's radios were on their main fireground channel and scanning additional channels. The aerial ladder crew, still spraying the master stream on the roof, watched the two holes get larger until the B-side and D-side holes met at the center of the roof line. The aerial crew then observed the roof collapse inward into the auditorium from the parapet wall all the way to the C-side exterior wall. Their interior hose crew was separated near the bathrooms from debris falling during the collapse. Also, the aerial crew recalled hearing an air horn sound from the C-side of the theatre. After reaching the A-side, the fire chief recalled heavy, gray smoke rising from the auditorium area, but the lobby area was free of fire and smoke. The fire chief immediately notified dispatch of the collapse and requested additional fire and EMS units to the scene. The fire chief overheard many of his fire fighters say that the building was clear, but he was stopped by his 1st assistant chief who advised him that the victim's department was still inside at the time of the collapse. The E1 pump operator recalled hearing the following radio transmissions over their fireground channel "…evacuate building…everyone is out of building…no the mutual aid department's fire fighters are still inside…well get them out." The fire chief then walked into the theatre's lobby and observed the roof down in the auditorium with fire burning in different areas. He rushed from the lobby over to his aerial ladder and advised his crew on the ladder to direct the master stream on the spot fires within the auditorium. The 1st due department's interior hose crew was able to self-extricate after the collapse by following their hoseline out. No Mayday was called by the 1st due department, but their interior hose crew did attempt to transmit over the radio while still inside (lots of radio transmissions). The 1st assistant chief ordered the AO to the C-side to take accountability for the mutual aid department. The mutual aid department advised the AO that they would handle accountability on C-side so that the AO could return to the A-side for search and rescue. When the AO returned they advised the fire chief and aerial operator that they were having trouble keeping up with accountability because responders were rushing into the theatre to help. The aerial operator then advised the fire chief to stay outside the building and pull everyone out of the theatre so that they could get a handle on accountability. The fire chief then advised the aerial operator that he needed more manpower to assist in getting the trapped fire fighters out before focusing on accountability. The fire chief advised NIOSH investigators that he never spoke to any personnel from the mutual aid department immediately following the collapse, but felt he had a good idea of where the trapped fire fighters were.
Collapse from Mutual Aid Department's Vantage Point
While standing near the quiet room, FF1 and FF2 stated they heard a weird noise followed by ceiling tiles falling on them. FF1, FF2, and the victim decided that they needed to leave immediately. They followed the hoseline leading out to the C-side door. The victim was first, followed by FF2 and then FF1. They traveled approximately 10 – 15 feet before the roof began to collapse in on them. FF1 saw the roof collapsing behind him so he dove into the B-side aisle, while FF2 was struck by roof debris that pushed him down into the aisle. FF1 and FF2 did not know where the victim was, but FF1 could reach out and touch FF2's boot. The patrol officer (victim's fire chief) had just come back to the C-side of the theatre and was having a conversation with his 1st assistant chief about the elevated master stream being used on the roof and that they should be getting interior fire fighters (from mutual aid department) out of the structure to evaluate conditions, when the roof collapsed. Fire fighters from the mutual aid department (still operating on C-side) recalled seeing heavy, black smoke pushed out the C-side door, which their interior crew had entered. They were unaware that the roof had collapsed until after the 1st assistant mutual aid chief looked through the door and could not see anything. He immediately went on air and followed the hoseline in. The patrol officer immediately went to ER1 and E2 and had personnel sound the sirens and air horns. At this time, information regarding the collapse was transmitted over the radio channel.
Following the collapse, FF1 and FF2 recalled being in a couple inches of water and the elevated master stream was still flowing water into the building and hitting them at times. The 1st assistant mutual aid chief stated he was in waist-deep water after he entered the building and walked down the stairs into the theatre's auditorium. FF1 and FF2 also remember fire burning around and on top of them. FF1 and FF2 also heard the victim still on air say, "Let's go guys, come on, get us out." No other verbal communications from the victim were heard following the activation of a PASS device. Moments later, FF1's low-air alarm began to sound from his SCBA, followed by his PASS device. When he ran out of air, he kept his facepiece on but removed his mask-mounted-regulator. At about the same time, the 1st assistant mutual aid chief was inside the building but could not get very far up the B-side aisle due to the collapse debris. He stated he heard what he thought was a PASS device alarm, but he was not sure due to the noise of the PPV fans running and the elevated master stream flowing water into the building. He then exited the building to hear their air horn sounding (Mayday call) and the patrol officer (their fire chief) asking for accountability in person.
The driver/operator of TE1 called FF1, FF2, and the victim on their radio channel without any response. The fire fighters from the mutual aid department stated they never heard any radio transmissions from the 1st due department regarding an evacuation, collapse, or rescue operations. Following his transmission attempts, the driver/operator of TE1 re-entered the building, following the hoseline, with another fire fighter and a second 1¾-inch hoseline to see if they could get further into the collapse area. They were unsuccessful in getting any further than the 1st assistant chief had earlier, but they were able to confirm the sound of a PASS device alarm.
Search, Rescue, and Recovery Operations
Additional attempts were made by both departments to enter into the theatre from the A- and C-sides. Entry through the A-side provided fire personnel the best means to access the auditorium. Note: The roof had collapsed (pancaked) onto the center rows of seating. Additional mutual aid personnel arrived to assist with search and rescue operations, as well. The 1st due fire chief stated to NIOSH investigators that he positioned himself, with his 2nd assistant chief, within the hallway leading into the auditorium. He stated he remembered many fire fighters from his and the mutual aid departments coming and going through the hallway as they searched in the auditorium through debris and water, knee to waist deep in areas. Many fire fighters stated to NIOSH investigators that there was no coordinated search and rescue effort and that the search area was extremely loud from the PPV fans and master stream flowing water. While fire fighters were searching within the debris, FF2, who had completely removed his SCBA pack, was able to remove some roof debris from around him and pull himself up to alert fire fighters. Two fire fighters quickly noticed him and assisted him out of the debris. Just before being removed, he stated he was laying in 10 inches of water. FF2 was then assisted out of the theatre by the 1st due fire department's fire chief and his 2nd assistant chief. Once out, FF2 remembered that the noise in the collapse area was extremely loud from the elevated master stream flowing water and the PPV fans blowing from the lobby area and rear of the building.
FF1 was then located, removed from debris and assisted out the A-side to an EMS unit waiting outside. The 1st due fire chief recalled hearing that all fire fighters had been accounted for, so the fire chief walked over to speak with EMS personnel who advised him they had only received two fire fighters who had been trapped in the collapse. The fire chief then had personnel continue search and rescue operations for the victim.
The 1st due fire chief remained within the theatre's hallway as fire personnel searched throughout the auditorium area, focusing on the B-side aisle way. The 1st due fire chief recalled someone retrieving a thermal imaging camera to assist with finding the victim. After removing a piece of debris from the B-side aisle, a fire fighter discovered a single fire fighting glove floating in approximately 3 feet of water. Personnel within the auditorium began to focus on searching this area for the victim (see Photo 6). They were able to find the victim face down after seeing a helmet and an SCBA bottle within the water. A fire fighter was able to stand in the water, get under the victim, and lift up the victim's upper torso. This fire fighter checked for a pulse and confirmed that the victim was deceased. Fire fighters remarked that the SCBA back frame had been damaged and the SCBA bottle was only attached to the air line. The SCBA bottle was disconnected to assist in freeing the victim who was partially trapped by what appeared to be piping from a boiler system. The fire fighter holding the victim stated to NIOSH investigators that the victim was still wearing his helmet, with chin strap attached, protective hood, and facepiece, with mask-mounted-regulator attached, properly positioned about his face. This fire fighter noted that the victim's facepiece was sunken in on the left side, but still appeared intact. After additional personnel assisted in removing debris from around the victim, the victim was removed from the water and placed in a stokes basket.

Photo 6. Victim discovered in this general area.
(Photo courtesy of 1st due department.)
Fire Origin/Cause and Behavior
State and federal fire/arson investigators investigated the origin and cause of the fire. These investigators determined that the fire was accidental and originated in the lobby area of the theatre.
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that led to the fatality and injuries:
- Initial arriving units not establishing/performing/implementing an incident management system, an overall incident commander, an incident action plan (IAP), and a 360-degree situational size-up
- Risk management principles not effectively used
- Fireground and suppression activities not coordinated
- Fire ground communications between departments not established
- Incident safety officer (ISO) role ineffective
- Rapid intervention crew (RIC) procedures not followed and/or implemented
- Bowstring roof truss construction not recognized by departments
- Fire burned undetected within the roof void space for unknown period of time
- Uncoordinated master stream operations
- Location of victim following roof collapse not immediately known.
Cause of Death and Injuries
According to the death certificate, the medical examiner listed the victim's cause of death as due to smoke inhalation and thermal injuries. Injuries incurred by other personnel on scene included a fractured foot, knee contusion, nonspecific ankle injury, nonspecific head injury, nonspecific knee injury, lung inflammation from fighting fire, and smoke inhalation.
Recommendations
Recommendation #1: Fire departments should ensure that an effective incident management system is established with a designated incident commander not involved with fire suppression activities.
Discussion: Most incidents are considered routine and involve a small commitment of resources (high-frequency/low-risk), while few incidents involve large commitments of resources, complex situations, and are low-frequency/high-risk events. An incident management system is intended to provide a standard approach to the management of emergency incidents. The National Fire Protection Association (NFPA) 1500 Standard on Fire Department Occupational Safety and Health Program4 and NFPA 1561 Standard on Emergency Services Incident Management System17 both state an incident management system shall be utilized at all emergency incidents. Most often, this system is commonly known as, or referred to as, the Incident Command System, or ICS. The many different and complex situations encountered by fire fighters require a considerable amount of judgment in the application of ICS. The primary objective is always to manage the incident. The incident commander (IC) should be able to apply ICS in a manner that supports effective and efficient management of the incident. The use of ICS should not create additional challenges for the IC, but rather provide a systems approach to ensuring a successful outcome of the incident.17
NFPA 1561, Chapter 3.3.29 defines an incident management system as "A system that defines the roles and responsibilities to be assumed by responders and the standard operating procedures to be used in the management and direction of emergency incidents and other functions."17 Chapter 4.1 states "The incident management system shall provide structure and coordination to the management of emergency incident operations to provide for the safety and health of emergency services organization responders and other persons involved in those activities." 17 Chapter 4.2 states "The incident management system shall integrate risk management into the regular functions of incident command."17
The incident management system covers more than just fireground operations. The incident management system must ensure for command/control and fire fighter safety, which includes situational evaluation, strategy and the incident action plan, personnel accountability, risk assessment and continuous evaluation, communications, rapid intervention crews (RIC), roles and responsibilities of the incident safety officer (ISO), and interoperability between multiple agencies (mutual aid departments, law enforcement, emergency medical services, state and federal government agencies and officials, etc.) and surrounding jurisdictions (automatic aid or mutual aid responders).
One of the most critical components of this system is the development and implementation of an incident action plan (IAP).17 For the fire service, the majority of times the IAP is communicated verbally. The IAP is based on the resources immediately available and those responding. The goal is determined in accordance with the incident priority from which a strategy must emerge; tactical objectives, aimed at meeting the strategy, are determined and specific assignments made. A personnel accountability system should be established as assignments are made. The important point is that the overall IC communicates the IAP to tactical- and task-level supervisors.
During this incident, the assumption of overall command was not declared over the radio to other fire fighters upon arrival. The mutual aid department was directed to the rear of the theatre without knowing fire conditions or an incident action plan for mutual operational strategy, tactics, and communications. Also, the 1st due department chief officers, who served as their ICs, were involved with fireground activities, such as water supply, securing utilities, and search and rescue, which significantly reduced their ability to function as an IC.
Recommendation #2: Fire departments should ensure that a complete situational size-up is conducted on all structure fires.
Discussion: Among the most important duties of the first officer on the scene is conducting an initial 360-degree situational size-up of the incident and transmitting this information to units on the fireground or responding to the incident. In order to accomplish this, the first officer on scene needs to have the requisite knowledge of the elements of a proper size-up.8 A proper size-up begins from the moment the alarm is received, and it continues until the fire is brought under control either offensively or defensively. The size-up should include an evaluation of factors such as the following:
- Location and volume of the fire
- Required fire flow
- Building construction
- Commercial versus residential structure
- Water supply
- Length of time the fire has been burning, recognizing burn time may have affected structural stability
- Conditions on arrival
- Occupancy
- Fuel load
- Presence of combustible or hazardous materials
- Exposures
- Roof and wall loads
- Time of day
- Available staffing on scene or en route
- Weather conditions
- A realistic evaluation of the ability to conduct an offensive attack with available resources.18-19
Even before ICs take command of an incident, they will be faced with having to determine which critical tasks must be performed (simultaneously or as required) to bring the incident under control, and whether they can delegate these tasks before becoming overwhelmed. ICs may need to consider assigning an individual to be an aide or operations sector leader so that critical tasks can be delegated, carried through, and effectively supervised. ICs will use current knowledge and previous experience to formulate a plan for arriving apparatus and personnel. When the IC arrives, as much information as possible must be ascertained to determine whether the IAP will still work. The IC may be faced with several priorities, such as an entrapped civilian, an incident of a scale larger than previously determined, and the fire environment itself. This is additionally part of the initial situational size-up, which will constantly change as the incident progresses until it is brought under control. ICs should be willing to prioritize and change their strategy and plan based on these assessments. Most importantly, the initial size-up provides a starting point for all fireground operations.
During this incident, the two departments on scene established their own fire suppression operations from opposing sides. Their officers in charge did not walk around the structure or communicate with each other on conditions that were encountered. Also, the bowstring truss roof construction and the hazards associated with that type of roof were never identified by personnel on scene.
Fire departments should be aware of the 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.20 These guidelines recommend that ICs conduct or obtain a 360-degree situational incident size-up, determine the occupant survival profile, and conduct an initial risk assessment.
Recommendation #3: Fire departments should use risk management principles at all structure fires.
Discussion: While it is recognized that fire fighting is an inherently hazardous occupation, risk management principles established by the fire service are based on the philosophy that greater risks will be assumed when there are lives to be saved and the level of acceptable risk to fire fighters is much lower when only property is at stake. Interior offensive fire fighting operations can increase the risk of traumatic injury and death to fire fighters from structural collapse, burns, and asphyxiation. In this incident, it was made clear by the theatre owner that no civilians were in the buildings. When it is confirmed that there is no risk, the IC must then decide what risks they are willing to place their personnel in based on risk-versus-gain.
Established risk management principles suggest that more caution should be exercised in abandoned, vacant, and unoccupied structures and in situations where there is no clear evidence indicating that people are trapped inside a structure and can be saved.18 The IC, with input from the assigned ISO and/or division/group supervisors, is responsible for evaluating conditions at a structure fire and determining safe tactics for fighting the fire. To accomplish this, the IC should use a standardized strategic decision-making model. First, the IC should size up the critical fireground factors. 19 Before ordering an offensive attack, the IC must make a determination that offensive (interior) operations may be conducted without exceeding a reasonable degree of risk to fire fighters and must be prepared to discontinue the offensive attack if the risk evaluation changes during the fire fighting operation. A full range of factors must be considered in making the risk evaluation, including (but not limited to) the following:
- Presence of occupants in the building
- A realistic evaluation of occupant survivability and rescue potential
- Size, construction, and use of the building
- Age and condition of the building
- Nature and value of building contents
- Location and extent of the fire within the building
- Adjacent exposures (structures)
- Fire involvement or compromise of the building’s structural components
- Residential or commercial structure
- Delayed discovery/reporting and its effect on burn time and structural stability
- Considerations of fire loading and fire behavior
- A realistic evaluation of the ability to execute a successful offensive fire attack with the resources that are available.18-19
These fireground factors must be weighed against the risk management plan. Fire fighters are routinely exposed to certain known and predictable risks while conducting operations that are directed toward saving property. The IC is responsible for recognizing and evaluating those risks and determining whether the level of risk is acceptable or unacceptable. However, risks taken to save property should always be less than those to save lives.18, 21 Risks to fire fighters versus gains in saving lives and property must always be considered when deciding whether to use an offensive or defensive attack. The IC should routinely evaluate and re-evaluate conditions and radio progress reports in reaching objectives to dispatch and on scene fire fighters. This process allows the IC to determine whether to continue or revise the strategy and attack plans. Failure to revise an inappropriate or outdated attack strategy is likely to result in an elevated risk of death or injury to fire fighters.4, 19 NFPA 1500, section 4.2, provides detailed information regarding the risk management plan.4
Incident demands on the modern fireground, unlike those of the past, require ICs and commanding officers to have increased technical knowledge of building construction with a heightened sensitivity to fire behavior, a focus on operational structural stability, and considerations related to occupancy risk versus the occupancy type. Strategies and tactics must be based on occupancy risk, not occupancy type, and must orchestrate sufficient staffing, fire flow, and tactical patience in a manner that identifies with the fire profiling and the predictability of the occupancy profile and accounts for presumptive fire behavior.22 The first arriving officer, as well as the IC, must make an informed judgment (before and ongoing) as to what is at risk – people or property. This judgment will determine the risk profile for the incident. Many fire fighters stand by the notion that all incidents are "people" events until proven otherwise. Historically, the fire service has a poor history of changing risk-taking strategies based upon the people/property issue.23
During this incident, there was no clearly defined IC to make decisions on risk management and as a result an offensive or defensive strategy(s)/tactic(s) was not communicated. Communications were not established between the two departments and each department had a different view of fire and smoke conditions. The observation of the burned through holes on the roof by the fire fighters on the elevated master stream should have prompted an immediate removal of all interior fire fighters and a defensive operation. It should be noted that the patrol officer (mutual aid fire chief) confirmed that the theatre was empty and had evacuated the fire building exposures prior to units arriving. This type of information needs to be passed on to all units and/or departments responding to the incident, and a decision needs to be made on whether an offensive or defensive strategy will be used.
Recommendation #4: Fire departments should work together to develop mutual aid standard operating procedures for fireground operations that support interagency operability and accountability and train on those procedures.
Discussion: Mutual aid companies should train together and not wait until an incident occurs to attempt to integrate the participating departments into a functional team. Differences in equipment and procedures need to be identified and resolved before an emergency occurs when lives may be at stake. Fire departments responding to mutual aid incidents must ensure that interior and exterior fireground operations are effectively coordinated and communicated to each other such as ventilation tactics and use of elevated master streams. As the incident escalates, additional staffing and resources may be needed, adding to the burden of tracking personnel. At this point, an accountability system should be in place, including an incident command board that is established and maintained by an assigned accountability officer or aide. A properly maintained incident command board allows the IC to readily identify the location and time of all fire fighters on the fireground. As a fire escalates and additional fire companies respond, a chief's aide or accountability officer assists the IC with accounting for all fire fighting companies at the fire, at the staging area, and at the rehabilitation area. The personnel accountability report (PAR) is an organized on-scene roll call in which each supervisor reports the status of his crew when requested by the IC or emergency dispatcher.4, 24 The use of a functional accountability system, as recommended by NFPA 1500 4 and NFPA 156117 requires the following:
- Development of a departmental SOP
- Training all personnel
- Strict enforcement during emergency incidents
On every response, a properly initiated and enforced accountability system that is consistently integrated into fireground command and control enhances fire fighter safety and survival by helping to ensure a more timely and successful identification and rescue of a disoriented or downed fire fighter. Procedures and protocols that are jointly developed and have the support of the majority of participating departments will greatly enhance overall safety and efficiency on the fireground. Once methods and procedures are agreed upon, training protocols must be developed and joint training sessions conducted to relay appropriate information to all affected department members.
During this incident, each department had varying levels of information contained within their individual department guidelines. These two departments had signed a county-wide mutual aid agreement, but no SOPs or SOGs had been established between them to assist interoperability while working together. These two departments used different accountability systems and SCBA packs. Also the departments had not trained together to get an idea of how they would function during a fire incident, especially during a Mayday situation. Fire departments that respond regularly on mutual aid or on automatic mutual aid should develop common operating policies/procedures to include regular inter-fire department training, equipment operability, and communications.
Recommendation #5: Fire departments should ensure that the incident safety officer (ISO) position, independent from the incident commander, is appointed and effectively utilized at every structure fire meeting the requirements within NFPA 1521 Standard for Fire Department Safety Officer.
Discussion: According to NFPA 1561 Standard on Emergency Services Incident Management System,17 the incident commander shall have overall authority for management of the incident and the incident commander shall ensure that adequate safety measures are in place. This shall include overall responsibility for the safety and health of all personnel and for other persons operating within the incident management system. While the incident commander is in overall command at the scene, certain functions must be delegated to ensure adequate scene management is accomplished.17
According to NFPA 1500 Standard on Fire Department Occupational Safety and Health Program,4 as incidents escalate in size and complexity, the incident commander shall divide the incident into tactical-level management units and assign an incident safety officer (ISO) who has the expertise to evaluate hazards and provide direction with respect to the overall safety of personnel. These standards indicate that the incident commander is in overall command at the scene but acknowledge that oversight of all operations is difficult. Although, the presence of a safety officer does not diminish the responsibility of individual fire fighters and fire officers for their own safety and the safety of others, on-scene fire fighter health and safety is best preserved by delegating the function of safety and health oversight to the ISO.
NFPA 1521 Standard for Fire Department Safety Officer defines the role of the ISO at an incident scene and identifies duties such as recon of the fireground and reporting pertinent information back to the incident commander; ensuring the department's accountability system is in place and operational; monitoring radio transmissions and identifying barriers to effective communications; and ensuring established safety zones, collapse zones, hot zones, and other designated hazard areas are communicated to all members on scene.25 The ISO adds a higher level of attention and particular expertise in analyzing safety hazards, building construction, fire conditions, and in the particular uses and/or limitations of protective equipment, which will help fire fighters and fire officers.26 Larger fire departments may assign one or more full-time staff officers as safety officers who respond to working fires. In smaller departments, every officer should be prepared to function as the ISO when assigned by the incident commander. When the designated ISO is not immediately dispatched or available at the scene, the IC should appoint an ISO. Line officers should receive sufficient training to act as an ISO where needed, until the designated ISO arrives on scene. This will ensure the presence of an ISO on the fireground at all times. The ISO should be automatically included as part of the first alarm assignment for a reported structure fire and for additional incidents that the fire department sees necessary.
Additionally, the IC relies upon fire fighters and the ISO to relay feedback on fireground conditions in order to make timely, informed decisions regarding risk-versus-gain and offensive-versus-defensive operations. The safety of all personnel on the fireground is directly impacted by clear, concise, and timely communications among mutual aid fire departments, sector command, the ISO, and the incident commander.
During this incident, the SOs for both departments had never received any formal training on what is expected of them during an emergency incident. The 1st due department's SO was available at the theatre fire, but was occupied at times with fireground activities such as water supply and setting up fire suppression activities. During this incident, this SO was not able to focus his attention on the structure, fire conditions, and the safety and health of fire fighters operating on the scene.
Recommendation #6: Fire departments should ensure that a rapid intervention crew (RIC) is readily available, on scene, and prepared to respond to fire fighter emergencies.
Discussion: A RIC should be designated and available to respond before interior attack operations begin and throughout the duration of the incident. The team should report to the IC, conduct a size-up of the structure and incident, and maintain a position in a location that promotes rapid access to the structure if a Mayday is declared. When standing by, the RIC should monitor radio traffic and continuously size up the incident and not assist in regular fire fighting activities. NFPA 1500, section 8.8.7 states, "At least one dedicated RIC shall be standing by with equipment to provide for the rescue of members that are performing special operations or for members that are in positions that present an immediate danger of injury in the event of equipment failure or collapse."4 The RIC should have all tools necessary to complete the job (e.g., search and rescue ropes, combo Halligan bar and flat-head axe, first-aid kit, and resuscitation equipment).24 These teams can intervene quickly to rescue a fire fighter who is running out of breathing air, disoriented, lost in smoke-filled environments, trapped by fire, or involved in structural collapse.4 During this incident, there was no established RIC prior to the collapse within the sanctuary.
Fire departments should be aware of the 2010 International Association of Fire Chiefs' Rules of Engagement of Structural Firefighting. These guidelines recommend that ICs always have a rapid intervention team in place at all working fires.20 Also, NFPA 1407 Standard for Fire Service Rapid Intervention Crews provides basic training procedures for fire service personnel to conduct fire fighter rapid intervention operations.3
During this incident, the victim's department had established a RIC standard operating procedure but had not established a RIC during the incident or following the collapse. Following the collapse both departments sent personnel inside the theatre to look for the fire fighters who were trapped in an uncoordinated manner. Uncoordinated search and rescue efforts can actually impede the efforts to find missing fire fighters while also exposing the rescuers to potentially unsafe conditions.
Recommendation #7: Fire departments should conduct pre-incident planning inspections of buildings within their jurisdictions to facilitate development of safe fireground strategies and tactics.
Discussion: NFPA 1620 Standard for Pre-incident Planning states, "The purpose of this document shall be to develop pre-incident plans to assist responding personnel in effectively managing emergencies for the protection of occupants, responding personnel, property, and the environment." A pre-incident plan identifies deviations from normal operations and can be complex and formal or simply a notation about a particular problem, such as the presence of flammable liquids, explosive hazards, lack of hydrants, modifications to structural building components, or structural damage from a previous fire. 27-29
Building characteristics, including type (or more importantly risk) of construction, materials used, occupancy, fuel load, roof and floor design, and unusual or distinguishing characteristics should be recorded, shared with other departments who provide mutual aid, and, if possible, entered into the dispatcher's computer so that the information is readily available if an incident is reported at the noted address.29 These pre-incident plans can help determine safety hazards within or around a structure, length of response times, and locations of closest hydrants. Since many fire departments have tens/hundreds of thousands of structures within their jurisdiction, it is a challenge to establish an effective preplanning system. Priority should be given to those having elevated or unusual fire hazards, being a high-risk and low-frequency type incident, and life safety considerations.
Prior to this incident, the theatre had not been preplanned but had received several fire inspections by the 1st due department. However, no information regarding the building construction type had been documented, including the presence of a bowstring truss roof.
Recommendation #8: Fire departments should familiarize and continually train all personnel on all types of building construction, especially those containing bowstring roof trusses.
Discussion: Bowstring truss roofs are easily identified by the roof's arched or curved outline. This type of arched roof can span a large open area while being unsupported by pillars or posts with the lower chord of the truss being covered with a ceiling to form an enclosed cockloft or attic space.24 These concealed spaces can hide a fire in progress long enough for the fire to seriously weaken the truss system, causing a very dangerous situation for fire fighters working above or below the roof system.24 A fire department's familiarity with types of construction in their community is an important tool in safely fighting fires, and the use of a thermal imaging camera will better assist fire fighters in determining where fire is located. Every structure, commercial or residential, has its own unique situation, and fire departments cannot rely solely on the last fire incident they participated in to provide them with a plan that will work at the next incident. Proper training is an important aspect of safe fire ground operation. Both officers and fire fighters must be aware of different types of building construction and their associated hazards.30-32 For example, collapsing roof systems can exert pressure on supporting exterior walls, increasing the potential for wall collapse. Light-weight roof truss systems pose a greater risk of collapse when damaged and/or exposed to fire. Different roof systems may collapse at different rates.32 While heavy timber roof systems will withstand more degradation by fire than lightweight engineered roof trusses, both types are subject to failure.24 Different phases of the fire suppression activities, such as the initial, offensive, and defensive attacks and overhaul will have different hazards. However, the potential for collapse exists in any fire-damaged structure.32
This building construction knowledge begins with an initial fire fighter recruit school or other types of training module(s). Knowledge of building construction progresses with additional training and experience gained through on-the-job training and/or individual walk-through/preplan activity during and after construction. One source of information on the hazards of structural collapse is the Building and Fire Research Laboratory of the National Institute of Standards and Technology (NIST). A DVD containing videos and reports on structural collapse can be obtained from the NIST Web site (http://www.nist.gov/el/).33 (Link Updated 1/29/2013) NFPA 220 Standard on Types of Building Construction has specific information on all building construction and types and could be used to design and develop training curriculum for building construction.34
Fire departments must ensure that fire fighters, officers, and incident commanders have a sound knowledge base and experience that they can apply to any incident, allowing them to adjust it to meet the changes of the incident at hand. These departments had limited documented training and no operating procedures for different types of building construction and safety factors associated with each building type.
During this incident, the fire fighters and officers who were interviewed by NIOSH investigators were unaware of what a bowstring truss roof was and that the theatre's roof was constructed that way.
Recommendation #9: Fire departments should train all personnel to identify the risks and hazards associated with supporting/loaded structural components degraded by fire, use of a thermal imaging camera, and realize the potential for a structural collapse exists at all times.
Discussion: During fire operations, two rules exist about structural collapse: (1) the potential for structural failure always exists during and after a fire, and (2) a collapse danger zone must be established.26, 27, 30, 35 Buildings or structures within a building can collapse due to the structural damage directly caused by a fire or the activities of fire fighting operations (e.g., pulling ceilings, roof ventilation, and water application). This is especially true in lightweight-type construction. Other factors may include roof loads, fuel loads, damage, renovation work, pre-existing deterioration, water load, support systems, and truss construction.31, 36, 37 A collapse is a possibility after fire involvement of more than 10 minutes, but fire departments should not rely solely on time as a collapse predictor.37
If fire is not venting through the roof, interior fire suppression crews if assigned, and based upon conditions, must act quickly in exposing concealed spaces such as walls, soffits, and drop ceilings, so that the seat of a fire and its spread can be quickly contained and extinguished through coordinated water application. Opening up concealed spaces will also provide interior fire suppression crews a good view of structural/support components in order to assess any damage or instability. This assessment will assist the fire department in making a decision to manage the fire offensively or defensively, to designate an incident safety officer, and whether or not to establish a collapse zone. Exterior fire personnel such as the ISO, ventilation crews, or the IC should be evaluating a structure for potential collapse as well. They should be observing visible fire and wind conditions, dead loads on roofs (e.g., air handling units or steeples), and visible instability of exterior load-bearing walls. Thermal imaging cameras can assist fire fighters in quickly getting crucial information about the location of the seat of the fire from the interior and exterior of the structure, which can help the incident commander plan an effective and rapid response. Knowing the location of the most dangerous and hottest part of the fire may help fire fighters determine a safer approach and avoid exposure to structural damage in a building that might have otherwise been undetectable. Whether interior or exterior, all observations need to be immediately passed on to the IC, so that a decision can be made to continue the current fire attack strategy or make a change.
Fire departments cannot rely on the structure to not collapse. Fire departments should constantly be evaluating their fireground strategy and tactics and observing potential indicators of collapse (e.g., time exposed to fire, construction type, noises, and cracks). Maintaining situational awareness at all times during a fire incident is paramount. Situational awareness is a highly critical aspect of human decision making: understanding what is happening around you, projecting future events, comprehending information and its relevance, being realistic, and an individual's perception.38 Fire fighters, officers, and incident commanders must be able to make critical decisions based on their knowledge, experience, and observations so that fire fighter health and safety is achieved.
During this incident, fire fighters who were operating inside the theatre stated to NIOSH investigators that they had no idea that the fire was burning above them in the roof trusses. The need to apply an elevated master stream onto the roof of this structure should have prompted the IC to evacuate all interior fire-fighting personnel prior to taking this type of defensive action. The fire fighters operating from the tip of the aerial ladder observed fire that had burned through the bowstring truss roof and attempted to direct the master stream into those areas while fire fighters were still inside. This type of information needs to be communicated immediately to the IC because this is an indication that the roof is structurally compromised. Added water weight from an elevated master increases the structure's instability and collapse potential. Indicators of impending collapse need to be communicated to all personnel at a fire scene immediately so that appropriate steps can be taken to evacuate a structure and make sure collapse zones have been appropriately established. When a decision is made to use an elevated master stream for suppression, steps need to be taken to ensure that fire fighter safety is maintained at all times.
Recommendation #10: Fire departments should train on and understand the use and operation of elevated master streams and its effects on structural degradation.
Discussion: Master streams are an effective tool for fire suppression operations. Master streams can deliver a large volume of water over a distance while reducing the direct exposure of fire fighters to the fire. Master stream operations can also accelerate structural degradation and can increase the risk of a building collapse.24, 39-40 When multiple master streams are flowing water onto a building, the additional weight of the water can rapidly increase the potential for structural collapse. Water weighs 8.33 pounds per gallon. A master stream flowing 1,000 gallons per minute can add an additional 8,330 pounds per minute that the structure, already deteriorated by fire, must support. In 30 minutes, the additional weight contributed by this master stream could add 249,900 pounds or 125 tons of additional weight to the structure.35 Direct impingement of the master stream at close range can also directly contribute to structural degradation by dislodging bricks, breaking windows and other building components. Master streams can also push fire throughout the interior of a structure, leading to fire spread.
Another important indicator that fire fighters and officers should look for is the presence or lack of runoff during master stream operations. If multiple outside streams are being applied to a structure and there is little or no water runoff, the water must be accumulating somewhere.39 As noted above, the additional weight added by standing water on roofs or floors can significantly contribute to the risk of structural collapse. Fire fighters and fire officers need to understand this fact and take this into consideration as part of the incident action plan. If a collapse zone has not already been established, then one should be established as quickly as possible. Fire fighters should not be allowed to enter the collapse zone without the direct permission of the incident commander.41
During this incident, the elevated master stream was initially manually operating from the ground and directed blindly over the bowstring truss roof. Interior fire fighters complained about the master stream coming into the building (through the roof) prior to the collapse and following the collapse. Fire fighters were also injured at the rear of the structure when cinder blocks were knocked off the roof by the master stream. Elevated master streams should never be operated directly onto fire fighters and care should be taken to also evaluate the amount of water added to a roof that has been structurally degraded by fire.
Recommendation #11: Fire departments and dispatch centers should ensure that emergency traffic over a radio, such as a Mayday, is effectively monitored, receiving the highest priority during an incident.
Discussion: NFPA 1221 Standard for the Installation, Maintenance, and Use of Emergency Services Communications Systems recommends the communication center have the ability to monitor tactical fireground radio traffic.42 Fireground communications can become very hectic and confusing when a fire fighter is in distress, becomes lost, or is trapped. Fire departments and dispatch centers must be able to effectively monitor radio transmissions (e.g., Maydays) while on the fireground and within a dispatch center. A Mayday procedure can outline the fireground response plan and duties of fire fighters, officers, the dispatch center, and the IC. This can include establishing separate radio channels for fireground operations, search and rescue operations, and/or water supply. This will help reduce any confusion during the Mayday.
The term "Mayday" is the international distress signal. Fire fighters must act promptly when they become lost, disoriented, injured, low on air, or trapped.43-48 They should announce, “Mayday-Mayday-Mayday” over the radio and manually activate their PASS device. A transmission of the Mayday situation should be followed by the last known location of the fire fighter and, if able, the individual’s identifier (e.g., E3 pump). A crew member who suspects a fire fighter(s) is in trouble or missing should quickly try to communicate with the fire fighter(s) via radio and, if unsuccessful, initiate a Mayday providing relevant information.
An emergency radio transmission reporting a "Mayday" is the highest priority transmission that may occur at any incident and should receive precedence from dispatch, the IC, and other units operating at the incident. When this emergency traffic is initiated, all other radio traffic should stop to clear the channel and allow the message to be heard. Mayday transmissions must always be acknowledged and immediate action taken. The IC must either personally handle the situation or designate another officer to do so. Part of handling a Mayday is to communicate with the fire fighter(s) in distress and with any other fire fighters or officers involved. The sooner the IC is notified and a RIC is activated, the greater the chance of the fire fighter being rescued. If there is any question that a Mayday may have been transmitted and heard by someone (not all), priority should be given in verifying if it were a Mayday transmission. The IC should be made aware of this immediately, so that he can attempt to contact the individual who potentially transmitted the Mayday or contact dispatch to verify the transmission. A possible Mayday transmission should never be overlooked.
These fire departments had not established a Mayday procedure that could be used as a training guide for fire personnel and guidance for dispatchers. Once a procedure is in place, the challenge for fire departments is providing realistic, safe training that accurately simulates fire conditions. It is absolutely necessary that the Mayday training place fire fighters in positions that closely simulate an actual fire to realistically exercise one's Mayday skills.48
Fire departments should be aware of the 2010 International Association of Fire Chiefs' (IAFC) Rules of Engagement (ROE) of Structural Firefighting.20 These guidelines recommend that fire fighters constantly monitor fireground communications for critical radio reports and declare a Mayday as soon as they are in danger. Although not addressed by the IAFC ROE, ICs and dispatch centers should also be constantly monitoring fireground communications for critical radio reports. The value of a dispatch center monitoring fireground channels cannot be understated. Quite often, due to normal fire ground activities, it is possible for the IC to miss a critical radio transmission. The dispatch center, in a different environment than the fireground, with a dispatcher dedicated to the incident, may be able to hear that transmission, potentially making a measurable difference in the outcome of the incident.
Also, the IAFF Fire Ground Survival program (which is available to all fire departments) was developed to ensure that training for Mayday prevention and Mayday operations is consistent between all fire fighters, company officers, and chief officers.48
During this incident, neither department had established May Day procedures within their departments or with respective emergency dispatch centers. Emergency buttons on hand-held radios were not programmed to alert or notify someone of an emergency or downed fire fighter. Following the collapse, no notification was made to dispatch regarding the trapped fire fighters.
Recommendation #12: Fire departments should ensure that Mayday training program(s) are developed and implemented so that they adequately prepare fire fighters to call a Mayday.
Discussion: The first and foremost priority for fire fighter safety is not getting oneself into a situation that could potentially cause injury or death. The fire fighter must maintain situational awareness at all times while operating on the fireground. Knowledge and skill training on how to prevent a Mayday situation and how to call a Mayday should begin and be mastered before a fire fighter engages in fireground activities or other immediately dangerous to life and health environments. Beginner fire fighter training programs should include training on such topics as air management; familiarity with an SCBA, a radio, or PPE; crew integrity; reading smoke, fire dynamics, and fire behavior; entanglement hazards; building construction; and signs of pending structural collapse. If fire fighters do find themselves in a questionable position (dangerous or not), they must be able to recognize this and be trained on procedures for when and how a Mayday should be called. A fire fighter's knowledge, skill, and ability to declare a Mayday must be at the mastery level of performance. This performance level should be maintained throughout their career through training offered more frequently than annually.48
Fire departments must understand that each fire fighter may have a different interpretation of what is life-threatening. The ability of a fire fighter to call a Mayday is a complicated behavior that includes the affective, cognitive, and psychomotor domains of learning and performance.49 Any delay in calling a Mayday reduces the chance of survival and increases the risk to other fire fighters trying to rescue the downed fire fighter. This incident illustrates the need for fire fighters to be given specific Mayday procedures for when a Mayday must be called.
There are no rules on when a fire fighter must call a Mayday, and Mayday training is not included in the NFPA standard for fire fighter qualifications. It is up to the authority having jurisdiction to train members for emergency operations , 4, 6 and to develop rules and performance standards for a fire fighter to call a Mayday. The National Fire Academy (NFA) has two courses addressing the fire fighter Mayday doctrine: Q133 Firefighter Safety, Calling the Mayday, a 2-hour program covering the cognitive and affective learning domain of the fire fighter Mayday doctrine; and, H134 Calling the Mayday: Hands-on Training, an 8-hour course covering the psychomotor learning domain of the fire fighter Mayday doctrine. These courses are based on the military methodology used to develop and teach ejection doctrine to fighter pilots. A training CD is available to fire departments free of charge from the U.S. Fire Administration Publications Office.49, 50 The NFA Mayday courses present specific Mayday parameters or rules for when a fire fighter must call a Mayday. The courses may help fire departments in developing and teaching Mayday procedures for fire fighters. Also, NFPA 1001, 2013 edition, includes job performance requirements related to the fire fighter calling for assistance (such as a Mayday situation).51
The IAFF Fire Ground Survival program is another resource fire departments can use and was developed to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers, and chief officers.48
During this incident, neither department had conducted May Day training.
Additionally,
Recommendation #13: Authorities having jurisdiction who have adopted specific NFPA consensus standards as part of their safety and health standards should ensure their safety and health standards cite up-to-date editions of the standard and consider adopting additional NFPA consensus standards to better protect individual fire fighter safety and health.
Discussion: The NFPA has formulated numerous standards for the fire service to better prepare a fire department and its members for an emergency and to protect an individual's safety and health. As stated earlier within this report, the authority having jurisdiction (AHJ) within the state of WI had adopted several NFPA standards within its safety and health standards, but the AHJ's safety and health standards had not been updated to reflect newer editions of the selected NFPA standards. AHJs need to ensure that safety and health standards are routinely reviewed and updated so that an individual has the best opportunity to perform their job (as a fire fighter) safely. This AHJ should also consider adopting or incorporating additional NFPA standards within their safety and health standards such as:
- NFPA 1026 Standard for Incident Management Personnel Professional Qualifications
- NFPA 1407 Standard for Fire Service Rapid Intervention Crews
- NFPA 1500 Standard for Fire Department Occupational Safety and Health Program
- NFPA 1521 Standard for Fire Department Safety Officer
- NFPA 1561 Standard for Emergency Services Incident Management System
- NFPA 1620 Standard for Pre-Incident Planning
- NFPA 1720 Standard for the Organization and Deployment of Fire Suppression Operations, Emergency Medical Operations and Special Operations to the Public by Volunteer Fire Departments
There are many other NFPA standards related to medical evaluations, personal protective equipment, and SCBAs that should also be reviewed when considering adopting into an AHJs safety and health standard(s). Additional information regarding NFPA, these, other available standards can be viewed at http://www.nfpa.org/codes-and-standards/document-information-pages. (Link updated 8/12/2013)
Establishing one's own standards and/or adopting nationally recognized standards will assist in laying the foundation for continued fire fighter safety.
References
- 1st Fire department [2008]. Standard operating guides.
- Mutual Aid Fire Department [no date]. Suggested operations guide.
- NFPA [2010]. NFPA 1407 standard for fire service rapid intervention crews. 2010 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1500 standard on fire department occupational safety and health program. 2007 ed. Quincy, MA: National Fire Protection Association.
- WDSPS [1995 – 2011]. Chapter SPS 330, fire department safety and health standards. Madison, WI: Wisconsin Department of Safety and Professional Services. [https://docs.legis.wisconsin.gov/code/admin_code/sps/safety_and_buildings_and_environment/326_360/330.pdf]. Date accessed: July 2012.
- NFPA [2008]. NFPA 1001 standard for fire fighter professional qualifications. 2008 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1002 standard for fire apparatus driver/operator professional qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1021 standard for fire officer professional qualifications. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2012]. NFPA 1403 standard on live fire training evolutions. 2012 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2009]. NFPA 1901 standard for automotive fire apparatus. 2009 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2012]. NFPA 1911 standard for the inspection, maintenance, testing, and retirement of in-service automotive fire apparatus. 2012 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1971 standard on protective ensembles for structural fire fighting and proximity fire fighting. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1981 standard on open-circuit self-contained breathing apparatus (SCBA) for emergency services. 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1982 standard on personal alert safety systems (PASS). 2007 ed. Quincy, MA: National Fire Protection Association.
- NFPA [2012]. NFPA 1983 standard on life safety rope and equipment for emergency services. 2012 ed. Quincy, MA: National Fire Protection Association.
- Tigue D and Hoigard K. [2011]. Vintage timber truss roofs: claims waiting to happen. Available from the file sharing website Engineering.com. [http://files.engineering.com/download.aspx?file=VintageWoodTruss.pdf&folder=3dff03a2-c020-4095-9537-f5c9a66d23b0]. Date accessed: July 2012.
- NFPA [2008]. NFPA 1561 standard on emergency services incident management system. 2008 ed. Quincy, MA: National Fire Protection Association.
- NIOSH [2010]. NIOSH alert: preventing deaths and injuries of fire fighters using risk management principles at structure fires. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No.2010-153 [http://www.cdc.gov/niosh/docs/2010-153/].Date accessed: July 2012.
- Phoenix Fire Department [2009]. Written comment to NIOSH Docket # 141. March 9.
- IAFC [2009]. Rules of engagement for structural firefighting, increasing firefighter survival. [Draft]. Fairfax, VA: International Association of Fire Chiefs, Safety, Health and Survival Section.
- Grorud LJ [2009]. Written comment to NIOSH Docket # 141. March.
- Command Safety [2011]. Occupancy risks versus occupancy types. [http://commandsafety.com/2010/11/occupancy-risks-versus-occupancy-types/]. Date accessed: December 2011.
- Dodson D [2005]. The art of first-due. Fire Eng March:135 – 141.
- IFSTA [2008]. Essentials of fire fighting. 5th ed. Stillwater, OK: Oklahoma State University, College of Engineering, Architecture, and Technology, Fire Protection Publications, International Fire Service Training Association.
- NFPA [2008]. NFPA 1521 standard for fire department safety officer. 2008 ed. Quincy, MA: National Fire Protection Association.
- Dodson D [2007]. Fire department incident safety officer. 2nd ed. New York: Thomson Delmar Learning.
- Dunn V [1988]. Collapse of burning buildings, a guide to fireground safety. Saddle Brook, NJ: Penn Well.
- Dunn V [1998]. Risk management and lightweight truss construction. WNYF 58(1).
- NFPA [2010]. NFPA 1620 standard for pre-incident planning. 2010 ed. Quincy, MA: National Fire Protection Association.
- NIOSH [1999]. NIOSH alert: preventing injuries and deaths of fire fighters due to structural collapse. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 99-146. http://www.cdc.gov/niosh/docs/99-146/
- NIOSH [2007]. Career fire fighter dies and chief is injured when struck by 130-foot awning that collapses during a commercial building fire – Texas. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, FACE Report No. F2007-01. http://www.cdc.gov/niosh/fire/reports/face200701.html
- NIOSH [2005]. NIOSH alert: preventing injuries and deaths of fire fighters due to truss system failures. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 2005-132. http://www.cdc.gov/niosh/docs/2005-132/
- NIST [2011]. Structural collapse. Gathersburg, MD. National Institute of Standards and Technology, Fire Research Division. [http://nist.gov/fire/collapse.cfm]. Date accessed: July 2012.
- NFPA [2012]. NFPA 220 standard on types of building construction. 2012 ed. Quincy, MA: National Fire Protection Association.
- Klaene BJ, Sanders RE [2000]. Structural fire fighting. Quincy, MA: National Fire Protection Association.
- Dunn V [1992]. Safety and survival on the fireground. Saddle Brook, NJ: Fire Engineering Books and Videos.
- Brannigan FL [1999]. Building construction for the fire service. 3rd edition. Quincy, MA: National Fire Protection Association.
- Endsley MR, Garlan J [2000]. Situational awareness analysis and measurement. Mahwah, NJ: Lawrence Erlbaum Associate.
- IFSTA [2010]. Building construction related to the fire service, 3rd ed. Stillwater, OK: Fire Protection Publications. International Fire Service Training Association.
- Norman J [2005]. Fire officer's handbook, 3rd ed. Tulsa, OK: Penn Well Corporation: Fire Engineering.
- Smith JP [2002]. Strategic and tactical considerations on the fireground. Upper Saddle River, NJ: Prentice Hall.
- NFPA [2010]. NFPA 1221 standard for the installation, maintenance, and use of emergency services communications systems. 2010 ed. Quincy, MA: National Fire Protection Association.
- Angulo RA, Clark BA, Auch S [2004]. You called Mayday! Now what? Fir Eng September.
- Clark BA [2004]. Calling a mayday: the drill [http://www.firehouse.com/article/10515446/calling-a-mayday-the-drill]. Date accessed: July 2012. (Link Updated 1/29/2013)
- DiBernardo JP [2003]. A missing firefighter: give the mayday. Firehouse, November.
- Sendelbach TE [2003]. Managing the fireground mayday. [http://www.firehouse.com/article/10541890/managing-the-fireground-mayday]. Date accessed: July 2012.
- Miles J, Tobin J [2004]. Training notebook: mayday and urgent messages. Fir Eng April.
- IAFF. IAFF Fire Ground Survival Program. International Association of Fire Fighters [http://www.iaff.org/HS/FGS/FGSIndex.htm]. Date accessed: July 2012.
- Clark, BA [2005]. 500 Maydays called in rookie school [http://www.firehouse.com/article/10498807/500-maydays-called-in-rookie-school]. Date accessed: July 2012. (Link Updated 1/29/2013)
- Clark BA [2008]. Leadership on the line: firefighter Mayday doctrine where are we now? [http://www.firehouse.com/podcast/10459336/leadership-on-the-line-firefighter-mayday-doctrine-where-are-we-now]. Date accessed: July 2012. (Link Updated 1/29/2013)
- NFPA [2013]. NFPA 1001 standard for fire fighter professional qualifications. 2013 ed. Quincy, MA: National Fire Protection Association.
- Bryner N, Mensch A [2011]. Emergency first responder respirator thermal characteristics: workshop proceedings. Workshop held in Pittsburgh, PA in July 2010, NIST Special Publication 1123, Gaithersburg, MD, June 2011. [http://www.nfpa.org/~/media/files/research/research%20foundation/foundation%20proceedings/rfscbafacepiecesworkshopproceedings.pdf]. Date accessed: July 2012. (Link updated 11/12/2013)
- Bryner N, Braga G, and Mensch A [2011]. Fire exposures of fire fighter self-contained breathing apparatus facepiece lenses. NIST Technical Note 1724, National Institute of Standards and Technology, Gaithersburg, MD, November 2011. [http://www.nist.gov/manuscript-publication-search.cfm?pub_id=909917]. Date accessed: July 2012.
- NFPA Fall Report on Proposals [2012]. NFPA 1981 standard on open-circuit self-contained breathing apparatus (SCBA) for emergency services. Log #CP5, Log #CP6. Quincy, MA: National Fire Protection Association. [http://www.nfpa.org/Assets/files/AboutTheCodes/1981/1981-F2012-ROP.pdf]. Date accessed: July 2012.
Investigator Information
This incident was investigated by Stacy C. Wertman and Stephen T. Miles, Safety and Occupational Health Specialists with the Fire Fighter Fatality Investigation and Prevention Program, Surveillance and Field Investigations Branch, Division of Safety Research, NIOSH located in Morgantown, WV. This report was authored by Stacy C. Wertman. An expert technical review was provided by Deputy Fire Chief William (Billy) Goldfeder, EFO, of the Loveland-Symmes Fire Department, Ohio. A technical review was also provided by the National Fire Protection Association, Public Fire Protection Division.
Additional Information
Bowstring Truss Roofs
DO YOU KNOW WHERE THEY ARE? THE DANGERS OF THE BOWSTRING TRUSS ROOF by Jeffrey Pindelski, Battalion Chief, Downers Grove, IL, Fire Department. Health and Safety for Fire and Emergency Services Personnel, Vol 21, Issue 5, May 2010. Fire Department Safety Officers Association, Ashland, MA. http://www.fdsoa.org/news/getpdf.htm?file=/www/docs/fdsoa/pdfs/membersonly/articles/past_articles/2010_05_newsletter.pdf (Link no longer available 5/13/2015)
Buildingsonfire.com is a website dedicated to art and science of building construction, fire fighting and command risk management for operational excellence, and fire fighter safety. http://buildingsonfire.com
Near-miss at grocery store fire results in local wood truss roof warning sign legislation. Illinois truss sign law. http://www.lib.niu.edu/1994/im940809.html (Link no longer available 5/28/2013)
Command Safety is a website dedicated to building construction, command risk management, and fire fighter safety for field operations. http://commandsafety.com/
Chicago: Anatomy of a Building and its Collapse. http://commandsafety.com/2010/12/chicago-anatomy-of-a-building-and-its-collapse/
IAFC Rules of Engagement for Firefighter Survival
The International Association of Fire Chiefs (IAFC) is committed to reducing fire fighter fatalities and injuries. As part of that effort the nearly 1,000 member Safety, Health and Survival Section of the IAFC has developed DRAFT "Rules of Engagement for Structural Firefighting" to provide guidance to individual fire fighters, and incident commanders, regarding risk and safety issues when operating on the fireground. The intent is to provide a set of "model procedures" for structural fire fighting to be made available by the IAFC to fire departments as a guide for their own standard operating procedure development. http://websites.firecompanies.com/iafcsafety/files/2013/10/Rules_of_Engagement_short_v10_2.12.pdf (Link Updated 1/14/2014)
IAFF Fire Ground Survival Program
The purpose of the International Association of Fire Fighters (IAFF) Fire Ground Survival Program is to ensure that training for Mayday prevention and Mayday operations are consistent between all fire fighters, company officers and chief officers. Fire fighters must be trained to perform potentially life-saving actions if they become lost, disoriented, injured, low on air or trapped. Funded by the IAFF and assisted by a grant from the U.S. Department of Homeland Security through the Assistance to Firefighters (FIRE Act) grant program, this comprehensive fire ground survival training program applies the lessons learned from fire fighter fatality investigations conducted by the National Institute for Occupational Safety and Health (NIOSH) and has been developed by a committee of subject matter experts from the IAFF, the International Association of Fire Chiefs (IAFC) and NIOSH. http://www.iaff.org/HS/FGS/FGSIndex.htm
NFPA Safety Alert on SCBA Facepiece Lenses
On July 2, 2012, NFPA issued a safety alert on SCBA facepiece lenses when investigations and additional research found SCBA facepiece lenses may undergo thermal degradation when exposed to intense heat. Investigations conducted by the NIOSH FFFIPP from 2002-2011 found evidence of thermal degradation of facepiece lenses that may have been a contributing factor in three fatalities. NIOSH also reported on the investigation of three SCBAs from a state training academy where the SCBA facepiece lens showed evidence of thermal degradation after being used in live fire training. Additionally, in four other NIOSH line-of-duty death investigations, the evidence, while not conclusive was suggestive of possible SCBA degradation or failure. Additional information on the alert including a full notice can be found at http://www.nfpa.org/research/resource-links/first-responders/nfpa-alert-self-contained-breathing-apparatus. (Link Updated 10/28/2013)
In addition, in 2010 the National Institute for Standards and Technology (NIST), NIOSH, the Fire Protection Research Foundation (FPRF) and the NFPA jointly hosted a research planning workshop on evaluating and addressing the concerns regarding the thermal impact of SCBA facepiece lenses.52 Subsequently, the United States Fire Administration (USFA) funded and participated with NIST in research53 that validated the adverse consequences to firefighters when lens degradation occurs in extreme thermal conditions and developed and provided new testing and performance methodologies to the NFPA Technical Committee on Respiratory Protection Equipment.54 Based on the information learned from the NIOSH investigations and NIST research, this Technical Committee is in the process of incorporating new test methods and performance criteria for facepiece lenses into the proposed 2013 edition of NFPA 1981,13 which is slated for completion and issuance as early as the Fall of 2012. Information on the continuing development of this new edition is available at http://www.nfpa.org/codes-and-standards/document-information-pages?mode=code&code=1981&docnum=1981&tab=nextedition&cookie%5ftest=1. (Link Updated 8/12/2013)
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
Appendix I
Status Investigation Report of One
Self-Contained Breathing Apparatus from the Fire Department
Submitted By the NIOSH Division of Safety Research
NIOSH Task Number 18485
(Note: The full report is available upon request.)
Background
As part of the National Institute for Occupational Safety and Health (NIOSH) Fire Fighter
Fatality Investigation and Prevention Program, the Technology Evaluation Branch agreed to examine and evaluate the self-contained breathing apparatus (SCBA) identified as the Mine Safety Appliances Company FireHawk, 2216 psi, SCBA.
This SCBA status investigation was assigned NIOSH Task Number 18485. The NIOSH Division of Safety Research was advised that NIOSH would provide a written report of the inspections and any applicable test results of this SCBA from the Fire Department.
The SCBA, contained within two boxes, was delivered to the NIOSH facility in Bruceton,
Pennsylvania on March 16, 2012. After its arrival, the packages were taken to building 20 and stored under lock until the time of the evaluation.
SCBA Inspection
The packages were opened in the Respirator General Inspection Area (building 20) and a complete visual inspection was conducted by Tom Pouchot, General Engineer, NPPTL. The SCBA was examined and inspected on May 16, 2012 and designated as Unit #1. Unit #1 was examined component by component, in the condition as received to determine their conformance to the NIOSH-approved configuration. The visual inspection process was photographed. Unit #1was identified as the MSA FireHawk, 30 minute, 2216 psi units, NIOSH approval number TC-13F-0473 based on the components of the SCBA.
The complete SCBA inspection is summarized in Appendix I of this evaluation report. The condition of each major component was also photographed with a digital camera. Images of the SCBA are contained in Appendix III of this evaluation report.
Unit #1, due to extensive damage, could not be safely pressurized and tested.
On May 17, 2012, a representative for the Mine Safety Appliances Company (MSA) down loaded the data logger included with this SCBA unit. The data download was performed at the MSA facility in Cranberry Township, Pennsylvania and the download was witnessed by NIOSH.
SCBA Testing
The purpose of the testing is to determine the SCBA’s conformance to the approval performance requirements of Title 42, Code of Federal Regulations, Part 84 (42 CFR 84). Further testing is also conducted to provide an indication of the SCBA’s conformance to the National Fire
Protection Association (NFPA) Air Flow Performance requirements of NFPA 1981, Standard on
Open-Circuit Self-Contained Breathing Apparatus for the Fire Service, 1997 Edition.
NIOSH SCBA Certification Tests (in accordance with the performance requirements of
42 CFR 84):
- Positive Pressure Test [§ 84.70(a)(2)(ii)]
- Rated Service Time Test (duration) [§ 84.95]
- Static Pressure Test [§ 84.91(d)]
- Gas Flow Test [§ 84.93]
- Exhalation Resistance Test [§ 84.91(c)]
- Remaining Service Life Indicator Test (low-air alarm) [§ 84.83(f)]
National Fire Protection Association (NFPA) Tests (in accordance with NFPA 1981,
1997 Edition):
- Air Flow Performance Test [Chapter 5, 5-1.1]
No report on testing is included as no testing was conducted.
Summary and Conclusions
A SCBA from the Fire Department was submitted to NIOSH by the NIOSH Division of Safety Research for evaluation. The SCBA was delivered to NIOSH on March 16, 2012 and inspected on May 16, 2012. The unit was identified as the MSA Company FireHawk, 2216 psi, SCBA (NIOSH approval number TC-13F-0473 based on the components, a 30 minute duration unit). Unit #1 suffered major damage from the fire and was covered with dirt, grime, foreign particulate material and soot. The cylinder valve as received could not be opened by hand. All the gauges were readable. The cylinder gauge indicated 0 psig in the cylinder. The facepiece was heavily damaged by heat along with the unit harness. Visibility through the lens was poor due to the heat damage. The low pressure hose was damaged and in two pieces. The PASS unit functioned. The SCBA air cylinder had some slight damage with foreign matter present on the cylinder. The NFPA/SEI label was present and readable but the NIOSH label was not visible.
The air cylinder on the Unit #1 had a manufactured date of 06/03. Under the applicable DOT-SP-10915-2216 exemption, the air cylinder is required to be hydro tested every 5 years, starting on or before the last day of 06/08. Therefore, it appears that the cylinder on this SCBA unit was due for hydro testing before the end of June 2008. The re-test label on the cylinder assembly for Unit #1 had a date of 09/08 and, therefore, it appears that this cylinder was within the hydro certification when last used. The Unit #1 cylinder also had some slight damage and foreign matter present.
On May 17, 2012, a representative for the Mine Safety Appliances Company (MSA) down loaded the data logger included with this SCBA unit. The data download was performed at the MSA facility in Cranberry Township, Pennsylvania and the download was witnessed by NIOSH.
In light of the information obtained during this investigation, NIOSH has proposed no further action on its part at this time. Following the visual inspection, the SCBA was returned to storage pending return to the Fire Department.
APPENDIX II
SCBA Data Logger
Last Recorded Data Entry for the SCBA Used by the Victim
(Note: The date and time do not coincide with the incident date.)
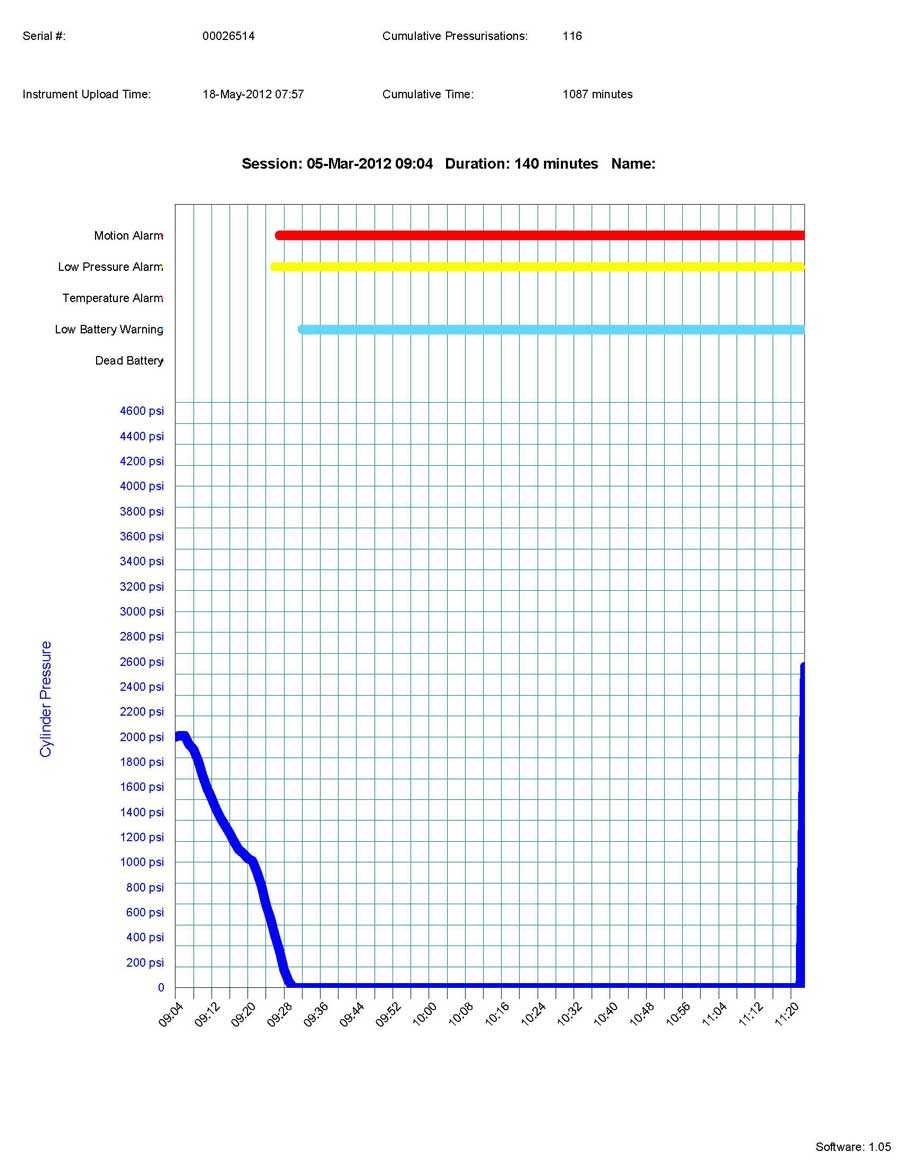
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1998, Congress appropriated funds to NIOSH to conduct a fire fighter initiative that resulted in the NIOSH “Fire Fighter Fatality Investigation and Prevention Program” which examines line-of-duty-deaths or on duty deaths of fire fighters to assist fire departments, fire fighters, the fire service and others to prevent similar fire fighter deaths in the future. The agency does not enforce compliance with State or Federal occupational safety and health standards and does not determine fault or assign blame. Participation of fire departments and individuals in NIOSH investigations is voluntary. Under its program, NIOSH investigators interview persons with knowledge of the incident who agree to be interviewed and review available records to develop a description of the conditions and circumstances leading to the death(s). Interviewees are not asked to sign sworn statements and interviews are not recorded. The agency's reports do not name the victim, the fire department or those interviewed. The NIOSH report's summary of the conditions and circumstances surrounding the fatality is intended to provide context to the agency's recommendations and is not intended to be definitive for purposes of determining any claim or benefit.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research