We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Nerve Block: Median
From WikEM
Contents
Background
- Useful for lacerations across multiple fingers/palm instead of multiple digit blocks
- Useful for exploration of flexor tendons of digits 1-3
- Ultrasound guidance significantly increases the success rate of this block [1]
Indications
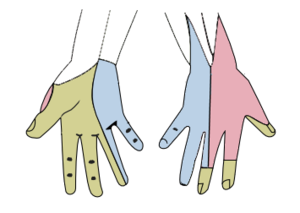
- Trauma or need to perform painful procedure on area innervated by median nerve
Contraindications
- Infection overlying injection site
- Previous allergic reaction to local anesthesic used
- Distortion of anatomic landmarks
Equipment Needed
- Topical anesthesia (LET, EMLA)
- local anesthesia
- Lidocaine 1% (lasts 30-60 minutes or longer if given with epinephrine, rapid onset)
- Mepivacaine 3% (lasts 45-90 minutes, slower onset)
- Bupivacaine 0.5% (lasts 2-4 hours, slowest in onset)
- 18G needle to draw up anesthetic
- 25-30G needle to inject. Use of a larger gauge (21-23) makes it easier to see the needle on ultrasound
- 10 cc syringe
- Gauze pads
- ultrasound probe cover or tegaderm to cover probe surface
Procedure
- Time out, confirm correct patient and laterality
- Apply topical anesthesia if needed
- Draw up 5-10 mL of anesthetic into syringe
- Beware of toxic dose of anesthetic you're using Local Anesthetic Systemic Toxicity (LAST)
- Before any nerve block, perform neurovascular exam (often includes 2 patient discrimination with paperclip)
Wrist Block
- Median nerve is within the carpal tunnel
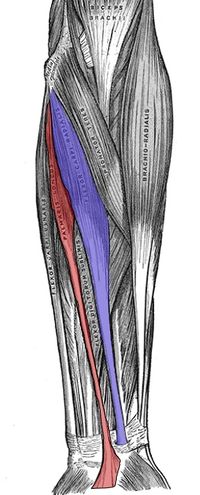
- Between palmaris longus and flexor carpi radialis
- Insert needle perpendicular between tendons, 2-3 cm proximal to the distal crease of the wrist
- Aspirate; if no blood inject a few mL's of anesthetic slowly
- Test sensation to pain distal to block
Elbow Block

- Cleanse the skin overlying the antecubital fossa with chosen antiseptic
- Create a sterile field using sterile drape
- In a sterile fashion, apply a small wheel of local anesthetic to the area immediately proximal to the antecubital fossa
- Palpate the brachial artery to be aware of its path
- The median nerve should be approximately 1 cm medial to the brachial artery at this point
- Insert the needle approximately 1-2 cm proximal to the flexor crease and advance with negative pressure applied to the syringe
- At 1-2 cm deep, aspirate prior to injection to rule out intravascular placement
- Inject 5-10 mL of local anesthetic
Ultrasound Guided Block
- Place a linear probe on the volar aspect of the midforearm
- It may be easier to find the nerve by starting with the probe over the volar wrist and sliding proximally. The tendons will disappear as they become muscles but the nerve will remain as the only continuous round structure.
- The median nerve takes the appearnce of a "chocolate chip cookie" in the axial orientation and lies between the flexor digitorum profundus and supeficialis
- Clean and prep the patient's arm under sterile conditions, and insert a 25 g needle in the long axis under ultrasound guidance next to the nerve
- Aspirate to prevent inadvertent intravascular injection
- Inject 5 mL of local anesthetic so that it basks the nerve
Complications
- Bleeding
- Infection
- Pain
- Needle fracture
- Neurapraxia
See Also
External Links
References
- ↑ Liebmann O, Price D, et al. [Feasibility of Forearm Ultrasonography-Guided Nerve Blocks of the Radial, Ulnar, and Median Nerves for Hand Procedures in the Emergency Department]. Ann Emerg Med 2006; 48(5):558-62.