We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Intrauterine device problems
From WikEM
Contents
Background
- Intrauterine devices (IUDs) are one of the most effective contraceptive methods
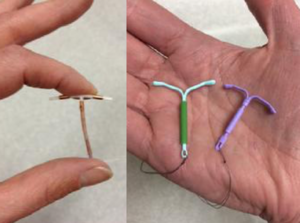
- T-shaped device inserted through cervix, can be used for up to 3-12 years
- Serious complications are rare, <1% of women with IUDs
- Copper IUD (Paraguard):
- lasts up to 12 years, no hormones, usually cheaper
- tend to cause more side effects (heavy/irregular menses, pelvic pain)
- also extremely effective as emergency contraception if inserted within 120 hours of unprotected sex
- Hormonal IUDs (Mirena, Liletta, Mirena, Skyla, Kyleena): secrete small amount of progestin (levonorgestrel)
- MIrena effective up to 6 years, the others for 3-5 years
- Menses tend to get significantly lighter or disappear altogether after the first few months
- Very little progestin absorbed systemically, so women tend NOT to have the hormonal side effects or increased DVT/PE risk associated with oral contraceptives[1]
Complications and Management
"Lost" IUD
- Most common IUD-related reason for ED presentation
- Small removal strings are left protruding from cervix on insertion
- Women are instructed to feel for string with finger, if strings seem shorter or cannot be felt, may indicate malposition or complication
- Management:
- Attempt to visualize strings
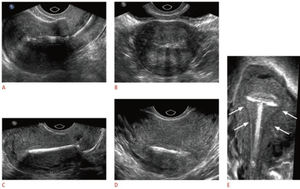
- If cannot, IUD position can be confirmed on ultrasound or (for copper IUDs) abdominal x-ray
- If extrauterine, needs surgical removal
Uterine perforation
- Extremely rare
- Suspect in patient with IUD and symptoms of endometritis, salpingitis, and/or peritonitis
- Diagnosed by imaging: IUD may be imbedded in uterine wall or free in peritoneum
- Requires emergent Ob/gyn consult for surgical removal/repair
Pregnancy with IUD in place
- Extremely rare, as IUDs are >99% effective in preventing pregnancy[2]
- Increased risk of ectopic pregnancy if hCG positive and IUD still in place
- Consult OB/Gyn for urgent evaluation/management
PID
- IUD use associated with increased rate of PID, particularly in first 21 days after insertion
- Related to preexisting STDs rather than the IUD itself
- Screening at time of insertion greatly reduces PID risk
- Management of PID with IUD in place
- CDC does NOT recommend empirically removing IUD, as it is not the source of infection[3]
- No change in usual antibiotic treatment (ceftriaxone + azithromycin or doxycycline +/- metronidazole
- If patient has had IUD for <3 weeks, consider referring to OB/Gyn for possible removal
Other Adverse Effects
- More common with copper IUD
- Irregular menses
- Heavy vaginal bleeding
- Pelvic pain
IUD Removal
- No real indication for removal in the emergency department
- However, if patient desires removal and outpatient referral is unfeasible, can be safely removed in the ED:
- Visualize string(s) protruding from cervix
- Grasp string with Kelly clamp or long forceps
- Pull with steady, gentle force until device emerges
- Do NOT jerk string, as this may detatch string from device, making removal much more difficult
See Also
External Links
References
- ↑ Beatty MN, Blumenthal PD. The levonorgestrel-releasing intrauterine system: Safety, efficacy, and patient acceptability. Ther Clin Risk Manag. 2009;5(3):561-74.
- ↑ ../docss/family-planning-methods-2014.pdf
- ↑ ../docss/management-during-contraception_508tagged.pdf