We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Hypokalemia
From WikEM
Contents
Background
Clinical Features
- Central nervous system
- Gastrointestinal
- Renal
- Cardiovascular
- PACs/PVCs
- Bradycardia or atrial/junctional tachycardia
- AV block
- Ventricular tachycardia, Ventricular fibrillation
Differential Diagnosis
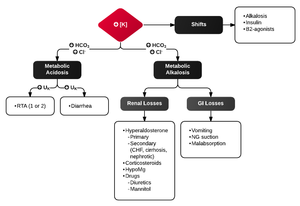
Intracellular Shift
- Alkalosis (each 0.10 rise in pH causes 0.5 decrease)
- Insulin
- B-agonist
Decreased intake
- Special diets or those low in potassium
- Chronic alcohol abuse
Increased loss
- GI
- Vomiting, diarrhea, fistula
- Renal
- Diuretics
- Hyperaldo
- Exercise
- Hypercalcemia
- Hypomagnesemia
Drugs
- Penicillins
- Lithium
- L-dopa
- Theophylline, methlxanthines
- Insulin
- Barium
- Quinine
- Catecholamines
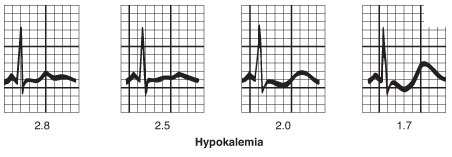
Evaluation
- Serum potassium level is diagnostic
- Normal = 3.5-5meq/L
- Severe hypokalemia = <2.5meq/L
- Always check magnesium
- Suggestive ECG findings:
Management
- Potassium repletion (PO or IV)
- Every 10mEq KCl → serum K ↑ ~0.1mEq/L
- PO preferred (if symptomatic or level is <2.5, both oral and IV should be given)
- Oral potassium
- Inexpensive and rapidly absorbed
- KCl tablet (elixir form available but has poor taste)
- K-Dur (extended release tablet) is large and may be difficult to swallow
- Intravenous potassium
- Must be given in dilute solutions at slow rate (10meq/hour) to minimize side effects and cardiac toxicity
- Generally should not give more than 40mEq via IV
- Side effects: Local tissue burning, phelbitis, sclerosis
- Also treat Hypomagnesemia if present
- Re-check ECG after treatment [1]
Disposition
- Based on underlying cause
See Also
External Links
References
- ↑ Slovis, Corey. "Electrolyte Emergencies". Presentation.