We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
STEMI equivalents
From WikEM
Contents
Background
- Standard teaching for STEMI typically has the following criteria[1]
- ≥1 mm (0.1 mV) of ST segment elevation in the limb leads
- ≥ 2 mm elevation in the precordial leads and present in anatomically contiguous leads
- There are several variations from the classic STEMI ECG changes that do not fit this definition
STEMI Equivalents
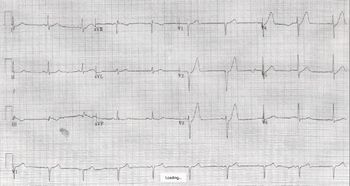
Posterior MI
- RCA (90%), LCA (10%)
- 12-Lead ECG findings[2]
- ST-segment depression (horizontal >> downsloping/upsloping)
- Prominent and broad R wave (>30ms)
- Relative tall R waves in precordial leads (may find R = S amplitude in V1)
- R/S wave ratio >1.0 in lead V2
- Prominent, upright T wave
- Combination of horizontal ST-segment depression with upright T wave
- Posterior ECG or 15-lead ECG may be helpful
- V7: Left posterior axillary line along the 5th ICS
- V8: Tip of the left scapula line along the 5th ICS
- V9: Left paraspinal area line along the 5th ICS
- Posterior ECG findings
- ≥1 mm ST-segment elevation
LMCA Occlusion
- Seen with occlusion or near-occlusion of the left main artery[3]
- Has been reported in occlusion of the proximal left anterior descending artery and severe multivessel coronary artery disease
- 12-Lead ECG findings
- ST elevation in aVR ≥ 1mm
- ST elevation in aVR ≥ V1
- ST depression typically seen in lateral
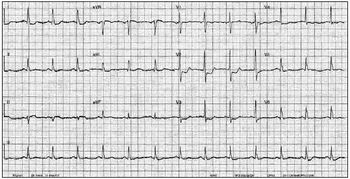
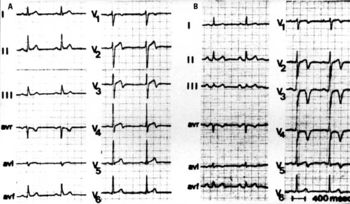
De Winter’s T Waves
- Suggestive of proximal LAD lesion
- 12-Lead ECG findings[4]
- Precordial ST-segment depression at the J-point
- Tall, peaked, symmetric T waves in the precordial leads
- Lead aVR shows slight ST-segment elevation in most cases
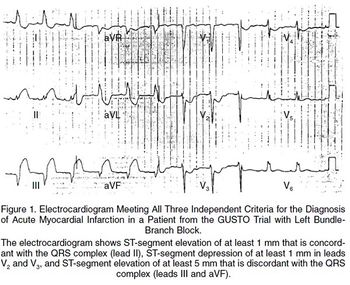
Sgarbossa's Criteria
- Used to identify STEMI in the setting of LBBB or pacemaker
- Original Criteria[5]
- ≥3 points = 98% probability of STEMI
- ST elevation ≥1 mm in a lead with upward (concordant) QRS complex - 5 points
- ST depression ≥1 mm in lead V1, V2, or V3 - 3 points
- ST elevation ≥5 mm in a lead with downward (discordant) QRS complex - 2 points
- Smith's modification[6]
- Changes the 3rd rule of original Sgarbossa's Criteria to be ST depression OR elevation discordant with the QRS complex and with a magnitude of at least 25% of the QRS increases Sn from 52% to 91% at the expense of reducing Sp from 98% to 90%[
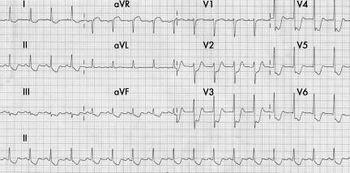
Wellens’ Syndrome
- ECG findings in absence of chest pain, but with recent cardiac chest pain symptoms
- Represents critical stenosis of the LAD
- Not necessarily STEMI equivalent but will require PCI in the next 24-48hr
- 12-Lead ECG findings[7]
- Deeply-inverted or biphasic T waves in V2-3
- Isoelectric or minimally-elevated ST segment (<1 mm)
- Absent precordial Q waves with preserved R waves
- Two T wave characteristics:
- Type A: Biphasic pattern - 25% - Biphasic T-waves (initial + deflection and terminal - deflection)
- Type B: Inversion pattern - 75% - Deeply inverted and symmetric T-waves
No Longer STEMI Equivalents
New LBBB
- New LBBB alone is no longer a reason to activate the cath lab[8]
- However, careful workup for ACS should be taken for symptomatic patients with LBBB
- 12-Lead ECG findings
- QRS > 0.12 in limb leads
- Leads
- Large and wide R waves — leads I, aVL, V5, and V6
- Small R wave followed by deep S wave —leads II, III, aVF, V1–V3

External Links
See Also
References
- ↑ ECC Committee, Subcommittees and Task Forces of the American Heart Association.. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care — Part 8: Stabilization of the Patient With Acute Coronary Syndromes. Circulation. 2005. 112 (24_suppl):IV–89–IV–110. 2005.
- ↑ Van Gorselen EO, et al. Posterior myocardial infarction: the dark side of the moon. Neth Heart J. 2007; 15:16-21.
- ↑ Hennings JR and Fesmire FM. A new electrocardiographic criteria for emergent reperfusion therapy. Am J Emerg Med. 2012; 30(6):994–1000.
- ↑ de Winter R, et al. A new ECG sign of proximal LAD occlusion. NEJM. 2008; 359:2071–2073.
- ↑ Sgarbossa E, et al.. "Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators". NEJM. 1996; 334(8):481-7.
- ↑ Smith, S, et al. Diagnosis of ST-Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block With the ST-Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. 60(6):766-776.
- ↑ Rhinehardt J, et al. Electrocardiographic manifestations of Wellens' syndrome. Am J Emerg Med. 2002; 20(7):638-43.
- ↑ Jain S, et al. Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction. Am J Cardiol. 2011; 107:1111-1116.