We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Jaundice
From WikEM
For neonatal jaundice please see the Neonatal jaundice page
Contents
Background
- Bilirubin is end product of heme metabolism
- All bilirubin products in the body are initially unconjugated and is transported bound to albumin into hepatocytes t o becombined with glucuronic acid into conjugated bilirubin
- Conjugated bilirubin is then excreted into biliary tract
- Only conjugated bilirubin is water-soluble (present in urine)
- Normal bilirubin level is <1.1 (70% unconjugated)
Jaundice Types
Prehepatic (overproduction):
- Hemolysis
- Primarily unconjugated bili
Hepatic (inadequate processing):
- Viral, alcohol, toxin
- Primarily unconjugated bili
Posthepatic (underexcretion):
- Pancreatic tumor, choledocholithiasis
- Primarily conjugated bili
Clinical Features
Differential Diagnosis

Indirect Hyperbilirubinemia
- Hemolytic
- G6PD
- Drug related
- Autoimmune hemolytic anemia
- Hematoma resorption
- Ineffective erythropoiesis
- Gilbert's
Direct (Conjugated) Hyperbilirubinemia
- Choledocholithiasis
- Cholecystitis
- Ascending cholangitis
- AIDS cholangiopathy
- Stricture
- Neoplasm
- Pancreatic head
- Gallbladder
- Primary liver
- Metastatic
- Obstructing AAA
Hepatocellular damage
Patient will have severely elevated AST/ALT with often normal Alkaline Phosphatase
- Viral hepatitis
- Fulminant hepatic failure
- ETOH hepatitis
- Ischemia
- Toxins
- Isoniazid
- Phenytoin
- acetaminophen
- Ritonavir
- Halothane
- Sulronamide
- Autoimmune hepatitis
- Primary biliary cirrhosis
- HELLP Syndrome
- Congestive Hepatopathy
Pregnancy Related
- HELLP Syndrome
- Acute fatty liver
- Hyperemesis gravidarum
- Cholestasis of pregnancy
Transplant Related
Pediatric Related
- Inborn error of metabolism
- Neonatal jaundice (physiologic)
Additional Differential Diagnosis
- Reye syndrome
- TPN
- Heatstroke
- Budd-Chiari (with acute ascites)
- Wilson's disease
- Sarcoidosis
- Amyloidosis
Masqueraders
Only bilirubin stains the sclera
- Carotenemia
- Quinacrine ingestion
- Dinitrophenol, teryl (explosive chemicals)
Evaluation

- Urine pregnancy
- CBC
- Chemistry
- LFT
- Hepatocyte injury: AST, ALT, alk phos
- Hepatocyte catabolic activity: Bilirubin
- Coags
- Hepatocyte synthetic function
- Albumin
- Hepatocyte synthetic function
- Ammonia
- Hepatocyte catabolic activity
- Acute hepatitis panel
- Lipase
- Urinalysis
- ?US vs. CT
- ?Retic count
- ?Haptoglobin/LDH
- ?APAP/ASA/Utox/ETOH
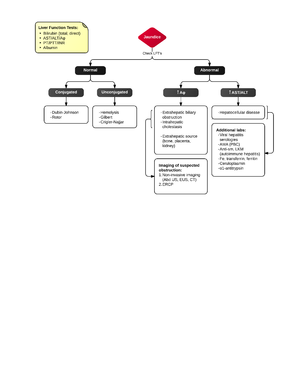
Liver function tests
Transaminases
- Transaminases in hundreds associated with mild injury; thousands suggests extensive injury
- Elevations <5x normal typical of alcoholic liver disease
- AST:ALT ratio > 2 common in acute alcoholic hepatitis (alcohol stimulates AST production)
- May be normal in end-stage liver failure
- ALT more specific marker of hepatocyte injury than AST
Alk phos
- Mild to moderate elevations accompany virtually all hepatobiliary disease
- Elevations > 4x normal suggest cholestasis
GGT
- Elevation in setting of hepatitis suggestive of alcoholic etiology
LDH
- Moderate elevations are seen in all hepatocellular disorders and cirrhosis
- Hemolysis results in elevation of LDH and unconjugated bili
Ammonia
- Elevation does NOT correlate with acute worsening of hepatic function in cirrhotic patient
- Serves as marker of generalized decline than as diagnostic tool or therapeutic end point
Coagulation Markers (PT/PTT/INR)
- Marker of synthetic function
- Correlation between PT prolongation and clinical outcome in fulminant liver disease
Albumin
- Marker of synthetic function
- Half-life is 3 weeks so less useful than PT in evaluating fulminant liver disease
- Low levels also seen in malnutrition
Management
- Management is dependent on the diagnosis of either conjugated or unconjugated hyperblirubinemia and the severity of the elevation
Disposition
New Onset Jaundice Admission Criteria
- Transaminase >1,000 IU/L
- Tbil >10mg/dL
- Evidence coagulopathy