We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Felon
From WikEM
Contents
Background
- Subcutaneous pyogenic infection of the pulp space compartments of the distal finger
- Do not mistake for pulp erythema due to paronychia or herpetic whitlow
- Infection typically begins with minor trauma to dermis overlying finger pad (e.g. foreign body such as a splinter)
- May spread to flexor tendon sheath, IP joint, or underlying periosteum

Clinical Features
- Red, tense, and markedly painful distal pulp space
Differential Diagnosis
Hand and finger infections
- Bedbugs
- Closed fist infection (Fight Bite)
- Hand cellulitis
- Hand deep space infection
- Herpetic whitlow
- Felon
- Flexor tenosynovitis
- Paronychia
- Scabies
- Sporotrichosis
Evaluation
Workup
- X-ray to assess for foreign body
- US can be utilized by placing the hand in a bowel of water and holding high frequency linear probe a few cm away from the finger (water is an excellent conductor)
- Gram stain and culture (chronic infections may be caused by atypical organisms)
Evaluation
- Usually a clinical diagnosis
Management
Incision and drainage
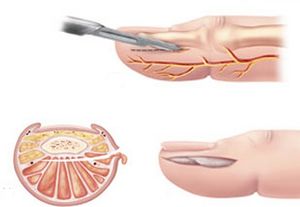
- The incision should be made along the ulnar aspect of the index, middle, and ring fingers and along the radial aspects of the thumb and little finger.
- Number 11 blade is used to make incision on nonoppositional side of affected digit
- Start incision 5 mm distal to flexor DIP crease
- End incision 5mm proximal to nail plate border
- Bluntly dissect and explore wound until abscess is decompressed
no need for packing
- DO NOT perform a "fishmouth" incision since this may results in: Unstable finger pad, neuroma, and/or loss of sensation
Antibiotics
Indicated for felon associated with cellulitis Definitive treatment is drainage but antibiotic coverage for S. aureus and Strep with caution to identify Herpetic whitlow
- Cephalexin 500mg PO q6hrs daily x 7 days
- TMP/SMX 2 DS tablets PO q12hrs x 7 days
- Clindamycin 450mg PO q8hrs x 7 days
- Dicloxacillin 250mg PO q6hrs daily x 7 days
Disposition
- Discharge with follow-up in 2 days for wound check
- Refer to hand surgery only if systemically ill or concern for complicated infection
- Instruct patient to keep extremity elevated