We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Bartholin gland abscess
From WikEM
(Redirected from Bartholin Gland Abscess)
Contents
Background
- Ducts of the glands drain into posterior vestibule at 4 o'clock and 8 o'clock positions
- A cyst does not need to be present for an abscess to develop
Clinical Features
- Mass in posterior introitus near 4 o'clock or 8 o'clock position
- May develop over days or longer time (if preceded by cyst)
- Systemic symptoms (e.g. fever/chills) are rarely present
Differential Diagnosis
- Cysts of other glandular structures
- Leiomyoma
- Lipoma
- Carcinoma (consider in older women who present with introital mass)
Skin and Soft Tissue Infection
- Cellulitis
- Erysipelas
- Lymphangitis
- Abscess
- Bartholin gland abscess
- Necrotizing soft tissue infections
- Mycobacterium marinum
Look-A-Likes
Evaluation
- Usually clinical diagnosis
Management
Incision and Drainage
I&D only perform once abscess is well-defined, walled-off structure
Word Catheter
- Inject local anesthetic
- Stab incision is made on the mucosal surface
- Extend incision for several mm but not so many that the Word catheter will fall out
- Insert Word catheter and inflate balloon with 2-4mL of water
- Tuck end of catheter into the vagina
- Catheter should remain in place for 4-6wk to avoid recurrence
Rubber Ring Catheter (Jacobi Ring)[1][2]

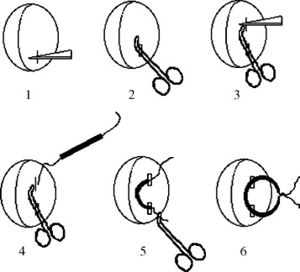
Less cumbersome for the patient and less likely to fall out and similar in procedure as a loop drain for a cutaneous abscess
- Additional equipment: 7-cm length of an 8–French T tube (can also use tubing from butterfly catheter) threaded with a 20-cm length of 2-0 silk suture.
- Inject local anesthetic
- Stab incision is made on the mucosal surface
- Pass hemostat into abscess cavity to lyse adhesions, and tunnel to make indentation for second incision
- Grab one end of Jacobi ring and pull through abscess cavity
- Tie two ends to form closed ring. DO NOT TIE TOO TIGHT (pressure necrosis risk)
Antibiotics
- Cefixime 400mg PO QD x7d + clindamycin 300mg PO QID x7d
Wound Care
- Sitz bath x2 days
- Abstain from vaginal intercourse
- Refer to GYN if >40yr (might need biopsy to rule out CA) and recurrence (complete excision vs. marsupialization)
Disposition
- Usually outpatient management
See Also
References
- ↑ Gennis P, Li SF, Provataris J, Shahabuddin S, Schachtel A, Lee E, Bobby P. Jacobi ring catheter treatment of Bartholin’s abscesses. Am J Emerg Med. 2005 May;23(3):414-5
- ↑ Kushnir VA, Mosquera C. Novel technique for management of Bartholin gland cysts and abscesses. J Emerg Med. 2009 May;36(4):388-90
- ↑ AEJM artle
- ↑ AEJM artle