

CDC Rwanda Staff Part of International Ebola Response Team in Guinea
By Joseph Rukelibuga, CDC Rwanda Avian Influenza Specialist
 ShareCompartir
ShareCompartir
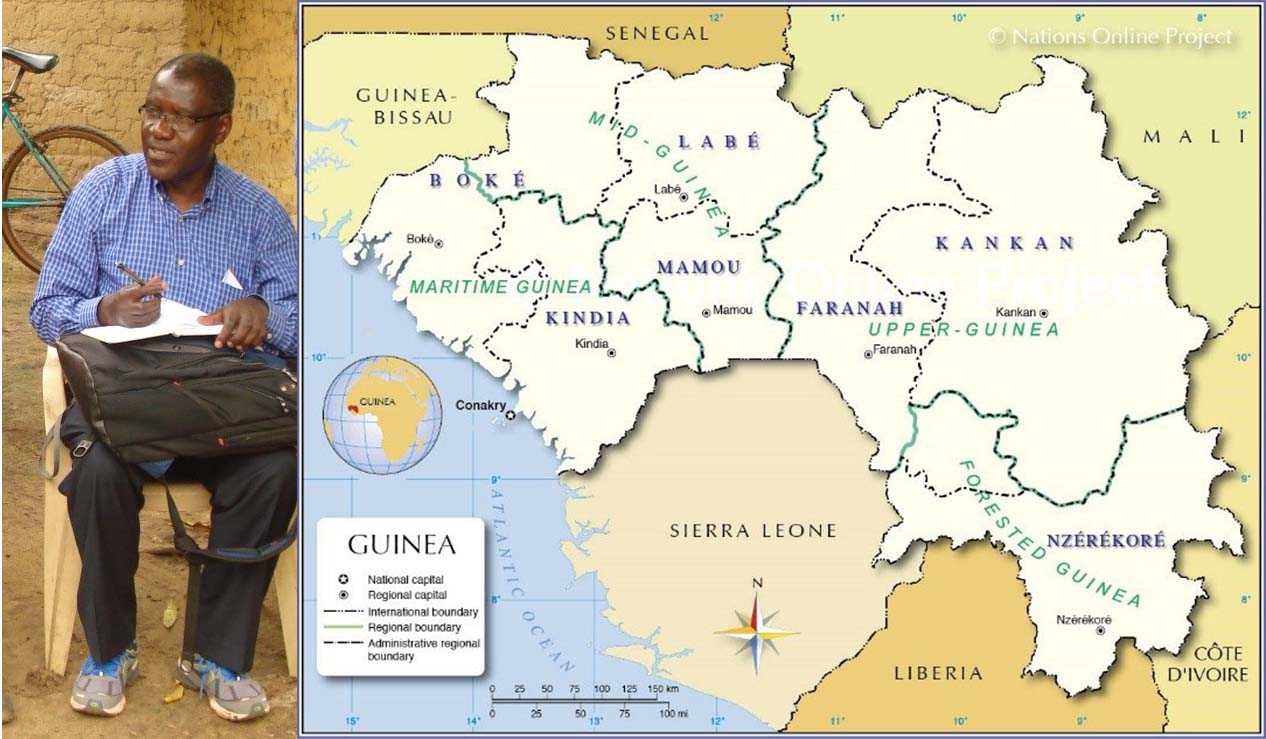
Joseph Rukelibuga in Guinea. Photo: CDC Rwanda.
CDC Rwanda is proud to have had an employee in the CDC International Ebola Response Team in West Africa. Dr. Joseph Rukelibuga is an epidemiologist working for CDC Rwanda as an Avian Influenza Specialist. He was assigned to the International Ebola Response Team in Guinea for a period of 45 days. He tells us his experience in Guinea here.
On February 11, 2015, I received an email from CDC’s Global Disease Detection Operations Center at CDC Headquarters in Atlanta urgently requesting that I join the International Ebola Team in Guinea on a 30-day deployment. The international team was having “tremendous difficulty” recruiting French-speaking staff and was therefore reaching out to French-speaking CDC staff based in Africa to volunteer for deployment to Guinea. They needed volunteers in all areas of the response, including epidemiologists, medics, infection control specialists, health communicators, logisticians, contact tracers, and others. Volunteers of all backgrounds and educational levels were being considered and matched to positions that best suited their skills.
I had mixed reactions to this invitation to volunteer on the International Ebola Response Team. On the one hand, I was excited that this would be my first time to work as part of an International Response Team. I knew the experience would broaden my work experience and expertise. On the other hand, I had real fears about the possibility of getting infected with Ebola and dying far away from my beloved family. So my answer to the email invitation was as follows:
“After consultation with my supervisor, I am glad to let you know that as a French speaker I have accepted to volunteer on the International Ebola Response Team and to be deployed to Guinea for 30 days from May 2015 where I can serve as a contact tracer or trainer. By the way, I have concerns regarding how my Health Insurance will be covered during the deployment period, the medical care in the case it happens I get infected and the management of the post-deployment quarantine. The policy in Rwanda is that any traveler coming from affected countries must undergo a 21-day self-quarantine on his own expenses. I wish to see these concerns addressed before effective deployment.”
My concerns were addressed as follows.
My deployment to Guinea was arranged under the World Health Organization/Global Outbreak Alert and Response Network (WHO/GOARN) mechanism as a WHO short-term Consultant. The mechanism ensures medical insurance and medical evacuation. Before issuance of the WHO contract, I was required to provide an updated CV, a validated WHO Health Form, updated vaccination records, certificates of completion of UN Basic and Advanced Field Security Trainings, a Declaration of Interests (DOI) form, a Designation of Beneficiary form, and more. CDC Atlanta and CDC Rwanda made my travel arrangements for 30 days of deployment in Guinea and 21 days of post-deployment in Atlanta.
At 2 AM on Friday, May 15, 2015, I traveled on Kenya Airways from Kigali, Rwanda, to Bamako, Mali. I arrived at Bamako-Sénou International Airport at noon local time. At the Bamako airport, I watched local Malian TV while waiting for my connecting flight to Conakry, Guinea. The flight from Bamako to Conakry took 45 minutes. This was my first time back in West Africa after 31 years. (In 1984 I had completed my degree in veterinary medicine in Dakar, Senegal.) I was excited to see the West African landscape and the Atlantic Ocean again.
A room was booked for me at the Camayenne Hotel in Guinea. What amazed me was that the city was busy, with all the businesses open, as if everything were normal. This comforted me. I felt that despite the Ebola outbreak, life continued without any apparent fear or stigma in the population. On my first day, I took a shower and fell into deep sleep until the next morning.
We began work the next day. Although it was Saturday, the CDC Guinea Deputy Country Director and Epidemiology Team were in the office early to welcome me and brief me on the situation and my scope of work. I then attended a meeting at the WHO Office and another meeting at the Rwanda Ministry of Health with the Guinean Ministry of Health Surveillance Team. I was then deployed to the field after security and health debriefs by the U.S. Embassy and the WHO. I was also given a smart phone to stay in touch with the teams at the head office. This was the first time I had used a smart phone and I had some difficulties familiarizing myself with it at first.
The Ebola outbreak had been declared in 2014. I expected to see that as of May 2015 the outbreak was almost under control in Guinea. I knew that another Rwandan colleague Dr. Landry Mayigane had been deployed to Guinea on the African Union (AU) Team. He had been in Guinea for six months and had told me that he expected WHO to declare Guinea free from Ebola by December 2015. The AU had already closed down its Ebola response operations.
Other International Ebola Response Team Members included Isaac, an IT Specialist from CDC Kenya; Dr. Katz, a clinician from Israel who used to lead the CDC Kenya Influenza Team; and Dr. Pratima Raghunathan, my former CDC Rwanda Director.
Because of their past experience with Ebola outbreaks, many residents and clinicians from the Democratic Republic of the Congo (DRC) Field Epidemiology and Lab Training Program (FELTP) participated in the response under the African Union, WHO, and CDC umbrella. They were very active in case management in the Ebola Treatment Centers, outbreak investigation, and contact tracing.
I was deployed to the field at the newly active site of Boke, where I supported Ebola contact tracing. I was part of both the CDC team and the WHO Surveillance Team. The WHO Surveillance Team duties included alerts management, investigation, contact follow-up, active case searching, and technical support for communication, epidemiology, and infection control efforts. I assisted with Surveillance Team activities such as investigation of suspected cases prior to sample collection and isolation, investigation of deaths in the community prior to sample collection, safe and dignified burial, and investigating contact tracing around confirmed cases. The investigations were conducted in the local language “Soussou,” and one of the main challenges was with correct translation.
After my 30 days in Guinea came to an end, I requested a 15-day extension while the International Ebola Response Team looked for someone to replace me. I was tired but wanted to stay a little longer because I loved working with such an amazing international team. After 15 days, my replacement arrived. Although I left Boke with an unsatisfied feeling, since I had wanted to see Guinea reach zero Ebola cases while I was still there, I was satisfied with the role I had played.
I remember many things about Guinea. In Conakry, the streets are busy and congested. It is a peaceful country with enormous economic potential. It borders the ocean and has big rivers, bauxite minerals, and a variety of sweet fruits.
An interesting aspect was the healthcare-seeking behavior of Guineans. Most Guineans begin or end their care with traditional healers. When a patient becomes symptomatic, he or she is not often led to a "modern" healthcare facility but rather to a traditional medicine man (except perhaps when at the terminal phase of a disease). This shows the importance attached to traditional medicine by the population and the weight people’s beliefs have on their choice of healthcare.
When I arrived back home in Rwanda, the first thing I wanted to do was sleep in my bed! But after that, I reached out to my family and colleagues to share my experiences in Guinea.
- Page last reviewed: March 1, 2017
- Page last updated: March 1, 2017
- Content source:
Global Health
Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.