

Estimation of Breastfeeding Rates in the United States from the National Immunization Survey: the Effect of Adding a Cellular Telephone Sample of Respondents
 ShareCompartir
ShareCompartir
Kelley S. Scanlon, PhD RD1; Ruowei Li, MD PhD1; Jian Chen, MS1; Laurence M. Grummer-Strawn, PhD1
1Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Control, Centers for Disease Control and Prevention, Atlanta Georgia
Executive Summary
Before 2011, the National Immunization Survey (NIS) used a landline telephone sampling frame to survey households with young children. However, because cell phones replaced landline phones in many US households, in 2011, the NIS sampling frame was expanded to include a cell phone sample. The combined landline and cell phone sampling, referred to as dual-frame sampling, has continued since the 2011 survey. To estimate the effect on measuring breastfeeding rates, we examined data from the 2011 and 2012 NIS surveys to estimate the difference in breastfeeding rates derived from the landline and dual-frame samples for infants born in 2009 and 2010.
NOTE: This document does not include state tables.
Key Findings
- Adding a cell phone sample to the NIS survey had a minimal effect on national estimates of the percentage of infants ever breastfed and the percentage exclusively breastfed at 3 and 6 months. Dual-frame prevalence estimates for these indicators differed from landline frame estimates by less than one percentage point for infants born in 2010, ranging from 0.5 percentage points lower for exclusively breastfed at 3 months to 0.2 percentage points higher for ever breastfed and 0.8 percentage points higher for exclusively breastfed at 6 months.
- Adding a cell phone sample had a slightly larger effect on national estimates of the duration of any breastfeeding. Among infants born in 2010, the dual-frame estimates were lower than the landline frame estimates by 1.5 and 1.6 percentage points for breastfed at 6 months and at 12 months, respectively.
- Adding a cell phone sample also had an effect on estimates of breastfeeding at the state level, with some states showing higher rates and some showing lower rates. However, the magnitude of the difference was less than 5 percentage points for 75% of the state estimates for infants born in 2010. State breastfeeding estimates from the National Immunization Survey do fluctuate from year-to-year because of the small size of the state samples.
- Based on our findings, we caution against making comparisons of current dual-frame birth-year estimates of breastfeeding duration to more recent landline frame estimates (e.g., 2007 or 2008 birth years) when there was an increasing number of US children living in households with only cell phone service and the National Immunization Survey did not yet include a cell phone sample of respondents. We have less concern about comparing current dual-frame birth-year estimates to landline frame estimates from birth years earlier in the decade when few households were cell phone only.
Full report, 2014
Estimation of breastfeeding rates in the United States from the National Immunization Survey: the effect of adding a cellular telephone sample of respondents
Kelley S. Scanlon, PhD RD1; Ruowei Li, MD PhD1; Jian Chen, MS1; Laurence M. Grummer-Strawn, PhD1
1Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Control, Centers for Disease Control and Prevention, Atlanta Georgia
Introduction
The Centers for Disease Control and Prevention (CDC) uses data from the National Immunization Survey (NIS) to estimate national and state breastfeeding rates among US infants. Before 2011, the NIS used a landline telephone sampling frame to survey households with young children. However, as cellular telephones replaced landline telephones in many US households, representation of the NIS landline survey population to estimate national rates became a concern. By 2011, 36% of children in the United States were living in households with only cellular telephone service.1 The NIS sampling frame was expanded in 2011 to include a cellular telephone sample of respondents. The combined landline and cellular telephone sampling, referred to as dual-frame sampling, has continued since the 2011 survey. The purpose of our analysis was to examine the effect on estimating breastfeeding rates with the addition of the cellular telephone sample to the NIS.
Methods
The National Immunization Survey is an ongoing, random-digit-dialed telephone survey conducted quarterly in 50 states and the District of Columbia among households with children aged 19–35 months.2 In 2011, the NIS sampling frame expanded to include a cellular telephone (cell phone) sample in addition to the usual landline telephone sample. In the first quarter of 2011, screening for age eligible children occurred if the selected cell phone number was associated with a household with a cell phone but no landline phone or if associated with a household with both a cell phone and landline phone if respondent indicated that it was unlikely the landline phone would be answered by anyone in the household. Beginning in the second quarter of 2011, screening for age eligible children occurred for all selected cell phone numbers whether or not a landline phone was answered by household members.
The primary purpose of the National Immunization Survey is to estimate vaccination coverage nationally and by state and selected urban areas. However, questions on breastfeeding have been included in the survey since 2001. In 2011 and 2012, four questions were used to assess whether the infant was ever breastfed, how long the infant was breastfed, how long the infant was exclusively breastfed (breast milk with no solids or other liquids except vitamin/mineral supplements or medications), and the age at which any infant formula was introduced while breastfeeding.3
NIS survey interviews are conducted with the person in the household most knowledgeable about the eligible child’s vaccination history. Starting with the 2011 survey year, eligible children were those aged 19–35 months any time during the sampling quarter. Therefore, each cross-sectional survey year includes children born in earlier calendar years. Multiple survey years are combined to estimate breastfeeding rates by births in one calendar year.3,4 For this report, we combined NIS survey years 2011 and 2012 to estimate breastfeeding rates for infants born in 2009 and 2010. Council of American Survey Research Organizations (CASRO) response rates for the 2011 survey were 61.6% for the landline sample and 25.2% for the cell phone sample; CASRO response rates for the 2012 survey were 64.5% and 30.6% for the landline and cell phone samples, respectively.
For each birth year, we estimated breastfeeding rates for the landline frame sample and the dual-frame (landline and cell-phone) sample.1 The same NIS landline respondents are included in both the landline frame and dual-frame samples for this study but the value of their sampling weights are different for calculation of a landline versus dual-frame rate. For the current analysis, the 2009 births included 16,968 children in the landline frame sample and 23,542 children in the dual-frame sample. The 2010 births included 8,436 children in the landline frame sample and 15,912 children in the dual-frame sample.
aPreviously published provisional rates for 2009 births were based on the landline frame sample from the 2010 and 2011 NIS surveys5; previous published rates for 2010 births were based on the landline sample frame from the 2011 and 2012 NIS surveys.6
For each birth year, we estimated the prevalence of breastfeeding initiation, 6- and 12-month breastfeeding duration, and 3- and 6-month exclusive breastfeeding duration and 95% Confidence Intervals (CI) as weighted percentages. We also calculated the weighted percentage and 95% CI of breastfed infants who were supplemented with infant formula before they were 2 days old. The rate of formula supplementation within the first 2 days was calculated among infants who were breastfeeding at 2 days of age whereas the breastfeeding initiation, duration, and exclusivity rates were calculated among all infants surveyed. All indicators were estimated separately for the landline frame and the dual-frame samples using the landline and dual-frame weights recommended by the National Center for Immunization Respiratory Diseases.2,7 The weighting procedures take into account variation in sampling rates, differential response rates, and differential coverage in the sample compared to the target population. In addition, the weighting procedures for the landline frame sample always have included adjustment for non-coverage of children living in homes without landline phones. Analyses were conducted using statistical software that accounts for complex sample design. The differences between the dual-frame and landline frame prevalence estimates were calculated by subtracting the landline frame estimate from the dual-frame estimate. A 95% CI for each difference between the estimated value of the landline frame and dual-frame was estimated using a procedure developed by NORC at the University of Chicago that accounts for the non-independence of the samples (K.M. Wolter, PhD, written communication, 2011). The procedure uses a condition on the common (landline) sample and assumes that the estimated difference is distributed as a normal random variable with conditional mean and conditional variance. A Taylor series approximation is used to estimate the conditional variance. Differences were considered not statistically significant if the 95% confidence interval around the difference included zero.
Results
National Estimates
Among infants born in 2010, the national estimate (±half width 95%CI) for the percentage of infants ever breast fed based on a dual-frame sample that included landline and cell phone respondents was 76.7% (±1.2), 0.2 (±0.9) percentage points higher than the 76.5% (±1.6) estimated for the landline frame sample (Table 1). The 0.2 point difference was not statistically significant. The effect of adding a cell phone sample of respondents was slightly larger on the national estimates for duration of any breastfeeding. Breastfeeding at 6 months was 1.5 (±2.0) percentage points lower and breastfeeding at 12 months was 1.6 (±1.8) percentage points lower when estimated with the dual-frame compared to landline frame sample, but these differences were also not statistically significant. The effect of adding a cell phone sample on estimates of exclusive breastfeeding was not in a consistent direction. While the dual-frame national estimate for 3 months of exclusive breastfeeding was 0.5 (±0.6) percentage points lower than the landline estimate, the dual-frame estimate for 6 months of exclusive breastfeeding was 0.8 (±0.6) percentage points higher. Only the difference on the 6 months of exclusive breastfeeding indicator was statistically significant. The dual-frame estimate for formula supplementation of breast milk before 2 days of life was 22.8% (±1.4) compared with 24.2% (±1.9) using the landline frame sample. The 1.4 (±1.4) percentage point difference between the samples was not statistically significant.
For 2009 births, the differences between national estimates of breastfeeding initiation and exclusivity derived from the dual-frame and landline frame samples were also less than one percentage point, as was observed for 2010 (Table 2). For breastfeeding at 6 and 12 months, the dual-frame estimates were lower than the landline frame estimates by a magnitude similar to what was observed for 2010 but the differences were statistically significant in 2009. The difference in estimating formula supplementation before 2 days was smaller for 2009 than for 2010 births (Table 2).
State Estimates
Our comparison of dual-frame and landline frame estimates for the smaller state samples revealed considerable variability, with some states showing higher rates and some showing lower rates after the addition of the cell phone sample (Tables 3 and 4). While many states had statistically significantly different breastfeeding estimates after the addition of the cell-phone sample, the magnitude of the difference was less than 5 percentage points for 75% of the state estimates. Our analysis of 2009 births also revealed considerable variability but a smaller magnitude of difference in state breastfeeding estimates when comparing the dual-frame to landline frame sample (Tables 5 and 6). In 2009, about 90% of dual-frame state estimates were within 5 percentage points of the rate based on the landline sample.
Discussion
The addition of a cell phone sample of respondents to the National Immunization Survey in 2011 and 2012 had a minimal impact on specific national estimates of breastfeeding. Among infants born in 2010, dual-frame prevalence estimates for ever breastfed and exclusively breastfed at 3 and 6 months differed from landline frame estimates by less than one percentage point, ranging from 0.5 percentage points lower to 0.8 percentage points higher. The effect on the duration of any breastfeeding at 6 and 12 months was somewhat greater, resulting in national prevalence estimates for 2010 births that were lower by 1.5 to 1.6 percentage points when a cell phone sample was added. For formula supplementation of breast milk before 2 days, the dual-frame estimate was 1.4 percentage points lower than the landline estimate. There was considerable variability in state estimates of breastfeeding, with some states showing higher rates and others showing lower rates after the addition of the cell phone sample. For 2009 births, differences between dual-frame and landline frame national breastfeeding estimates were of a similar magnitude to what was observed for 2010 but not always in the same direction. The difference on the formula supplementation indicator was smaller in 2009. The effect of adding a cell phone sample on state specific estimates varied for 2009 births as it did for 2010 births.
The magnitude of the effect on NIS national breastfeeding estimates when moving from a landline frame to dual-frame sample is slightly greater than the effect reported for estimated immunization rates of the 19- to 35-month-old children surveyed by NIS in 2011.7 For the vaccines examined, the differences between national dual-frame and landline frame estimates ranged from -0.8 to +0.4 percentage points. The differences between landline frame and dual-frame at the state and local level varied by location, with a range of -6.2 to +6.1 percentage points for the vaccines examined.
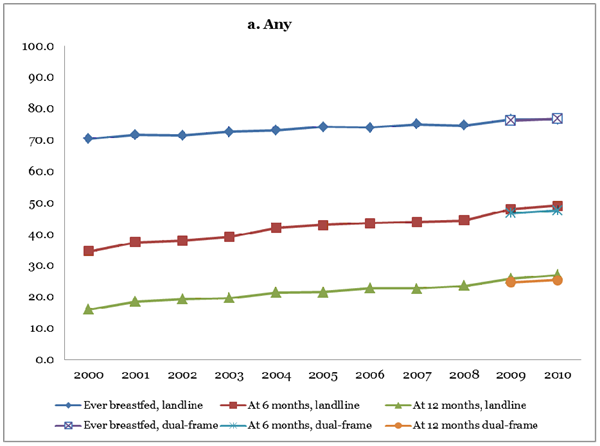
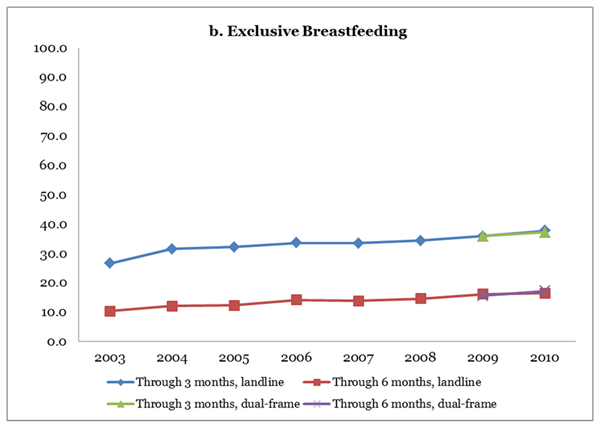
CDC has released annual breastfeeding rates based on landline phone sampling for infants born from 2000 to 2010.8 The survey weights adjusted for non-coverage of non-landline telephone households among other factors.2,7 Figure 1 shows the addition of the national dual-frame rates for infants born in 2009 and 2010 from this study to the landline frame rates for 2000 through 2010. Interpretation of the trends for breastfeeding initiation and exclusivity is minimally affected by the addition of the cell-phone respondents in 2009 and 2010. For breastfeeding duration at 6 and 12 months, a relatively small decrease in the prevalence is noted and needs to be considered when comparing 2009 and 2010 rates with earlier years; however, the decrease does not affect overall interpretation of the trends since 2000. For example, using the landline frame samples from 2005 and 2010, breastfeeding at 6 months increased from 42.9% in 2005 to 49.0% in 2010, a relative increase of 14%. Replacing 2010 with the dual-frame estimate would indicate that breastfeeding at 6 months increased from 42.9% to 47.6% in 2010, a relative increase of 11%. The minimal effect on national trends when comparing current rates with 2005 rates suggests that any differences in breastfeeding behavior by respondents living in households without a landline phone may have been accounted for by the survey weighting procedure applied to the landline frame estimates in 2005.
Our examination of the effect on breastfeeding estimates when a cell phone sample of respondents is added to a survey previously based on a landline sampling frame informs our interpretation of national and state breastfeeding trends. A limitation of our study is that we do not know how much bias there might have been on breastfeeding rates for births before 2009 when a cell phone sample was not available. While the percentage of children living in households with only cell phone service was lower before 2009, it increased from <5% in early 2003 to about 17% by 2008.1 Therefore, bias in landline estimates from more recent birth years (e.g., 2007 and 2008) is of greater concern than from earlier in the decade. Further, the NIS had a lower response rate for the cell phone compared with landline phone sample, but we have no reason to believe that this difference biased our comparison of breastfeeding estimates for the two sampling frames.
As the number of children living in households with only cell phone service increased, it became increasingly important to estimate breastfeeding rates using a sampling frame that included both a landline and cell phone sample of respondents. Starting in 2011, the National Immunization Survey included a cell phone sample of respondents to the sampling frame to improve representativeness of the survey population by accounting for changes in telephone use in the United States. Our analysis found that the addition of the cell phone sample had a minimal effect on national estimates of breastfeeding initiation and exclusivity, but a slightly larger effect on national estimates of breastfeeding duration.
Our analysis showed that adding a cell phone frame also had an effect on estimates of breastfeeding at the state level, with some states showing higher rates and some showing lower rates. State breastfeeding rates estimated from NIS do fluctuate from year-to-year because of the small size of the state samples. A separate analysis comparing 2008 landline state breastfeeding estimates to both landline and dual-frame state estimates for 2009 revealed that the average magnitude of this fluctuation in rates across states was not any greater with the move to dual-frame sampling (K.S.S., unpublished data, 2014).
On the basis of the findings of our study, we caution against making comparisons of current dual-frame birth year estimates of breastfeeding duration to more recent landline frame estimates (e.g., 2007 or 2008 birth years) when there was an increasing number of US children living in households with only cell phone service and the National Immunization Survey did not yet include a cell phone sample of respondents. We have less concern about comparison of current dual-frame birth-year estimates to landline frame estimates from birth years earlier in the decade when few households were cell phone only.
Acknowledgements:
We acknowledge James A Singleton, PhD MS and Laurie D Elam-Evans, PhD MPH for providing statistical consultation for the analysis and critical review of the final document. We also acknowledge statistical and computer programming consultation from Kirk M Wolter, PhD; Ray B Smith, MS; and David S Freedman, PhD.
References
- Blumberg SJ, Luke JV. Wireless Substitution: Early Release of Estimates from the National Health Interview Survey, July–December 2011 website. https://www.cdc.gov/nchs/data/nhis/earlyrelease/wireless201112.htm. Accessed October 3, 2014.
- CDC. Statistical methodology of the National Immunization Survey, 1994–2002. Vital Health Stat. 2005;2(138). https://www.cdc.gov/nchs/data/series/sr_02/sr02_138.pdf [PDF-2.63MB]. Accessed October 2, 2014.
- CDC. National Immunization Survey (NIS) Methods for Estimating Breastfeeding Rates website. https://www.cdc.gov/breastfeeding/data/nis_data/survey_methods.htm. Accessed October 3, 2014.
- Smith PJ, Zhao Z, Wolter KM, Singleton JA, Nuorti JP. Age-period-cohort analyses of public health data collected from independent serial cross-sectional complex probability sample surveys. Paper presented at the Joint Statistical Meeting; 2006: Seattle, WA.
- Centers for Disease Control and Prevention. Breastfeeding Report Card— United States, 2012 website. https://www.cdc.gov/breastfeeding/pdf/2012breastfeedingreportcard.pdf [PDF-299KB]. Accessed October 3, 2014.
- Centers for Disease Control and Prevention. Breastfeeding Report Card— United States, 2013 website https://www.cdc.gov/breastfeeding/pdf/2013breastfeedingreportcard.pdf [PDF-1.12MB]. Accessed October 3, 2014.
- Centers for Disease Control and Prevention. Adding households with cell phone service to the National Immunization Survey (NIS) website. https://www.cdc.gov/vaccines/imz-managers/coverage/nis/child/dual-frame-sampling.html. Accessed October 3, 2014.
- Centers for Disease Control and Prevention. Breastfeeding Among US Children Born 2000–2010, CDC National Immunization Survey website. https://www.cdc.gov/breastfeeding/data/NIS_data/index.htm. Accessed October 3, 2014.
| Table 1. Breastfeeding and Formula Supplementation Rates Among Infants Born in 2010 based on Dual-Frame and Landline Frame Sampling—National Immunization Surveys 2011 and 2012 | |||||
|---|---|---|---|---|---|
| Indicator | Dual-frame Sample | Landline Sample | Difference | ||
| n | Percentage±half 95% CI | n | Percentage±half 95% CI | Percentage±half 95% CI | |
| Ever breastfed | 15912 | 76.7±1.2 | 8436 | 76.5±1.6 | 0.2±0.9 |
| Breastfed at 6 months | 15912 | 47.5±1.4 | 8436 | 49.0±1.9 | -1.5±2.0 |
| Breastfed at 12 months | 15912 | 25.3±1.3 | 8436 | 26.9±1.8 | -1.6±1.8 |
| Exclusively breastfed at 3 months | 15703 | 37.1±1.4 | 8318 | 37.6±1.9 | -0.5±0.6 |
| Exclusively breastfed 6 months | 15703 | 17.2±1.2 | 8318 | 16.4±1.5 | 0.8±0.6* |
| Formula supplementation before 2 days | 12565 | 22.8±1.4 | 6631 | 24.2±1.9 | -1.4±1.4 |
*difference is statistically significant
| Table 2. Breastfeeding and Formula Supplementation Rates Among Infants Born in 2009 based on Dual-Frame and Landline Frame Sampling—National Immunization Surveys 2011 and 2012 | |||||
|---|---|---|---|---|---|
| Indicator | Dual-frame Sample | Landline Sample | Difference | ||
| n | Percentage±half 95% CI | n | Percentage±half 95% CI | Percentage±half 95% CI | |
| Ever breastfed | 23542 | 76.1±1.0 | 16968 | 76.5±1.1 | -0.4±0.6 |
| Breastfed at 6 months | 23542 | 46.6±1.2 | 16986 | 47.9±1.4 | -1.3±1.1* |
| Breastfed at 12 months | 23542 | 24.6±1.0 | 16986 | 25.8±1.3 | -1.2±1.0* |
| Exclusively breastfed at 3 months | 23216 | 35.9±1.1 | 16735 | 35.7±1.4 | 0.2±0.4 |
| Exclusively breastfed 6 months | 23216 | 15.6±0.9 | 16735 | 16.0±1.1 | -0.4±0.6 |
| Formula supplementation before 2 days | 18535 | 23.3±1.1 | 13347 | 23.5±1.4 | -0.2±0.4 |
*difference is statistically significant
Figure 1.a. Trends in breastfeeding initiation and duration by year of birth, National Immunization Survey; b. Trends in exclusive breastfeeding by year of birth, National Immunization Survey
- Page last reviewed: October 5, 2015
- Page last updated: August 2, 2017
- Content source: