Thromboelastography (TEG)
- Lack of evidence strongly suggests that these tests currently should be used ONLY FOR RESEARCH purposes in regards to trauma-induced coagulopathy.[1]
Contents
Background
Tromboelastogram (TEG or formerly ROTEM) is used to identify acute coagulopathies in both traumatic and nontraumatic patients. This may enable focused use of blood products during resuscitation. It quantifies the interaction of platelets with the coagulation cascade (aggregation, clot strengthening, fibrin cross linking and fibrinolysis). 0.36mL of clotted blood from the patient is spun in a small cup with changes in the clot strength recorded electrically.
There are Two commercial types of viscoelastic tests are available:
- Thromboelastography =TEG
- Rotational thromboelastogram = ROTEM
Heparinase to deactivate heparin is now employed in the TEG(r) technology to prevent interference from heparin in samples[2]
Nomenclature Differences for ROTEM
Although TEG and ROTEM measure the same coagulation functions there is a different naming convention for each device.
| ROTEM | TEG |
| Clotting time (CT) | R value (reaction time) |
| α angle and clot formation time (CFT) | K value and α angle |
| Maximum clot firmness (MCF) | Maximum amplitude (MA) |
| Clot lysis (CL) | LY30 |
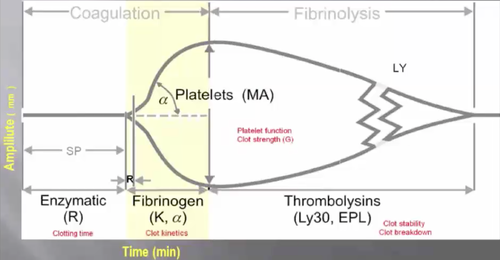
Features of a TEG Curve
Initiation (R)
Represents period of time of latency from start to initial fibrin formation due to effects of Factor VIIa and Tissue Factor.
Amplification (K)
Represents time taken to achieve a certain level of clot strength due to thrombin and activation of platelets (where r-time = time zero)
Propagation (α-Angle)
Measures the speed at which fibrin build-up and cross-linking takes place (clot strengthening), and hence assesses the rate of clot formation.
Maximum Amplitude (MA)
A function of the maximum dynamic properties of fibrin and platelet bonding via GPIIb/IIIa and represents the strongest point of fibrin clot and correlates to platelet function: 80% platelets; 20% fibrinogen.
Clot stability (LY 30%)
This is percentage decrease in amplitude 30 minutes post-MA and gives measure of degree of fibrinolysis
Normal Values[3]
- R: 4-8 min
- K: 1-4 min
- α-Angle: 47-74°
- MA: 55-73mm
- LY 30%: 0-8%
Abnormal Values
Prolonged R
- Factor deficiency (ie hemophilia)
- Treat with FFP or protamine
Prolonged K/Reduced α-Angle
- Fibrinogen deficiency (ie DIC)
- Treat with cryoprecipitate
Reduced MA
- Thrombocytopenia, platelet dysfunction (ie patient on clopidogrel)
- Treat with platelets or DDAVP
Elevated LY 30%
- Rapid clot lysis (ie tPA given)
- Treat with TXA
TEG Diagram
See Also
External Links
References
- ↑ Hunt H, Stanworth S, Curry N, Woolley T, Cooper C, Ukoumunne O, Zhelev Z, Hyde C. TEG and ROTEM for diagnosing trauma‑induced coagulopathy (disorder of the clotting system) in adult trauma patients with bleeding. Cochcrane Review. 16 February 2015
- ↑ Milind Thakur, Aamer B Ahmed. A Review of Thromboelastography. International Journal of Perioperative Ultrasound and Applied Technologies, January-April 2012;1(1):25-29 Fulltext]
- ↑ Walsh M, Thomas SG, Howard JC, et al. Blood component therapy in trauma guided with the utilization of the perfusionist and thromboelastography. Journal of Extra-Corporeal Technology. 2011 Sep; 43(3):162-7.
{kind=link}