We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Fifth metatarsal fracture
From WikEM
Contents
Background
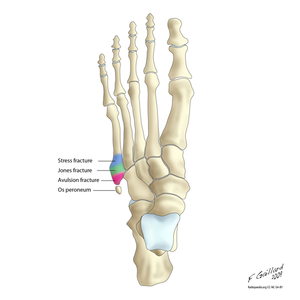
- Os peroneum is an accessory bone (ossicle) located at the lateral side of the tarsal cuboid, proximal to the base of 5th metatarsal, commonly mistaken for a fracture
Clinical Features
Tuberosity (styloid) avulsion fracture
- Most common fracture at base of 5th metatarsal
- Sx often mild, patients usually present with sprained ankle complaint
- Occurs due to forced inversion foot/ankle while in plantar flexion
Jones or metaphyseal-diaphyseal junction fracture
- Second most common fracture at base of 5th metatarsal
- Abrupt onset of lateral foot pain, with no prior history of pain at that site, suggests acute injury and helps distinguish from stress injury
- Occurs due to sudden change in direction with heel off the ground
- Edema & ecchymosis usually present, may not be able to bear weight
Diaphyseal stress fracture
- Occurs through repetitive microtrauma, usually in younger athletes
- Important to identify given propensity for delayed union and nonunion
- Usually present with history of months of pain, which is more intense during exercise or weight-bearing
- always ask about persistent pain prior to acute event to help distinguish worsening stress fracture from acute fracture
Differential Diagnosis
Foot and Toe Fractures
Hindfoot
Midfoot
Forefoot
- Fifth metatarsal fracture
- Non-fifth metatarsal fracture
- Toe fracture
Evaluation
Plain radiographs are usually adequate
- Must distinguish Jones fracture from diaphyseal stress freacture:
- Acute fracture will have narrow fracture line that appears sharp, normal thin cortex adjacent to fracture, and normal intramedullary canal
- Stress fracture will demonstrate cortical thickening near fracture line, older stress fracture will demonstrate widened fracture line and intramedullary sclerosis
Management & Disposition
Tuberosity (Styloid) Avulsion Fracture
- Refer to ortho if > 3mm displacement
- Nondisplaced fracture usually require only symptomatic treatment, RICE
- Walking boot (casting rarely necessary) and weight-bearing as tolerated, follow up in 1 week
Jones Fracture (non-displaced)
- Posterior Ankle Splint, strict NWB, RICE, ortho follow up in 3-5 days
- 50% of Jones fracture treated conservatively may result in nonunion or re-fracture
- Conservative treatment failure usually due to poor vascular supply of bone and premature return to weight-bearing
Diaphyseal Stress Fracture
- Strict NWB short-leg cast, RICE
- Ortho referral for all stress fractures
See Also
References
Video