

A History of Anthrax
 ShareCompartir
ShareCompartir
Throughout history, from biblical times to modern day, many sicknesses have been described with symptoms that resemble anthrax. Although we cannot know for sure whether these earliest reports of illness were, in fact, anthrax, many researchers believe that they were.
Naturally Occurring Anthrax
700 BC - Ancient origins of anthrax
Moschophoros (Calf Bearer), a statue by Phaidimos Moschophoros by Phaidimos
Anthrax is thought to have originated in Egypt and Mesopotamia. Many scholars think that in Moses’ time, during the 10 plagues of Egypt, anthrax may have caused what was known as the fifth plague, described as a sickness affecting horses, cattle, sheep, camels and oxen.
Ancient Greece and Rome were also well acquainted with anthrax, and this is illustrated in many of the ancient writings of the most famous scholars from those times. For example, many scholars think anthrax was depicted by Homer in The Iliad, written around 700 BC, and in poems by Virgil, who lived from 70-19 BC. Some even suggest that anthrax may have contributed to the fall of Rome.
1700s - First clinical descriptions of anthrax
 The first clinical descriptions of cutaneous anthrax were given by Maret in 1752 and Fournier in 1769. Before this, anthrax had only been described through historical accounts.
The first clinical descriptions of cutaneous anthrax were given by Maret in 1752 and Fournier in 1769. Before this, anthrax had only been described through historical accounts.
1877 - Robert Koch uses anthrax to develop his famous Koch Postulates
Bacteriologist Robert Koch in his laboratory Bacteriologist Robert Koch in his laboratory
Scientist Robert Koch studied Bacillus anthracis, the bacterium that causes anthrax. He discovered that the bacteria formed spores and were able to survive for very long periods of time and in many different environments. Koch decided to use anthrax bacteria in one of his most important historical experiments, in which he isolated and grew Bacillus anthracis in pure culture and injected animals with the bacteria. Using what he observed in this study, he described how the microbe he injected into the animals caused the disease. From these studies, he was also able to determine the life cycle of the anthrax bacteria, and was able to demonstrate what became known as Koch’s postulates, which demonstrate a causal relationship between a specific microorganism and a disease.
1800s - Many significant scientific discoveries
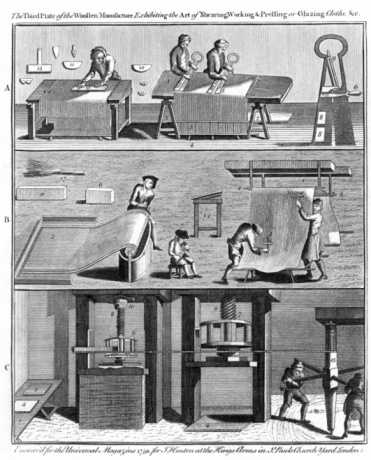
Art depicting sequence of wool production Art depicting sequence of wool production
During the 1800s, doctors saw cases of anthrax but did not yet have a diagnosis for the disease. During this time, the organism that causes anthrax had not yet been discovered, but doctors had noticed a link between the disease and the animal hair industry. Because of this, the disease became known as “wool sorters disease.” By the middle of the century, early researchers had associated the disease with the presence of rod-shaped bodies that were seen in the blood of infected animals. These bodies were eventually identified as bacteria and given the name Bacillus anthracis.

1881 - Louis Pasteur creates the first vaccine for anthrax

French Chemist Louis Pasteur
Louis Pasteur, another prominent scientist, took Koch’s work a step further, trying to fully prove how anthrax was spread and how it made people or animals sick. Pasteur also worked to create a vaccine for anthrax. In his experiment, Pasteur gave 25 animals two shots of an anthrax vaccine he had created with weakened anthrax bacteria. After he gave both rounds of the vaccine to these animals, he injected them with live anthrax bacteria. He also injected live bacteria into 25 other animals that had not been vaccinated. Each of the vaccinated animals survived, while the 25 that were not vaccinated died.
1900s - Anthrax well documented in the U.S., but undocumented in other countries
Much knowledge was gained about anthrax in the 1800s. As a result, animal and human cases of anthrax in the United States, Britain, and Germany were well documented in the early 1900s. However, there were still places where anthrax cases hadn’t been documented, such as Russia, Asia, India and Africa. Because of the high number of contaminated animal products imported from these countries, however, it was known that anthrax had to be widespread in these regions.
1937 - Anthrax vaccine for animals reduces anthrax cases in humans
 Max Sterne successfully created the anthrax live spore vaccine for animals. This vaccine is still used in animals in most countries. Because of the introduction of routine vaccination of animals against anthrax and the improvements in animal product processing procedures, the number of cases of anthrax in humans declined. This decline was so significant that during the entire 20th century there were only 18 cases of inhalation anthrax in the United States.
Max Sterne successfully created the anthrax live spore vaccine for animals. This vaccine is still used in animals in most countries. Because of the introduction of routine vaccination of animals against anthrax and the improvements in animal product processing procedures, the number of cases of anthrax in humans declined. This decline was so significant that during the entire 20th century there were only 18 cases of inhalation anthrax in the United States.
1944 - Penicillin used to treat anthrax
Penicillin had been discovered in 1928, but it wasn’t until 1944 when it was first used to treat anthrax. Penicillin became the drug of choice for treating anthrax, and it replaced all previous therapies, such as serum therapies and chemotherapies.
1950s - The first anthrax vaccine for humans is created
 The first anthrax vaccine for humans was created. This anthrax vaccine was tested in a group of goat hair mill workers. Volunteers were given either the vaccine or a placebo (a shot that does not have the vaccine in it). The volunteers were then followed over a 2-year period. This study determined that the vaccine was 92.5% effective in preventing cutaneous anthrax. After the study, the vaccine was made available to people working in goat hair processing mills in the United States.
The first anthrax vaccine for humans was created. This anthrax vaccine was tested in a group of goat hair mill workers. Volunteers were given either the vaccine or a placebo (a shot that does not have the vaccine in it). The volunteers were then followed over a 2-year period. This study determined that the vaccine was 92.5% effective in preventing cutaneous anthrax. After the study, the vaccine was made available to people working in goat hair processing mills in the United States.
1970 - New human vaccine released
An updated human anthrax vaccine was released, replacing the 1950s vaccine. This is essentially the same vaccine used today.
2006 - New York City drum maker diagnosed with inhalation anthrax
 A drum-maker from New York City got sick while on tour with a dance troupe in Pennsylvania. He had just returned from Africa with four goat skins that he planned to use to make drums. He said that when he processed the goat skins to remove the hair, he did not use chemicals on the skins to kill germs or wear protection while handing the skins. He also reported that while he processed the skins, hair and dust particles floated into the air. Four days after he last had contact with the goat skins, he began having breathing problems and was hospitalized. Five days later he was diagnosed with inhalation anthrax. Public health investigators determined he had been exposed to anthrax while processing the goat skins he brought home from Africa. When he scraped the hair from the skins, the anthrax spores were released into the air and he breathed them in. The spores got into his lungs and caused him to become ill. It was the first time in 30 years that a case of naturally acquired anthrax was reported in the United States.
A drum-maker from New York City got sick while on tour with a dance troupe in Pennsylvania. He had just returned from Africa with four goat skins that he planned to use to make drums. He said that when he processed the goat skins to remove the hair, he did not use chemicals on the skins to kill germs or wear protection while handing the skins. He also reported that while he processed the skins, hair and dust particles floated into the air. Four days after he last had contact with the goat skins, he began having breathing problems and was hospitalized. Five days later he was diagnosed with inhalation anthrax. Public health investigators determined he had been exposed to anthrax while processing the goat skins he brought home from Africa. When he scraped the hair from the skins, the anthrax spores were released into the air and he breathed them in. The spores got into his lungs and caused him to become ill. It was the first time in 30 years that a case of naturally acquired anthrax was reported in the United States.
2009 - A woman in Connecticut was diagnosed with Gastrointestinal anthrax
 A woman in Connecticut was diagnosed with gastrointestinal anthrax. Public health investigators learned that the woman had participated in a drumming event the day before she became ill. The drums used at the event and the event space were all tested for contamination with anthrax spores. Two animal skin drums were found to have anthrax spores on them, and spores were also found in the room where the drumming took place, and in other rooms in the building. Investigators determined that the spores were released into the air while the contaminated drums were played. After 2 months in the hospital, the woman recovered and was released from the hospital.
A woman in Connecticut was diagnosed with gastrointestinal anthrax. Public health investigators learned that the woman had participated in a drumming event the day before she became ill. The drums used at the event and the event space were all tested for contamination with anthrax spores. Two animal skin drums were found to have anthrax spores on them, and spores were also found in the room where the drumming took place, and in other rooms in the building. Investigators determined that the spores were released into the air while the contaminated drums were played. After 2 months in the hospital, the woman recovered and was released from the hospital.
2010 - A new form of anthrax
 Early in 2010, a small outbreak of anthrax occurred in the United Kingdom and Germany. All of the patients who came to the hospital were illicit drug users who had used heroin before having symptoms. Anthrax in these patients did not look like typical cutaneous anthrax. Many had swelling and infection of the deeper layers of skin but they didn’t have a raised sore with a black center – the tell-tale sign of cutaneous anthrax. Doctors recognized this anthrax as a new type of anthrax, calling it injection anthrax. Doctors wondered where the anthrax spores came from and how they were injected into the drug users. While no anthrax was found in the heroin itself, the evidence gathered by epidemiologists strongly suggested that was anthrax was in the heroin. Public health officials believe that the anthrax spores were in the heroin and that when the patients injected the drug into their bodies, they also injected anthrax spores.
Early in 2010, a small outbreak of anthrax occurred in the United Kingdom and Germany. All of the patients who came to the hospital were illicit drug users who had used heroin before having symptoms. Anthrax in these patients did not look like typical cutaneous anthrax. Many had swelling and infection of the deeper layers of skin but they didn’t have a raised sore with a black center – the tell-tale sign of cutaneous anthrax. Doctors recognized this anthrax as a new type of anthrax, calling it injection anthrax. Doctors wondered where the anthrax spores came from and how they were injected into the drug users. While no anthrax was found in the heroin itself, the evidence gathered by epidemiologists strongly suggested that was anthrax was in the heroin. Public health officials believe that the anthrax spores were in the heroin and that when the patients injected the drug into their bodies, they also injected anthrax spores.
2011 - A medical victory remains a medical mystery

Dan Anders had a close-call with inhalation anthrax. His wife, Anne (in the background) calls him “Miracle Man.” Photo courtesy of the Star Tribune/Minneapolis-St. Paul, 2013
A retired Florida man and his wife traveled for 3 weeks on a cross-country trip that took them through Wyoming, Montana and the Dakotas. They visited many state parks. The man got sick when they arrived in Minnesota. He went to the emergency room complaining of flu-like symptoms and was originally diagnosed with community-acquired pneumonia. A doctor, who had grown up on a cattle farm and was familiar with anthrax, felt that this diagnosis was not right and ordered more tests. The tests found bacteria in his blood that looked like anthrax bacteria. The samples of his blood were then sent to the Minnesota Public Health laboratory, where his anthrax illness was confirmed.
Because the doctors at the hospital were able to quickly diagnose anthrax, the patient got treatment immediately, including a specialized antitoxin (anthrax immunoglobulin) rushed in by the Centers for Disease Control and Prevention. After 3 weeks in the hospital, the patient fully recovered and was sent home.
A case of naturally occurring inhalation anthrax is very rare in the United States, so to rule out any possible bioterrorism threats, the FBI was called in to investigate the case. The FBI determined that the man had inhaled the anthrax spores in a natural environment and there was no threat to anyone else.
Anthrax Used as a Biological Weapon
1800s - Scientific discoveries led to more knowledge of how to grow specific germs
Portrait of Robert Koch Portrait of Robert Koch
The work of scientist Robert Koch in the 1800s led to the development of more modern microbiology experiments. This increase in more sophisticated experiments also created the knowledge of how to grow and produce large stocks of specific germs.
1900s - First deliberate use of anthrax as an act of aggression
 The first deliberate uses of anthrax as an act of aggression were recorded in the early decades of the 1900s, during World War I.
The first deliberate uses of anthrax as an act of aggression were recorded in the early decades of the 1900s, during World War I.
1914-1918 Anthrax used during the first World War
 There is evidence that the German army used anthrax to secretly infect livestock and animal feed traded to the Allied Nations by neutral partners. An example of this undercover biological warfare was the infection of Argentinian livestock intended for trade with the allied forces, resulting in the death of 200 mules in 1917 and 1918.
There is evidence that the German army used anthrax to secretly infect livestock and animal feed traded to the Allied Nations by neutral partners. An example of this undercover biological warfare was the infection of Argentinian livestock intended for trade with the allied forces, resulting in the death of 200 mules in 1917 and 1918.
1925 - A diplomatic approach to limit the use and creation of germ and chemical warfare
After the many chemical and biological horrors of WWI, a diplomatic attempt was made to limit the use and creation of this kind of warfare. The Geneva Protocol for the Prevention of the Use in War of Asphyxiating, Poisonous or other Gases and Bacteriological Methods of Warfare was created. This treaty was a great step in trying to stop the use of biologic agents during war. However, it did not specifically outlaw the research or production of biologic agents. Many countries agreed to the treaty but then created amendments to allow for use of biologic weapons during retaliation.After the Geneva Convention, interest in anthrax mostly focused on preventing disease in livestock and on improving the Pasteur vaccine.
1932 - Japan experimenting with anthrax as a weapon
 Japan began producing anthrax to be used as a weapon and conducted research with biological weapons in Japanese-occupied Manchuria. During this time, prisoners were infected with anthrax and other deadly diseases. It was later discovered that during this program, the Japanese attacked at least 11 Chinese cities with anthrax and other biological agents by spraying them directly onto homes from aircraft.
Japan began producing anthrax to be used as a weapon and conducted research with biological weapons in Japanese-occupied Manchuria. During this time, prisoners were infected with anthrax and other deadly diseases. It was later discovered that during this program, the Japanese attacked at least 11 Chinese cities with anthrax and other biological agents by spraying them directly onto homes from aircraft.
1942 - United States and Great Britain experiment with bioweapons

Gruinard bay in Scotland Gruinard Bay, Scotland
A bioweapons program was started in the United States. The United States conducted experiments with anthrax, among other biologic agents, at testing sites in Mississippi and Utah. More than 5,000 bombs were filled with anthrax in preparation for a response to any possible attacks from Germany.
Great Britain also began to experiment with anthrax for bioweapons on a small island off the coast of Scotland called Gruinard Island. They tested the widespread release of anthrax by releasing bombs containing the germ over the island, where 80 sheep had been placed. All of the sheep died from anthrax. One of the most important findings from this experiment was how long anthrax stays in the environment after a release. The island remained uninhabitable until 1986, when Great Britain decided to decontaminate it by killing all of the anthrax spores. After a year of soaking the island in a mixture of formaldehyde and seawater, the island was considered disinfected.
1950 - U.S. bioweapon programs are expanded
During the Korean War, U.S. bioweapon programs were expanded. This expansion included the creation of a program to develop vaccines and treatments to protect troops against biological agents.
1960s - Growing international concern about the use of bioweapons
 By 1960, the United States possessed a large collection of bioweapons, including many types of bacteria, fungi, and toxins. During the late 1960s, there was growing concern, internationally, about the use of biological weapons and the ineffectiveness of the Geneva Protocol. In July of 1968, Great Britain submitted a proposal to the Committee on Disarmament of the United Nations, which would prohibit the development, production, and stockpiling of biological agents. This proposal also outlined the need for inspections for alleged violators. Several months later, The Warsaw Pact nations submitted a similar proposal. In 1969, President Nixon terminated the U.S. bioweapons program through an executive order. This executive order stopped offensive bioweapon research and production of the weapons, and it also called for destruction of the arsenal. The United States also adopted the policy to never use any biological or toxic weapons under any circumstances. After this, research efforts in the United States became solely directed toward the creation of defensive methods like vaccines, treatments, and diagnostic tests for potential biologic threats.
By 1960, the United States possessed a large collection of bioweapons, including many types of bacteria, fungi, and toxins. During the late 1960s, there was growing concern, internationally, about the use of biological weapons and the ineffectiveness of the Geneva Protocol. In July of 1968, Great Britain submitted a proposal to the Committee on Disarmament of the United Nations, which would prohibit the development, production, and stockpiling of biological agents. This proposal also outlined the need for inspections for alleged violators. Several months later, The Warsaw Pact nations submitted a similar proposal. In 1969, President Nixon terminated the U.S. bioweapons program through an executive order. This executive order stopped offensive bioweapon research and production of the weapons, and it also called for destruction of the arsenal. The United States also adopted the policy to never use any biological or toxic weapons under any circumstances. After this, research efforts in the United States became solely directed toward the creation of defensive methods like vaccines, treatments, and diagnostic tests for potential biologic threats.
1972 - Treaty signed to prohibit biological and toxic weapons
The 1972 Convention on the Prohibition of the Development, Production, and Stockpiling of Biological and Toxin Weapons and on Their Destruction was later created after the proposals of Great Britain and the Warsaw Pact nations. This treaty prohibited the development, possession, and stockpiling of pathogens or toxins. The treaty also required parties to destroy stockpiles of bioweapons within 9 months of signing the treaty. The treaty was ratified in April of 1972, with more than 100 nations signing it, including Iraq, the United States, and the Soviet Union.
Between 1971 and 1972, the United States destroyed pathogens and stockpiles of biologic weapons. Small amounts of certain pathogens were kept so they could be used to test new treatments and vaccines.
1979 - Deadly anthrax outbreak in Sverdlovsk, USSR
 In April and May of 1979, an unusual outbreak of anthrax was reported in the city of Sverdlovsk, USSR.However, reports of this outbreak did not begin to surface in Western news until early 1980. Later that year, articles in Soviet medical, veterinary, and legal journals described the outbreak as naturally occurring in livestock, causing 96 cases of anthrax in humans. Of these cases, 79 were described as gastrointestinal anthrax, and 17 of them were cutaneous anthrax. Soviet officials reported that 64 of these 96 people died from gastrointestinal anthrax.
In April and May of 1979, an unusual outbreak of anthrax was reported in the city of Sverdlovsk, USSR.However, reports of this outbreak did not begin to surface in Western news until early 1980. Later that year, articles in Soviet medical, veterinary, and legal journals described the outbreak as naturally occurring in livestock, causing 96 cases of anthrax in humans. Of these cases, 79 were described as gastrointestinal anthrax, and 17 of them were cutaneous anthrax. Soviet officials reported that 64 of these 96 people died from gastrointestinal anthrax.
Internationally, there was a great debate about the data presented from this outbreak and its accuracy.Some speculated that the outbreak was not naturally occurring among livestock, but that it resulted from activities banned by the Biological Weapons Convention of 1972 (Convention on the Prohibition of the Development, Production, and Stockpiling of Biological and Toxin Weapons and on Their Destruction). All of the cases occurred within 4 kilometers (about 2½ miles) downwind from a Soviet military microbiology facility, and it was suspected that the cases were from the accidental airborne release of anthrax spores. Years later, Western analysts were permitted to review the outbreak to address the speculation. These analysts used data to determine that the anthrax outbreak did occur from the microbiology facility and was the largest outbreak of inhalation anthrax in history. Despite these findings, the Soviet Union maintained that the outbreak was from meat contaminated with anthrax spores. In 1992, then-president of Russia, Boris Yeltsin, admitted that the outbreak was exactly what Western analysts had determined. He stated that the air filters at the biologic facility had not been properly installed the morning of the release, allowing anthrax spores to spew out of the facility.
2001 - Anthrax attack on America
Before 2001, the last case of inhalation anthrax reported in the United States was in 1976. After the September 11 attacks on the World Trade Center and Pentagon, letters filled with a white powder containing anthrax spores were mailed to two U.S. Senators’ offices and news media agencies along the East Coast. Authorities recovered four letters, postmarked September 18, 2001, and October 9, 2001. The powder form allowed the anthrax to float in the air and for it to be breathed in. The powder from these letters contaminated the postal facilities they were processed through as well as the buildings where they were opened.
Until the first few people became ill with anthrax, Americans were unaware of this attack. The first case of inhalation anthrax was diagnosed on October 4, 2001. During October and November of 2001, there were a total of 11 confirmed cases of inhalation anthrax and 11 confirmed cases of cutaneous anthrax. Of the 11 cases of inhalation anthrax, seven of the cases were postal workers who handled the letters or worked in a postal facility where the letters were processed. Two cases were from the AMI Publishing Company, where a photo editor received a contaminated letter. The last two cases were the hardest in which to determine exposure: a 94-year old Connecticut woman and a New York City hospital employee. Investigators thought that the Connecticut women’s mail may have been cross-contaminated in a mail facility; however, no anthrax spores were ever found in her home. The exposure source of the New York City hospital employee is still unknown.
Of the 22 people who got sick with anthrax in 2001, five of them died. All of the people who died had inhalation anthrax, the most serious form of the disease. In all, 43 people tested positive for exposure to anthrax, and 10,000 more people were considered at risk of possible exposure to anthrax.
Before this event, there had never been an intentional release of anthrax in the United States. The FBI conducted an intense 7-year investigation into who may have sent the contaminated letters. Many years after the attacks, advancements in genetic testing allowed the FBI to conduct more complex testing of the spores used in the attack. Once the spores were analyzed, it was determined they came from a strain called the Ames strain and from a single spore batch known as RMR-1029, from a specific research lab. The attack and the subsequent investigation came to be known as Amerithrax. The FBI officially concluded the Amerithrax investigation on February 19, 2010.
Blaney D, Lehman M (2012). Multi-agency investigation of inhalation anthrax—United States, 2011 [Powerpoint slides].
Brachman PS (2002). Bioterrorism: an update with a focus on anthrax. American Journal of Epidemiology, 155(11), 981-987.
Centers for Disease Control and Prevention (2012). A medical victory remains a medical mystery In: NCEZID: Our Work, Our Stories 2011–2012. Atlanta, GA: National Center for Emerging and Zoonotic Infectious Diseases, Centers for Disease Control and Prevention. Available at https://www.cdc.gov/ncezid/pdf/annual-report.pdf
Centers for Disease Control and Prevention (2006). Inhalation anthrax associated with dried animal hides—Pennsylvania and New York City, 2006. Morbidity and Mortality Weekly Report, 55(10);280-282. Available at https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5510a4.htm
Christopher GW, Cieslak TJ, Pavlin JA, and Eitzen Jr EM (1997). Biological warfare: a historical prospective. Journal of the American Medical Association, 278(5), 412-417.
Inglesby TV, Henderson DA, Bartlett JG, Ascher MS, Eitzen E, Friedlander AM, Hauer J, McDade J, Osterholm MT, O’Toole T, Parker G, Perl TM, Russell PK, Tonat K (1999). Anthrax as a biological weapon, medical and public health management. Journal of the American Medical Association, 281(18), 1735-1963.
Inglesby TV, O'Toole T, Henderson DA, Bartlett JG, Ascher MS, Eitzen E, Friedlander AM, Gerberding J, Hauer J, Hughes J, McDade J, Osterholm MT, Parker G, Perl TM, Russell PK, Tonat K; Working Group on Civilian Biodefense (2002). Anthrax as a biological weapon, 2002, updated recommendations for management. Journal of the American Medical Association, 287(17), 2236-2252.
Jernigan JA, Stephens DS, Ashford DA, Omenaca C, Topiel MS, Galbraith M, Tapper M, Fisk TL, Zaki S, Popovic T, Meyer RF, Quinn CP, Harper SA, Fridkin SK, Sejvar SJ, Shepard CW, McConnell M, Guarner J, Shieh W-J, Malecki JM, Gerberding JL, Hughes JM, Perkins BA, and members of the Anthrax Bioterrorism Investigation Team (2001). Bioterrorism-related inhalational anthrax: the first 10 cases reported in the United States. Emerging Infectious Diseases, 7(6), 933-944.
Jernigan DB, Raghunathan PL, Bell BP, Brechner R, Bresnitz EA, Butler JC, Cetron M, Cohen M, Doyle T, Fischer M, Greene C, Griffith KS, Guarner J, Hadler JL, Hayslett JA, Meyer R, Petersen LR, Phillips M, Pinner R, Popovic T, Quinn CP, Reefhuis J, Reissman D, Rosenstein N, Schuchat A, Shieh WJ, Siegal L, Swerdlow DL, Tenover FC, Traeger M, Ward JW, Weisfuse I, Wiersma S, Yeskey K, Zaki S, Ashford DA, Perkins BA, Ostroff S, Hughes J, Fleming D, Koplan JP, Gerberding JL, and National Anthrax Epidemiologic Investigation Team (2002). Investigation of bioterrorism-related anthrax, United States, 2001: epidemiologic findings. Emerging Infectious Disesases, 8(10), 1019-1028.
Knox D, Murray G, Millar M, Hamilton D, Connor M, Ferdinand RD, Jones, GA (2011). Subcutaneous anthrax in three intravenous drug users. Journal of Bone & Joint Surgery, 93-B(3), 414-417.
Lehman MW, Traxler R, Blaney D, Shadomy S, Gomez T, Rubin C, Snippes Vagnone P, Lees C, Miller T, Kightlinger L, Horan V, Murphy T, Amuso P, Schmitz A, Wong D, Treadwell T, Lynfield R (2012). Utilizing partnerships for enhanced surveillance following a case of inhalation anthrax. In: 61st Annual Epidemic Intelligence Service (EIS) Conference, April 16–20, 2012, Atlanta, GA: Centers for Disease Control and Prevention. Available at https://www.team-psa.com/eis/2012/doc/EIS_Program_Book.pdf
Meselson M, Guillemin J, Hugh-Jones M, Langmuir A, Popova I, Shelokov A, Yampolskaya O (1994). The Sverdlovsk anthrax outbreak of 1979. Science Magazine, 266, 1202-1207.
Turnbull PCB, Shadomy SV (2010). Anthrax from 5000BC to AD 2010. In: Bacillus anthracis and Anthrax. NH Bergman, ed., Hoboken, NJ: Wiley-Blackwell.
Sternbach G (2003). The history of anthrax. Journal of Emergency Medicine, 24(4), 463-467.
- Page last reviewed: August 15, 2016
- Page last updated: August 15, 2016
- Content source: