We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Babesiosis
From WikEM
Contents
Background
- Spread by the deer tick (Ixodes scapularis)
- People often unaware they are bitten
- Natural reservior is the white footed mouse
- Endemic in US, Europe, parts of Russia and China
- Babesia Microti is pathogen in US
- Possible to have co-infection with Lyme (same tick family)
Clinical Features
- Fever, hemolytic anemia, chills, thrombocytopenia, DIC
- More severe disease in immunocompromized patients (HIV, Elderly, Asplenic)
Differential Diagnosis
Tick Borne Illnesses
- Babesiosis
- Ehrlichiosis
- Lyme
- Rocky mountain spotted fever
- Tularemia
- STARI
- Heartland virus
- Tick paralysis
- Murine typhus
Evaluation
- CBC
- Often with depressed white count
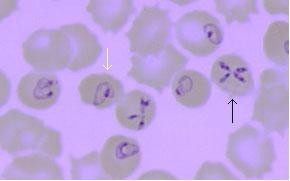
- Peripheral Blood Smears
- Shows intracellular parasites: Maltese Cross sign
- May need large smear as parasitemia can be as low as 1%
- Can often be confused for malaria parasites
- Electrolytes and renal function
- LFTs
- Total bilirubin and haptoglobin values reflect the intensity of the infection (hemolysis)
- Lyme
- Urine - hemolysis
- CXR - rare but possible ARDS
Management
2 drug regimen for 7-10 days
Option 1
- Atovaquone (750mg BID) and Azithromycin (500-1000mg on first day, 250-1000mg on subsequent days)[1]
Option 2
- 600 mg PO q8h x 7-10 days
- Alt: 300-600mg IV q6h x 7-10 days
- First Dose: 300-600mg IV x 1
- Give with Quinine (650mg TID); use IV for severe infections
Pediatrics
- Clindamycin 20mg/kg/day for children and 25mg/kg/day for children for 7-10 days
Disposition
See Also
External Links
References
- Tobler WD, Cotton D, Lepore T, Agarwal S, Mahoney EJ. Case Report: Successful non-operative management of spontaneous splenic rupture in a patient with babesiosis. World Journal of Emergency Surgery : WJES. 2011;6:4. doi:10.1186/1749-7922-6-4.
- ↑ Krause PJ, Lepore T, Sikand VK, Gadbaw J Jr, Burke G, Telford SR 3rd, et al. Atovaquone and azithromycin for the treatment of babesiosis. N Engl J Med. Nov 16 2000;343(20):1454-8.