

Tracking Candida auris
 ShareCompartir
ShareCompartir
September 18, 2017: Case Count Updated as of August 31, 2017
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area and New Jersey. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
Please note that as of September 18, 2017, the total case counts reported include both probable and confirmed clinical cases; previously reported case counts included only confirmed cases. Case counts for some states are quite a bit higher than those listed before September 18, 2017 because of the change in reporting, and not because of a large increase in new cases. Read more below about how cases are defined.
U.S. Map: Clinical cases of Candida auris reported by state, United States, as of August 31, 2017
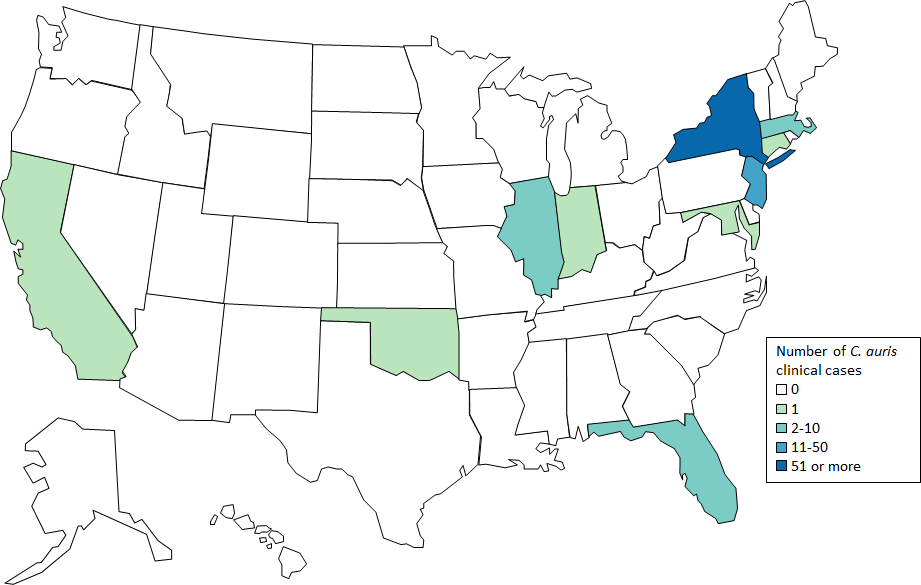
Cases are categorized by the state where the specimen was collected. Most probable cases were identified when laboratories with current cases of C. auris reviewed past microbiology records for C. auris. Isolates were not available for confirmation. Early detection of C. auris is essential for containing its spread in healthcare facilities.
Table: Clinical cases of Candida auris reported by state, United States, as of August 31, 2017
| State | Number and type of clinical Candida auris cases reported | |
|---|---|---|
| Confirmed | Probable | |
| California | 1 | 0 |
| Connecticut | 1 | 0 |
| Florida | 2 | 0 |
| Illinois | 4 | 0 |
| Indiana | 1 | 0 |
| Maryland | 1 | 0 |
| Massachusetts | 3 | 0 |
| New Jersey | 26 | 23 |
| New York | 86 | 4 |
| Oklahoma | 1 | 0 |
| TOTAL | 126 | 27 |
Beyond the clinical case counts reported above, an additional 143 patients have been found to be colonized with C. auris by targeted screening in four states with clinical cases.
CDC will update case counts monthly.
What are clinical cases?
Cases are classified according to definitions established by the Council of State and Territorial Epidemiologists [PDF – 13 pages]. Clinical cases are based on cultures from specimens collected during the course of clinical care for the purpose of diagnosing or treating disease. Confirmed clinical cases are those with isolates that have been confirmed as C. auris in the laboratory.
What are probable clinical cases?
Cases are classified according to definitions established by the Council of State and Territorial Epidemiologists [PDF – 13 pages]. Probable clinical cases are those with supportive laboratory evidence and evidence of epidemiologic linkage (e.g.: C. haemulonii identified in a patient from a facility with other known C. auris cases, but the isolate was not available for confirmatory testing).
Certain laboratory methods commonly misidentify C. auris. Most frequently, C. auris is misidentified as Candida haemulonii, though other misidentifications have occurred. CDC has developed identification, treatment, and infection control recommendations to help prevent the spread of C. auris.
What are screening cases?
Cases are classified according to definitions established by the Council of State and Territorial Epidemiologists [PDF – 13 pages]. Screening is when samples are collected from patients that do not have an infection that is caused by the organism of interest to determine whether or not they may unknowingly be carrying that organism somewhere on their bodies. Colonization means that these patients are found to be carrying C. auris on their bodies, even though they are not sick with the infection. This targeted screening work was conducted as part of an effort to control the spread of C. auris.
CDC encourages all U.S. laboratories that identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov. CDC is working closely with public health and healthcare partners to prevent and respond to C. auris infections. The CDC-sponsored Antibiotic Resistance Laboratory Network (ARLN) will help improve detection and response to C. auris nationwide.
Countries from which Candida auris cases have been reported, as of August 31, 2017
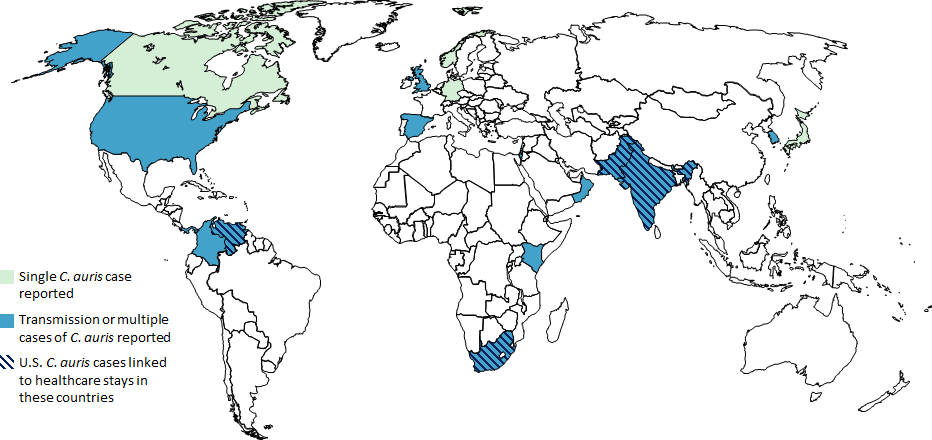
- Single cases of C. auris have been reported from Canada, Germany, Japan, Kuwait, and Norway.
- Multiple cases of C. auris have been reported from Colombia, India, Israel, Kenya, Oman, Pakistan, Panama, South Korea, South Africa, Spain, the United Kingdom, the United States (primarily from New York City Metropolitan Area and New Jersey) and Venezuela; in some of these countries, extensive transmission of C. auris has been documented in more than one hospital.
- U.S. cases of C. auris have been found in patients who had recent stays in healthcare facilities in India, Pakistan, South Africa and Venezuela, which also have documented transmission.
- Other countries not highlighted on this map may also have undetected or unreported C. auris cases.
- Page last reviewed: September 6, 2017
- Page last updated: September 15, 2017
- Content source: