


Fire Fighter / Emergency Medical Technician Dies in Apparatus Incident at Wildland Fire - California
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F99-42 Date Released: May 9, 2000
SUMMARY
On October 16, 1999, four volunteer fire fighters (Chief and two fire fighters from Volunteer Department #1 and a Chief from Volunteer Department #2) responded to a request for assistance in fighting wildland brush fires that were endangering several structures. The brush fires were burning approximately 60 miles east of the departments' home location. The fire fighters traveled in two different vehicles. The two volunteer Chiefs brought the engine, and one male and one female fire fighter (the victim) drove a privately owned vehicle (POV) to the brush fires, stopping along the way to pick up some refreshments. After meeting up with the two Chiefs on the engine, the four assisted in fighting brush fires, then they proceeded down the highway to look for structures endangered by fire. A determination was made to relocate the POV, so the Chief stopped the engine across the highway from the POV. The victim and the Chief from Volunteer Department #1 intended to ride together in the POV; however, unknown to the Chief in the engine, the victim picked up some soft drinks from the POV and proceeded back across the highway to the engine (see diagram). The victim apparently stepped up on the sideboard of the engine and was going to pass the soft drinks through the pass-through window when the Chief started to move the engine forward. The victim lost her balance, and she turned and jumped toward the center of the highway, landing in a squatting position and off balance. She then fell backward toward the slow-moving engine, and her head was caught by the rear dual wheels. NIOSH investigators concluded that to minimize similar occurrences, fire departments should
ensure fire fighters are aware of individual roles and responsibilities when members have not worked together
ensure effective communications between crew members
ensure fire fighters are aware of responsibilities regarding getting on and off an apparatus
INTRODUCTION
On October 16, 1999, four volunteer fire fighters (Chief and two fire fighters from Volunteer Department #1 and a Chief from Volunteer Department #2) responded to a request for assistance in fighting wildland brush fires that were endangering several structures. The fire fighters traveled in two different vehicles (an engine and a POV) to the incident site. Being from two different departments, the fire fighters had not trained together and were not familiar with individual roles and responsibilities. After assisting in fighting several brush fires, a decision was made to move the POV to a different location. The victim had proceeded to the POV and was going to bring refreshments back to the engine when the fatal incident occurred.
On November 17-18, 1999, an investigation of this incident was conducted by the NIOSH Senior Fire Fighter Investigator. Interviews were conducted with the following: the Chief of Volunteer Department #1, the Chief of Volunteer Department #2, and representatives from the California Department of Forestry (CDF). A copy of the CDF informational summary report was also obtained. The diagram used in this report was provided by the CDF.
The two volunteer departments involved in this incident are comprised of the following: Volunteer Department #1 - Chief and 13 fire fighters, and Volunteer Department #2 - Chief and 15 fire fighters. The training in both departments requires all new recruits to comply with the requirements of the CDF. The recruits are on probation for the first 6 months. Hands-on training is provided during monthly drills, and specialized training is provided periodically by CDF instructors. The victim had 9 years' experience as a volunteer fire fighter. Both departments are responsible for several hundred square miles of sparsely populated, mountainous terrain.
INVESTIGATION
On October 16, 1999, at 0630 hours, the county sheriff's office placed a radio call to the county fire districts requesting assistance in fighting wildland brush fires that were endangering several structures approximately 60 miles east of their location. Since equipment and personnel were already committed to other locations at this time, two volunteer departments formed a team comprised of the following personnel and equipment: a Chief and two fire fighters (one was the victim) from Volunteer Department #1 and a Chief and an engine from Volunteer Department #2. The Chief of Volunteer Department #1, accompanied by a female volunteer fire fighter/emergency medical technician (the victim), drove her privately owned vehicle (POV) approximately 25 miles east, where they met up with the Chief of Volunteer Department #2 and a fire fighter from Volunteer Department #1. The Chief of Volunteer Department #2, accompanied by the Chief of Volunteer Department #1, drove his engine to the staging area for assignment. The two volunteer fire fighters from Volunteer Department #1 drove the POV to the staging area. They stopped along the way to pick up refreshments and eventually met up with the two Chiefs on the engine. All four assisted other units in fighting brush fires that were threatening structures, then they proceeded down the highway. At approximately 1330 hours, the victim told the Chief to stop the engine where they had parked the POV, and she would pick up some refreshments. It was decided that the victim should move the POV to a different location. The victim and the Chief of Volunteer Department #1 got off the engine and proceeded across the highway to the POV. However, unknown to the Chief in the engine, the victim had picked up some soft drinks from the POV and proceeded back across the highway to the engine (see diagram). The victim apparently stepped up on the sideboard of the engine and was going to pass the soft drinks through the rear pass-through window over the jump seat when the Chief started to move the engine forward. The victim lost her balance, and she turned and jumped toward the center of the highway (facing the POV), landing in a squatting position and off balance. She then fell backward toward the slow-moving engine, and her head was caught by the rear dual wheels. The victim died instantly.
CAUSE OF DEATH
According to the medical examiner, the cause of death was blunt force trauma to the head.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Fire departments should ensure fire fighters are aware of individual roles and responsibilities when members have not worked together.1
Discussion: The strike force team involved in this incident consisted of a Chief and two fire fighters from one volunteer fire department and a Chief from another volunteer fire department. When members of fire departments have never worked together, difficulties may arise which may cause confusion at the emergency scene. To minimize confusion at the emergency scene, a unifying system should be employed to establish roles and responsibilities. The Incident Command System (ICS) has been successfully used in managing available resources at a variety of emergency operations. The system consists of procedures for controlling personnel, facilities, equipment, and communications. In this incident, if an ICS had been applied and adhered to, then roles and responsibilities could have been determined, and the incident may have been avoided.
Recommendation #2: Fire departments should ensure effective communications between crew members.1
Discussion: Effective communications between team members and the Incident Commander is essential to maintain a level of safety in all operations. When members departed the engine, it was not acknowledged that any were returning to the engine.
Recommendation #3: Fire departments should ensure fire fighters are aware of responsibilities regarding getting on and off an apparatus.2
Discussion: The driver of an apparatus (engine) should not start to move the vehicle until all persons are seated and secured. The victim had left the engine, and without the knowledge of the Chief (driver of the engine), had returned and jumped on the sideboard behind and out of sight of the driver. When the Chief started to move the engine forward, the victim lost her balance and had to jump from the engine.
REFERENCES
1. National Fire Protection Association [1995]. NFPA 1561, Standard on fire department incident management system. Quincy, MA: National Fire Protection Association.
2. National Fire Protection Association [1997]. NFPA 1500, Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
INVESTIGATOR INFORMATION
This investigation was conducted by Ted A. Pettit, Senior Fire Fighter Investigator, NIOSH, Division of Safety Research.
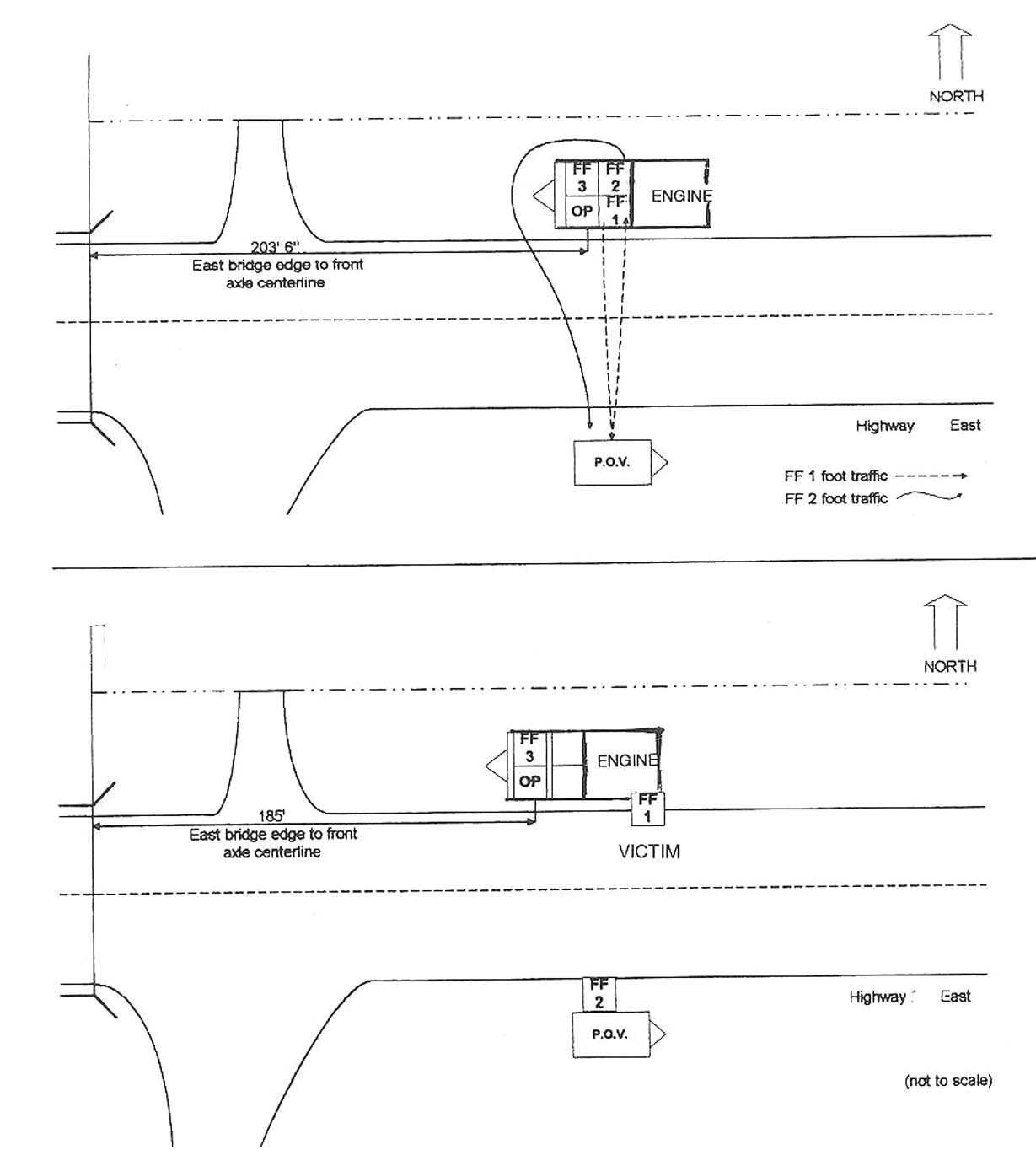
Diagram. Overview of Incident Scene
This page was last updated on 05/17/00
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research