We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Acute rheumatic fever
From WikEM
(Redirected from Rhumatic fever)
Contents
Background
- Primarily affects school age children 2-6wk after strep pharyngitis
- Connective tissue of heart, joints, CNS, subq tissues are targeted by immune reaction
Clinical Features
- Polyarthritis
- Most common symptom (75%)
- Migratory, fleeting polyarticular arthritis primarily affecting large joints
- Carditis (33%)
- Most serious complication and second most common
- New murmur, pericardial rub, CHF
- Most serious complication and second most common
- Chorea (10%)
- May appear months following strep infection, may be sole manifestation of RF
- Erythema marginatum
- Persists only for several days
- Usually coexists with presence of carditis in some form
- Nonpruritic, located on trunk and proximal limbs, never on face
- Nodules
- Located on extensor surfaces of wrists, elbows, knees
Differential Diagnosis
- Kawasaki Disease
- Viral or other forms of cardiomyopathy
- Leukemia
- Vasculitis (HSP, drug reaction)
Pediatric hip pain
- Septic arthritis of the hip (peds)
- Slipped capital femoral epiphysis
- Legg-Calve-Perthes disease
- Transient (toxic) synovitis
- Acute rheumatic fever
- Juvenile idiopathic arthritis
- Developmental dysplasia of hip
- Femur fracture
Polyarthritis
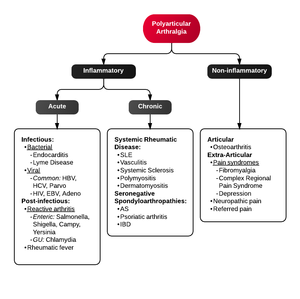
- Fibromyalgia
- Juvenile idiopathic arthritis
- Lyme disease
- Osteoarthritis
- Psoriatic arthritis
- Reactive poststreptococcal arthritis
- Rheumatoid arthritis
- Rheumatic fever
- Serum sickness
- Systemic lupus erythematosus
- Serum sickness–like reactions
- Viral arthritis
Evaluation
Work-Up
Modified Jones Criteria (1992) for Acute Rheumatic Fever
REQUIRE: 2 major or 1 major and 2 minor criteria and evidence of previous GAS pharyngitis
- Major diagnostic criteria
- Carditis (new or changing murmur, cardiomegaly, CHF, pericarditis)
- Migratory polyarthritis (typically affects knees, ankles, elbows, wrists)
- Chorea (abrupt, purposeless movements)
- Subcutaneous nodules (painless, firm, usually over bones/tendons)
- Erythema marginatum (non-pruritic, trunk/extremities, with facial sparing)
- Minor diagnostic criteria
- Fever
- Arthralgia
- History of previous attack of rheumatic fever
- Prolonged PR interval
- Elevated ESR, CRP
- Evidence of preceding streptococcal infection
- Increased ASO or other strep ab
- Positive throat culture for Group A strep
- Positive rapid GAS
- Recent scarlet fever
Management
- Penicillin
- Indicated for all with rheumatic fever even if culture for strep is negative
- 600K units IM if <27 kg
- 1.2 million units IM if >27 kg
- Penicillin V PO x10d
- Prophylaxis
- 5yr if no cardiac involvement, lifetime if cardiac involvement
- Pen G IM q month or oral penicillin daily
- Erythromycin x10d if pen allergic
- Arthritis
- High-dose aspirin therapy (75-100mg/kg/d)
- Carditis
- Prednisone 1-2mg/kg/d
- Chorea
- Haloperidol 0.01-0.03mg/kg/d in four divided doses
Disposition
- Admit for confirmation of diagnosis
See Also
References
- Horeczko T, Inaba AS: Cardiac Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. St. Louis, Mosby, Inc., 2014, (Ch) 171: p 2139-2170.
- Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Associa