We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
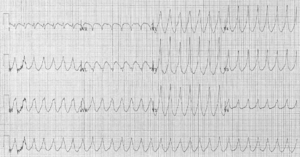
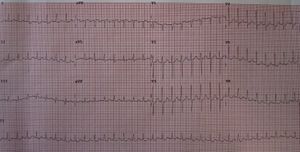
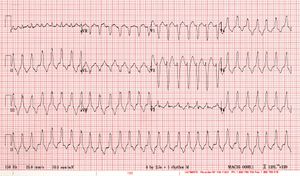
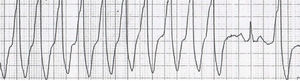
V Tach vs. SVT
From WikEM
Assume ventricular tachycardia until proven otherwise
Contents
Background
- Ventricular tachycardia vs. supraventricular tachycardia
Evaluation

| Factor |
V-Tach | SVT with Aberrancy |
| Age | >50 | <35 |
| History | MI, CHF, CABG, MVR | MVR, WPW |
| Cannon A Waves | Present | Absent |
| Arterial Pulse | Variation | No variation |
| First heart sound | Variable | Not variable |
| Fusion Beats | Present | Absent |
| AV dissociation | Present | Absent |
| QRS | >0.14sec | <0.14sec |
| Axis | Extreme LAD (< -30) | Normal or slightly abnormal |
| Vagal Maneuvers | No response | Slows or terminates |
|
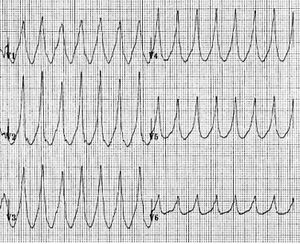
QRS morphology (RBBB-like pattern) |
V1 - R or qR V6 - rS |
V1 - rsR' V6 - R(slurredS) |
|
QRS morphology (LBBB-like pattern) |
V1 or V2 - Broad R wave (>40msec) V6 - Any Q or QS |
V1 - rS or QS V6 - qRs |
Diagnostic Algorithms
- Only for regular rhythms, if irregular consider a-fib with block
- Only for treatment decision if patient is stable
- Assume V-tach until proven otherwise
Brugada Algorithm
- Absence of an RS complex in all precordial leads?
- If yes then VT
- If no then continue
- RS interval >100ms in any precordial lead? (onset of R wave to deepest part of S wave)
- If yes then VT
- If no then continue
- AV dissociation?
- If yes then VT
- If no then continue
- Morphology criteria for v-tach present in both V1-2 and V6?
- If yes then VT
- If no then possibly SVT with aberrant conduction
aVR Algorithm
- In lead aVR:
- Presence of an initial R wave?
- If yes then VT
- If no then continue
- Presence of an initial r or q wave >40ms
- If yes then VT
- If no then continue
- Presence of a notch on descending limb of a negative onset, predominantly negative QRS?
- If yes then VT
- If no then continue
- Ventricular activation-velocity ratio (Vi/Vt) ≤1?
- If yes then VT
- If no then SVT
Niemann Algorithm[1]
- Combination of the most specific aspects of the above two algorithms
Acronym: CARMA → Concordance → aVR →Regular → Morphology →AV dissociation
- Presence of an initial R wave in aVR? [2][3]
- If yes then VT
- If no then continue
- Is there concordance (monophasic with same polarity) in all of the precordial leads? [4]
- If yes then VT
- If no then continue
- Is there evidence of AV dissociation/Capture beats?
- If yes then VT
- If no then continue
- Is the QRS morphology in V1 and V6 consistent with either LBBB or RBBB? [5][6]
- If no then VT
- If yes then SVT with aberrancy
R-Wave Peak Time Method
- In lead II, if the TIME in (ms) it takes the R wave to go from the isoelectric line to its peak voltage is greater than 50ms, it is VT
- Positive Likelihood ratio of 34.8
Lesser Known Criteria
- Josephson's sign --- notching or slurring near the nadir of the S-wave is characteristic of V. Tach
- Rsr' sign --- A taller left R wave in v1-v2 is very specific for VT, as opposed in a RBBB where the second/right R-wave (R') is taller
- "Northwest" axis deviation -- Negative QRS complex in I, AVF and Positive QRS in AVR

See Also
References
- ↑ James Niemann MD FACEP is EM Faculty at Harbor-UCLA Medical Center and prominent resuscitation researcher
- ↑ Vereckei A et al. New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachy- cardia. Heart Rhythm 2008; 5:89-98
- ↑ Szelenyi Z, et al. Acad Emerg Med 2013;20:1121- 1130
- ↑ Brugada P et al. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation 1991;83:1649-1659
- ↑ Brugada, Circulation; Griffith MJ et al. Lancet 1994;343:386-388
- ↑ Wellens HJJ et al. Am J Med 1978; 64:27-33