EBQ:Ottawa Ankle Rule Study
PubMed Full text PDF
Contents
Clinical Question
Can a clinical decision rule be used to aid in the efficient use of radiography in acute ankle injuries?
Conclusion
The Ottawa Ankle Rule is a highly sensitive decision rule used to determine the need for radiography in patients with acute ankle injuries.
Major Points
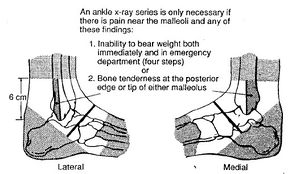
Ottawa ankle rule
Ankle x-ray needed if:
- Pain near the maleoli AND
- Inability to bear weight immediately and in the ED (4 steps) OR
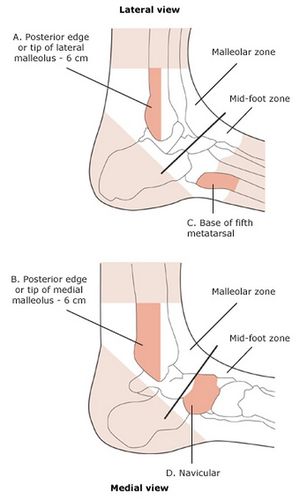
- Tenderness at posterior edge or tip of lateral malleolus OR
- Tenderness at posterior edge or tip of medial malleolus
Rule had 100% sensitivity and 49% specificity for identifying 50 clinically significant malleolar zone fractures in the prospective validation study.
Ottawa foot rules
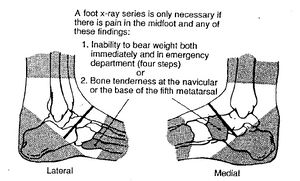
Foot x-ray series needed if:
- Pain in the midfoot AND
- Inability to bear weight both immediately and in the ED (4 steps) OR
- Tenderness at the navicular OR
- Tenderness at the base of the 5th metatarsal
Rule had 100% sensitivity and and 79% specificity for identifying 19 clinically significant midfoot fractures in the prospective validation study.
Study Design
- Conducted in 2 stages in 2 Canadian EDs, both prospective cohort studies
- First stage
- Each patient was evaluated for 15 clinical variables as defined by previously derived clinical decision rules. All patients then underwent radiographs--standard ankle series for patients with pain in malleolar zone vs. standard foot series for patients with pain in the midfoot zone.
- Original decision rule then refined by univariate and recursive partitioning analyses.
- Second stage
- Each patient was evaluated for 6 clinical variables, and the decision rule was applied to determine necessity of radiographs.
- In both studies, a subset of patients were also assessed by second EM physician independently when possible.
- Clinically significant fracture seen in ankle or foot radiographic series was the primary outcome
- Defined as bone fragments greater than 3 mm in breadth.
- All radiographic series were interpreted by qualified radiologists who were blinded to the data collection sheets.
Population
Patient Demographics
Similar characteristics in stage 1 (refinement) vs. stage 2 (validation)
- Mean age: 35 vs. 36
- Male sex: 52% vs. 52%
- Pt at Ottawa Clinic: 60% vs. 64%
- Twisting mechanism: 84% vs. 86%
- Clinically significant fractures: 16% vs. 15%
- Clinically insignificant fractures: 6% vs. 7%
- Ankle rediographs performed: 85% vs. 85%
- Foot radiographs performed: 39% vs. 35%
Inclusion Criteria
- Patients who presented to the emergency department with pain or tenderness 2/2 to blunt ankle trauma due to any mechanism
- Ankle defined as area commonly involved in twisting injuries
- Malleolar zone
- Distal 6 cm of tibia, fibula, talus
- Midfoot zone
- Navicular bone, cuboid, cuneiforms, anterior process of calcaneus, base of 5th metatarsal
- Malleolar zone
- 1 of 21 designated EM physicians had to be on duty
Exclusion Criteria
- Age <18 years old
- Pregnant
- Isolated injuries of the skin
- Referred from outside hospital with radiographs
- Injury occurred >10 days previously
- Returned for reassessment of the same injury
Interventions
- Refinement stage was a prospective observational study
- In validation phase, the clinical decision rule was applied. If patients were positive for any 1 of the 6 clinical variables (listed in major points), an x-ray series was performed.
- Standard ankle series completed in patients with positive Ottawa Ankle Rule, standard foot series completed in patients with positive Ottawa Foot Rule
Outcomes
First stage (validation and refinement of original rules): n=1032 enrolled and assessed
Second stage (validation of refined rules): n=453 enrolled and assessed
Primary Outcome
First stage (refinement): 121 (12%) clinically significant malleolar zone fractures and 49 (5%) clinically significant midfoot zone fractures identified
Performance of the Ottawa Decision Rule in the second stage (validation) cohort
| Ankle Decision Rule | Fracture | No Fracture |
|---|---|---|
| Rule Positive | 50 | 205 |
| Rule Negative | 0 | 198 |
Sensitivity 100% (95% CI 93% to 100%)
Specificity 49% (95% CI 44% to 54%)
| Foot Decision Rule | Fracture | No Fracture |
|---|---|---|
| Rule Positive | 19 | 90 |
| Rule Negative | 0 | 344 |
Sensitivity 100% (95% CI 83% to 100%)
Specificity 79% (95% CI 75% to 83%)
Secondary Outcomes
Stage 1 (refinement)
- Physicians correctly classified patients according to the ankle and foot decision rules in 97% and 98%
- Inter-observer agreement between physicians for ankle and foot decision rules was 56% and 69%
Stage 2 (validation)
- Physicians correctly classified patients according to the ankle and foot decision rules in 99% and 100%
- Potential reduction in radiography for ankle and foot series estimated to be 34% and 30%
- Likelihood ratio negative for a fracture estimated to be 0
Subgroup analysis
Further Discussion
- Rules may not be useful in patients with multiple painful injuries, altered sensorium, intoxication, paraplegia, or bone disease
- During the study, the rule had limited experience with uncommon fractures
- 2 fractures of talus
- 12 fractures of midfoot other than base of 5th metatarsal
- A subsequent study by Stiell in 1994 confirmed the high sensitivity and demonstrated reduction the number of ankle X-rays by 36% [1]
- The rules have been shown to be easily applied with education in multiple centers [2] but due to poor interrater reliability from the general public, self application of the rule to decrease ED visits was not possible [3]
- The rules have been validated in assessing children 2-16 years old, with 100% sensitivity [4]
- However in 1 of the 2 centers in this study, the decision rules would have increased the use of x-ray for ankle injuries, suggesting that the benefit of these decision rules may not be as great in a pediatric setting.
Funding
Grant from Emergency Health Services Branch of Ontario Ministry of Health, Toronto
See Also
References
- ↑ Stiell IG et al. Implementation of the Ottawa ankle rules. JAMA. 1994 Mar 16;271(11):827-32.
- ↑ Stiell I. et al. Multicentre trial to introduce the Ottawa ankle rules for use of radiography in acute ankle injuries. Multicentre Ankle Rule Study Group. BMJ. 1995 Sep 2;311(7005):594-7
- ↑ Blackham JE et al. Can patients apply the Ottawa ankle rules to themselves? Emerg Med J. 2008 Nov;25(11):750-1.
- ↑ Plint AC. et al. Validation of the Ottawa Ankle Rules in children with ankle injuries. Acad Emerg Med. 1999 Oct;6(10):1005-9.
Authors
Catie Reynolds, Daniel Ostermayer, Neil Young, Ross Donaldson, Claire