We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Umbilical vein catheterization
From WikEM
Contents
Indications
- Emergency access and stabilization of the newly born with lack of peripheral access
- Remains viable and patent until ~1 week after birth[1]
Contraindications
- Omphalitis
- Peritonintis
- Necrotizing enterocolitis
Equipment Needed
- Fluid chamber, IV tubing, infusion pump, filter (0.22 µm), short length of IV tubing, three-way stopcock
- Umbilical catheter (3.5 to 5 Fr)
- 3-0 silk suture on a curved needle
- Curved iris forceps without teeth
- Small clamps, forceps, scissors, needle holder
- 10 mL of heparinized solution for flush (1–2 units heparin per milliliter of fluid)
- Sterile drapes, surgical cap, mask, gown, and gloves
Procedure
- Place patient under warmer
- Hold umbilical stump and scrub with betadine (avoid pooling at patient's sides secondary to to blistering under warmer
- Drape in sterile fashion (leave head exposed for observation)
- Flush catheter (3.5 Fr for preterm to 5 Fr for term newborns and attach to three-way stopcock)
- If emergency and UVC kit not available, consider 3.5 Fr ≈ 18.5 gauge and 5 Fr ≈ 16 ga[2]
- Grab long angiocaths and remove from needle in sterile fashion
- Place purse string suture or umbilical tape at jct of skin and cord to provide hemostasis and to secure line
- Cut cord with scalpel 1 cm from skin
- Identify the vein (larger, thin walled vessel usually at 12 o'clock position that continues to bleed. usu 2 arteries, 1 vein)
- Feed the "mouth"
- Gently dilate catheter with forceps, clearing thrombus
- Gently advance catheter until blood returns and then advance 1-2 cm more (usually a total of 4-5 cm in term infant)
- Secure the catheter using the purse string or umbilical tape and then secure to the patient
- The catheter can be advanced to the IVC using a standardized graph, if CVP monitoring or high concentrations of glucose are indicated
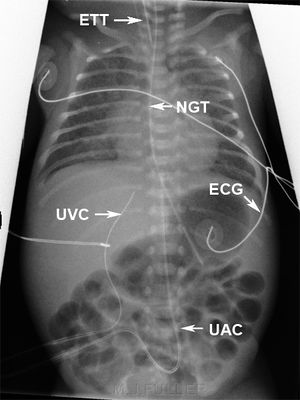
- Confirm catheter location radiographically[3][4]
- Travels cephalad until passing through ductus venosus
- In contrast, umbilical arterial catheters travel down into iliac arteries and then cephalad

Complications
- Hemorrhage
- Infection
- Hepatic necrosis (secondary to to injection of sclerosing solutions)
- Air embolism (especially on removal of catheter)
- Catheter tip embolism
- Vessel perforation
See Also
References
- ↑ Butler-O'Hara M, Buzzard CJ, Reubens L, McDermott MP, DiGrazio W, D'Angio CT. A randomized trial comparing long-term and short-term use of umbilical venous catheters in premature infants with birth weights of less than 1251 grams. Pediatrics. 2006 Jul. 118(1):e25-35.
- ↑ Ahn W, Bahk JH, Lim YJ. "The “Gauge” System for the Medical Use." Anesthesia & Analgesia. October 2002. 95(4): 1125.
- ↑ Hoellering AB, Koorts PJ, Cartwright DW, Davies MW. Determination of umbilical venous catheter tip position with radiograph. Pediatr Crit Care Med. 2014 Jan. 15(1):56-61.
- ↑ Vali P, Fleming SE, Kim JH. Determination of umbilical catheter placement using anatomic landmarks. Neonatology. 2010. 98(4):381-6.
Authors
Matthew, Kevin Lu, Ross Donaldson, Neil Young, Daniel Ostermayer, Claire