Amiodarone pulmonary toxicity
Contents
Background
Amiodarone is an antiarrhythmic agent commonly used to treat supraventricular and ventricular arrhythmias. This drug is an iodine- containing compound with a large volume of distribution that tends to accumulate in several organs, including the lungs. Although the incidence of this complication has decreased with the use of lower doses of amiodarone, it can occur with any dose.[1] Since amiodarone has a long half life it is possible of effects to persist well after discontinuation.
Pathophysiology
Amiodarone and its metabolites can produce lung damage dir- ectly by a cytotoxic effect and indirectly by an immunological reaction.[2] Amiodarone may induce the production of toxic O2 radicals, which can directly damage cells.[3]
Clinical Features
Differential Diagnosis
Amiodarone Adverse effects
- Bradycardia
- Hypotension with older solvent-based formulation. Uncommon with newer aqueous formulation.
- Prolonged QT
- Thyrotoxicosis[4]
- Between 5-20% of patients treated with amiodarone have thyrotoxicosis (higher in areas of iodine deficiency)
- Iodine-induced hyperthyroidism
- It is thought that the iodine load may unmask hyperthyroidism in patients with multinodular goiter and subclinical Graves’ disease
- Drug-induced destructive thyroiditis
- More commonly, the cytotoxic effects of amiodarone destroy thyroid cells, resulting in a release of preformed hormone.
- Amiodarone Pulmonary Toxicity
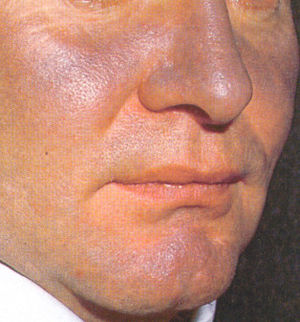
- Hyperpigmentation rash
Evaluation
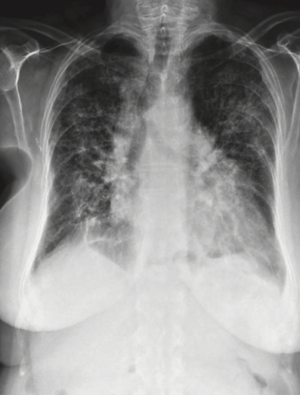
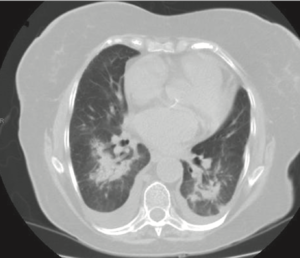
The diagnosis is often clinical and due presence of ground glass opacities of CT in the setting of amiodarone use and after exclusion of an infectious etiology such as pneumonia.
Lung CT Findings
- Ground glass opacities with interstitial or alveolar inflitrations and lung nodules
- Pleural thickening and pleural effusions
Management
Disposition
- Admit the patient for rule out of an infectious etiology.
- Consult with the patient's pulmonologist or cardiologist for recommendations on stopping the amiodarone
See Also
References
- ↑ Wolkove N, Baltzan M. Amiodarone pulmonary toxicity. Can Respir J. 2009;16(2):43-48.
- ↑ Martin WJ, Rosenow EC. Amiodarone pulmonary toxicity: Recognition and pathogenesis (Part 2). Chest 1988;93:1242-8.
- ↑ Jessurum GA, Crijns HJG. Amiodarone pulmonary toxicity. BMJ 1997;314:619-20.
- ↑ Rosen's 8th Edition