

Cluster of Ebola Virus Disease Linked to a Single Funeral — Moyamba District, Sierra Leone, 2014
Weekly / March 4, 2016 / 65(8);202–205
 ShareCompartir
ShareCompartir
Kathryn G. Curran, PhD1,2; James J. Gibson, ; MD3; Dennis Marke, ; MD4; Victor Caulker4; John Bomeh4; John T. Redd, MD5; Sudhir Bunga, MD6; Joan Brunkard, PhD2; Peter H. Kilmarx, MD7 (View author affiliations)
View suggested citationSummary
What is already known about this topic?
Ebola Virus Disease (Ebola) is transmitted person-to-person through direct contact with blood, body fluids, or contaminated clothing and other personal items of symptomatic or deceased patients. Traditional funeral practices, including washing and touching the corpse, pose a substantial risk for Ebola transmission.
What is added by this report?
A single, traditional funeral of a prominent pharmacist was associated with a sharp increase in the number of reported Ebola cases in a previously low-incidence district of Sierra Leone. Twenty-eight laboratory-confirmed cases occurred in persons who reported attending the pharmacist’s funeral. Sixteen (57%) patients had direct contact days or weeks before the funeral, 21 (75%) reported touching the corpse, and eight (29%) died. Rapid and effective outbreak control limited the second and third generations to four cases each, including one death.
What are the implications for public health practice?
Because of the potential for high levels of transmission from a single patient or event, vigilant Ebola surveillance and rapid response are essential, and immediate, safe, dignified burials by trained teams are critical to interrupting transmission and controlling Ebola. Enhanced community-based surveillance strategies, such as a community event-based surveillance system, will be critical to quickly identify high-risk events and prevent ongoing transmission.
As of February 17, 2016, a total of 14,122 cases (62% confirmed) of Ebola Virus Disease (Ebola) and 3,955 Ebola-related deaths had been reported in Sierra Leone since the epidemic in West Africa began in 2014 (1). A key focus of the Ebola response in Sierra Leone was the promotion and implementation of safe, dignified burials to prevent Ebola transmission by limiting contact with potentially infectious corpses. Traditional funeral practices pose a substantial risk for Ebola transmission through contact with infected bodies, body fluids, contaminated clothing, and other personal items at a time when viral load is high; however, the role of funeral practices in the Sierra Leone epidemic and ongoing Ebola transmission has not been fully characterized (2). In September 2014, a sudden increase in the number of reported Ebola cases occurred in Moyamba, a rural and previously low-incidence district with a population of approximately 260,000 (3). The Sierra Leone Ministry of Health and Sanitation and CDC investigated and implemented public health interventions to control this cluster of Ebola cases, including community engagement, active surveillance, and close follow-up of contacts. A retrospective analysis of cases that occurred during July 11–October 31, 2014, revealed that 28 persons with confirmed Ebola had attended the funeral of a prominent pharmacist during September 5–7, 2014. Among the 28 attendees with Ebola, 21 (75%) reported touching the man’s corpse, and 16 (57%) reported having direct contact with the pharmacist before he died. Immediate, safe, dignified burials by trained teams with appropriate protective equipment are critical to interrupt transmission and control Ebola during times of active community transmission; these measures remain important during the current response phase.
The Sierra Leone Ministry of Health and Sanitation and CDC conducted a retrospective analysis of laboratory-confirmed Ebola cases in Moyamba during July 11–October 31, to investigate the increase in cases in September 2014, determine the source and risk factors, and recommend prevention and control measures. The Moyamba District Health Management Team (DHMT) received and responded to alerts from health workers, contact tracers, and community members regarding ill persons, possible Ebola cases, and unexplained deaths. Interviewers completed standardized case investigation forms with patients or proxies regarding demographics, symptoms, illness onset, and potential exposures during the month before illness onset, including contact with ill persons, persons with suspected Ebola, and corpses, plus funeral attendance, hospital or traditional healer visits, and travel history. Laboratory technicians collected whole blood from living patients with suspected Ebola and oral swab specimens from corpses and sent the samples to a centralized laboratory for testing.
A suspected case was defined as 1) the occurrence of fever and at least three of 12 symptoms (i.e., vomiting, headache, nausea, diarrhea, difficulty breathing, fatigue, abdominal pain, loss of appetite, muscle or joint pain, unexplained bleeding, difficulty swallowing, and hiccups) in any person; or 2) any sudden, unexplained death. A confirmed case was defined as a suspected case with a positive laboratory test result by reverse transcription–polymerase chain reaction (RT-PCR) test specific for Ebola virus. If RT-PCR results from blood specimens collected <72 hours after symptom onset were negative or indeterminate, additional specimens were collected for repeat diagnostic testing. Paper case investigation forms and laboratory results were entered into the Sierra Leone Viral Hemorrhagic Fever database. Descriptive statistics were calculated using statistical software.
Confirmed Cases of Ebola
Among 281 suspected Ebola cases in Moyamba District during July 11–October 31, a total of 109 (39%) were confirmed; among these patients, 40 died (case fatality rate = 37%). The median age of patients with suspected Ebola was 30 years (range = 11 months–84 years), and 59% were male. Incidence peaked during the week of September 13–19 at 32 confirmed cases (Figure 1). Overall, during the month before becoming ill, 78 (72%) patients with confirmed Ebola reported having contact with a known or suspected Ebola patient (alive or dead) or ill person. Forty-two (39%) had attended a funeral, 36 (33%) had carried or touched a corpse at a funeral, 10 (9%) had traveled, and eight (7%) had visited a hospital or traditional healer. Among 78 patients with confirmed Ebola who reported contact, 23 (29%) had contact with a corpse, 26 (33%) had contact with a live patient, and 29 (37%) had contact with an Ebola patient both while the patient was alive and after the patient had died.
Attendees at a Single Funeral
During September 5–7, 28 persons who were later confirmed to have Ebola attended the 3-day funeral of a prominent pharmacist in Moyamba; patients developed symptoms a median of 9 (interquartile range = 7–12) days after the funeral (Figure 2). The pharmacist was buried by relatives rather than by a district Ebola burial team, and his death was not investigated; consequently, no epidemiologic records exist regarding his exposures and illness, although anecdotal reports suggested he had treated an Ebola patient from a neighboring village. Among the 28 persons who attended the funeral and later developed Ebola, 23 (82%) were family members and 18 (64%) were male. Eight (29%) of these patients, all of whom were male and had touched the corpse, died and were buried by the district Ebola burial team. The case fatality rate among men was 44%; no deaths occurred among women (p = 0.02). Among the 28 Ebola patients who had attended the funeral, 16 (57%) reported having had direct contact with the pharmacist for days (August 25–September 1) before the funeral, and 21 (75%) carried or touched his corpse at the funeral. Subsequent contact with funeral attendees likely led to eight known additional confirmed cases (four in the second generation, including one death, and four in the third generation) (Figure 2).
Because the pharmacist was suspected to have died from Ebola, Moyamba DHMT engaged the local village chiefs, youth leaders, the community health officer, and others to ensure community support of rapid response measures. Moyamba DHMT conducted case investigations, traced contacts, and established quarantine in the town in mid-September 2014, closing local businesses and providing food support to residents for 21 days. District surveillance officers conducted daily active case finding. A youth leader convened a neighborhood watch, consisting of local, trained youths, who observed contacts of the pharmacist both inside and outside quarantine for Ebola symptoms every day, to support contact tracers and security. DHMT notified the community health officer to be on high alert for Ebola patients at the clinic or in the community; the community health officer notified DHMT soon after when children from the pharmacist’s home became symptomatic. Only two identified contacts of the pharmacist were lost to follow-up.
Discussion
A single, traditional funeral likely led to a sharp increase in Ebola cases in a previously low-incidence district in Sierra Leone, suggesting a substantially higher rate of secondary transmission from one patient than the basic Ebola virus reproduction number of 2.53 estimated for the outbreak in Sierra Leone (4). A high number of secondary cases might be explained by a high viral load in the primary patient, the type of contact, timing of contact (e.g., while a patient was alive or dead), the number of persons exposed, or a combination of these factors. An investigation of the 1995 Ebola outbreak in Kikwit, Democratic Republic of the Congo, identified 38 secondary cases linked to one patient who had many visitors while hospitalized (5).
Eight men with confirmed Ebola who attended this funeral died. The high case fatality rate among men might be explained by more intense or prolonged contact with the corpse by the male funeral attendees. According to traditional funeral practices in Sierra Leone, family and friends of the same sex are often responsible for preparing, washing, and clothing the body (6). Funerals pose a substantial risk for Ebola transmission for several reasons. First, the risk for transmission might increase with viral load, which is often highest in nonsurvivors, especially during the later stages of disease progression and at death (7). Second, the traditional practices of washing, preparing, and touching the body include direct, prolonged contact with the corpse. Finally, funerals attract family, friends, and colleagues from various locations. Attendance is important to demonstrate respect, establish land rights, and determine whether widows will return to their community of origin (6). Travelers who are exposed and become infected can establish new chains of transmission when they return to their original communities.
This report highlights the potential for high levels of transmission from a single patient or event and underscores the importance of vigilant Ebola surveillance and response. At least 36 Ebola cases and nine deaths might have been prevented had the pharmacist had a safe, medical burial. The DHMT’s comprehensive and targeted response, including rapid community engagement, quarantine, and active surveillance through daily house-to-house visits and formation of a youth neighborhood watch, likely led to the prompt identification of cases and limited transmission beyond the four cases in the second generation and the four cases in the third generation.
Fear, stigma, and discrimination might lead to underreporting of Ebola cases (8), and there was likely underascertainment of Ebola cases, deaths, and exposures. During the time of the investigation, Moyamba DHMT and CDC witnessed and received anecdotal reports of persons who were fleeing the area and hiding from surveillance and contact tracing teams. Self-reported data are limited by patients’ and proxies’ ability to recall exposures and dates, and social desirability bias and fear might have led to underreporting of Ebola symptoms and contact with ill persons or corpses.
To achieve and maintain zero new infections, enhanced community-based surveillance strategies, such as the community event-based surveillance system, which employs community health monitors to detect and report Ebola trigger events (e.g., two or more ill or dead family or household members) (9), are critical to the rapid identification of high-risk events to prevent transmission. Safe, dignified burials by trained burial teams using appropriate protective equipment are critical to the interruption of transmission and control of Ebola in both low-incidence and high-incidence settings, as well as in rural and urban settings (10). Early identification of Ebola cases along with prompt isolation, testing, and care of patients can limit transmission, improve likelihood of survival, and ensure safe burials of persons who die, ultimately preventing deaths from occurring at home and unsafe burials in the community. Ebola response teams can strengthen community Ebola surveillance.
Acknowledgments
Moyamba District Health Management Team, including Moyamba District Emergency Operations Committee, surveillance officers, data team, contact tracing team, and clinicians; West Africa Ebola national and international response teams; Ministry of Health and Sanitation, Sierra Leone; World Health Organization; Action Contre la Faim; Médecins Sans Frontieres.
Corresponding author: Kathryn G. Curran, ydh9@cdc.gov, 404-639-4638.
1Epidemic Intelligence Service, CDC; 2Division of Foodborne, Waterborne, and Environmental Diseases, National Center for Emerging and Zoonotic Infectious Diseases, CDC; 3Division of Global Health Protection, Tanzania Country Office, Center for Global Health, CDC; 4Sierra Leone Ministry of Health and Sanitation; 5Office of Public Health Preparedness and Response, CDC; 6Division of Global Health Protection, Center for Global Health, CDC; 7Division of Global HIV/AIDS, Zimbabwe, Center for Global Health, CDC.
References
- World Health Organization. Ebola situation report. February 3, 2016. Geneva, Switzerland: World Health Organization; 2016. http://apps.who.int/ebola/current-situation/ebola-situation-report-3-february-2016
- Brainard J, Hooper L, Pond K, Edmunds K, Hunter PR. Risk factors for transmission of Ebola or Marburg virus diseases: a systematic review and meta-analysis. Int J Epidemiol 2015. Epub. November 20, 2015. https://ije.oxfordjournals.org/content/early/2015/11/20/ije.dyv307.full.pdf+html
- Statistics Sierra Leone. 2004 population and housing census. Freetown, Sierra Leone: Statistics Sierra Leone. http://statistics.sl/2004_population_and_housing_census.htm
- Althaus CL. Estimating the reproduction number of Ebola virus (EBOV) during the 2014 outbreak in West Africa. PLoS Curr 2014;6:ecurrents.outbreaks.91afb5e0f279e7f29e7056095255b288. PubMed
- Khan AS, Tshioko FK, Heymann DL, et al. The reemergence of Ebola hemorrhagic fever, Democratic Republic of the Congo, 1995. Commission de Lutte contre les Epidémies à Kikwit. J Infect Dis 1999;179(Suppl 1):S76–86. CrossRef PubMed
- Richards P, Amara J, Ferme MC, et al. Social pathways for Ebola virus disease in rural Sierra Leone, and some implications for containment. PLoS Negl Trop Dis 2015;9:e0003567. CrossRef PubMed
- Towner JS, Rollin PE, Bausch DG, et al. Rapid diagnosis of Ebola hemorrhagic fever by reverse transcription-PCR in an outbreak setting and assessment of patient viral load as a predictor of outcome. J Virol 2004;78:4330–41. CrossRef PubMed
- Lasuta J. Ebola victims face stigma in West Africa. 2014. http://www.voanews.com/content/ebola-victims-face-stigma-in-west-africa/1902587.html
- Crowe S, Hertz D, Maenner M, et al. . A plan for community event-based surveillance to reduce Ebola transmission—Sierra Leone, 2014–2015. MMWR Morb Mortal Wkly Rep 2015;64:70–3. PubMed
- Nielsen CF, Kidd S, Sillah AR, Davis E, Mermin J, Kilmarx PH. Improving burial practices and cemetery management during an Ebola virus disease epidemic—Sierra Leone, 2014. MMWR Morb Mortal Wkly Rep 2015;64:20–7. PubMed
 FIGURE 1. Confirmed Ebola cases (N = 108), by date of symptom onset and relation to a pharmacist’s funeral* — Moyamba District, Sierra Leone, July 18–October 31, 2014
FIGURE 1. Confirmed Ebola cases (N = 108), by date of symptom onset and relation to a pharmacist’s funeral* — Moyamba District, Sierra Leone, July 18–October 31, 2014
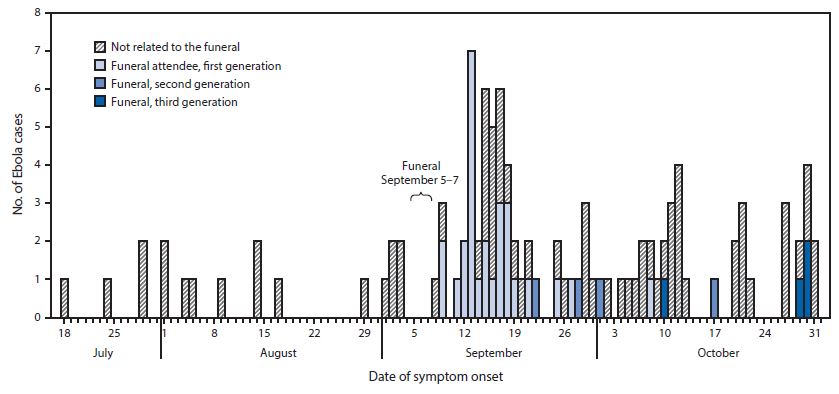
* Excludes case in one funeral attendee for whom date of symptom onset was unknown.
FIGURE 2. Cha?in of Ebola transmission involving 28 attendees at a pharmacist’s funeral (1st generation patients) and eight epidemiologically linked cases, by date of symptom onset — Moyamba District, Sierra Leone, September 5–October 30, 2014
Suggested citation for this article: Curran KG, Gibson, JJ, et al. Cluster of Ebola Virus Disease Linked to a Single Funeral — Moyamba District, Sierra Leone, 2014. MMWR Morb Mortal Wkly Rep 2016;65:202–205. DOI: http://dx.doi.org/10.15585/mmwr.mm6508a2.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All HTML versions of MMWR articles are generated from final proofs through an automated process. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (https://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.
- Page last reviewed: August 25, 2017
- Page last updated: August 25, 2017
- Content source: