

Interim Guidance for U.S. Hospital Preparedness for Patients Under Investigation (PUIs) or with Confirmed Ebola Virus Disease (EVD): A Framework for a Tiered Approach
 ShareCompartir
ShareCompartir
Page Summary
Who this is for: State and local health departments, acute care hospitals, and other emergency care settings, including urgent care clinics.
What this is for: Guidance to assist state and local health departments, acute care hospitals, and other emergency care settings (including urgent care clinics) in developing preparedness plans for patients under investigation (PUIs) for Ebola virus disease (EVD). This guidance does not address Ebola preparedness for primary care offices and other non-emergent ambulatory care settings. Guidance for these settings can be found in Identify, Isolate, Inform: Emergency Department Evaluation and Management of Patients Under Investigation for Ebola Virus Disease [PDF – 1 page].
How this relates to other guidance documents/purpose: This guidance serves as an overarching framework for three other specific CDC guidance documents: Interim Guidance for Preparing Frontline Healthcare Facilities for Patients Under Investigation (PUIs) for Ebola Virus Disease (EVD); Interim Guidance for Preparing Ebola Assessment Hospitals; and Interim Guidance for Preparing Ebola Treatment Centers.
Key Points
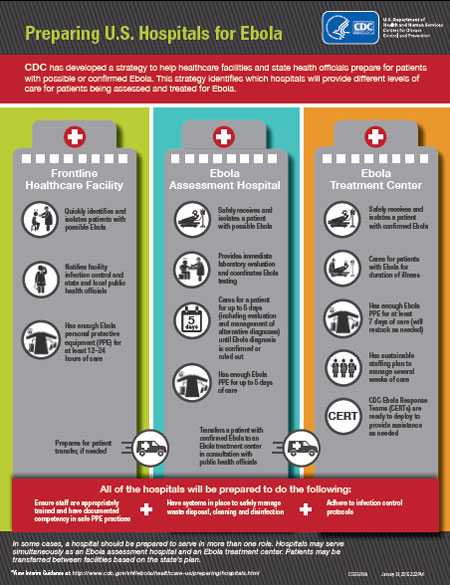
- Acute healthcare facilities can serve one of three roles:
- Frontline healthcare facilities
- Ebola assessment hospitals
- Ebola treatment centers
- To create a coordinated, networked approach, state and local health officials, in collaboration with hospital and healthcare facility executives, may designate healthcare facilities across the state to serve in one of three suggested roles outlined in this guidance document.
- Whereas every state is not obligated to adopt a three-tiered approach, all states are strongly encouraged to identify Ebola assessment hospitals that can successfully manage PUIs until an EVD diagnosis is either confirmed or ruled out while awaiting transfer to an Ebola treatment center.
All U.S. acute healthcare facilities have an important role in preparing to identify, isolate, and evaluate PUIs for EVD and promptly informing public health authorities. However, the roles and the preparations required to perform these tasks will differ by facility. Acute healthcare facilities can serve one of three roles: as a frontline healthcare facility, Ebola assessment hospital, or Ebola treatment center (see Figure). In some cases, a hospital may be prepared to serve in more than one role. Some hospitals may serve simultaneously as an Ebola assessment hospital and an Ebola treatment center. State and local health officials, in consultation with healthcare officials in hospitals and urgent/emergency care settings and emergency medical services providers across the state, should develop a concept of operations plan that describes a networked approach to the evaluation, care, and testing of PUIs , including specific plans for the transfer and treatment of patients with confirmed EVD. As part of Ebola hospital preparedness efforts, hospital officials should develop an internal communications plan to ensure that information is shared in a coordinated way if the facility needs to care for PUIs. An external communications plan to effectively communicate with media, partners, and others should also be developed.
To create a coordinated, networked approach, state and local health officials, in collaboration with hospital executives, may identify healthcare facilities across the state to serve in one of three suggested roles outlined in this guidance document. Whereas every state is not obligated to adopt a three-tiered approach, all are strongly encouraged to identify Ebola assessment hospitals that can successfully manage PUIs or confirmed cases of EVD until an EVD diagnosis is ruled out, especially in states where there is not expected to be an Ebola treatment center. This is particularly important in states where there is not expected to be an Ebola treatment center. Designating assessment hospitals helps to ensure that PUIs have in-state access to care while awaiting transfer to an Ebola treatment center.
Specific CDC guidance can be found in frontline healthcare facilities, Ebola assessment hospitals, and Ebola treatment centers.
Frontline Healthcare Facilities
Most U.S. acute care facilities that are equipped for emergency care (such as hospital-based emergency departments and other emergency care settings including urgent care clinics and critical access hospitals) are in this tier. Frontline healthcare facilities do not include primary care offices and other nonemergent ambulatory care settings. Preparedness guidance for these settings can be found at: Identify, Isolate, Inform: Emergency Department Evaluation and Management of Patients Under Investigation for Ebola Virus Disease [PDF – 1 page].
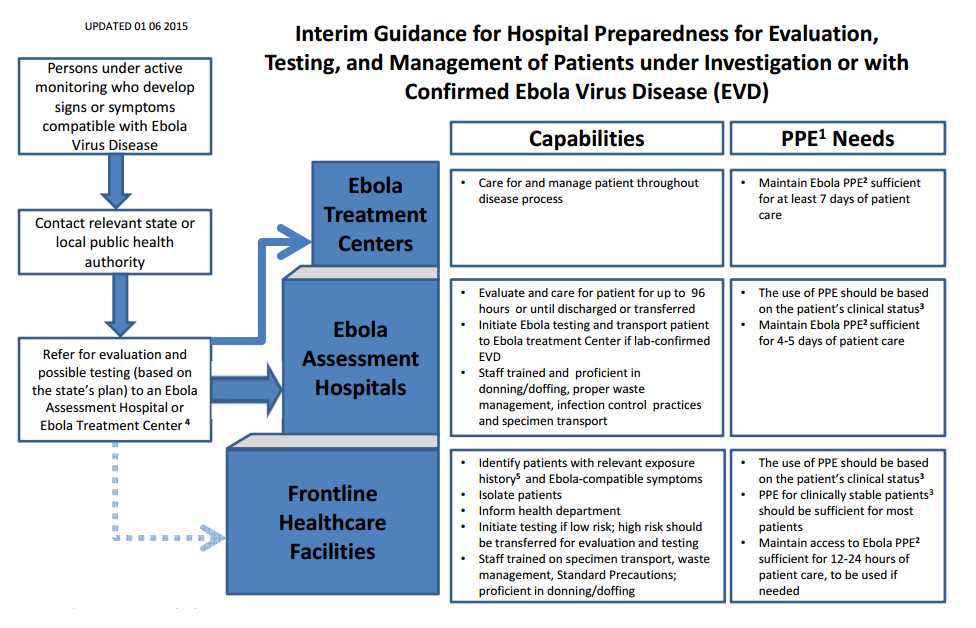
CDC’s Interim U.S. Guidance for Monitoring and Movement of People with Potential Ebola Virus Disease (EVD) recommends active monitoring by state and local public health agencies for all people who have a recognized potential exposure to EVD within the previous 21 days. These people will be directed to designated facilities for evaluation if they become ill. However, it is also possible that patients with unrecognized EVD will present to a frontline healthcare facility without warning or, rarely, patients may be temporarily referred to frontline healthcare facilities when it is not feasible to refer them to an Ebola assessment or Ebola treatment center, based on distance, bed availability, or other considerations. Therefore, frontline healthcare facilities should be prepared to promptly identify and isolate patients who may have EVD and promptly inform the hospital/facility infection control program and state and local public health agency according to the CDC guidance for emergency departments. In some situations, frontline healthcare facilities may also arrange for Ebola testing at the nearest Laboratory Response Network (LRN) laboratory capable of performing testing for EVD, in accordance with the state’s plan. Frontline healthcare facilities are not expected to provide prolonged care (>12–24 hours) for a severely ill patient.
Specifically, frontline healthcare facilities should, in coordination with local and state health authorities, be able to:
- Rapidly identify and triage patients with relevant exposure history AND signs or symptoms compatible with EVD as outlined in CDC’s Emergency Department Evaluation and Management for Patients Under Investigation (PUIs) for Ebola Virus Disease(EVD).
- Immediately isolate any patient with relevant exposure history and signs or symptoms compatible with EVD and take appropriate steps to adequately protect staff caring for the patient, including appropriate use of personal protective equipment (PPE). If the patient has vomiting or bleeding follow the PPE guidance for confirmed Ebola patients or PUIs that have vomiting and diarrhea as outlined here. If the patient is clinically stable, and is not vomiting or having obvious bleeding, follow the PPE guidance for clinically stable persons under investigation for Ebola found here.
- Immediately notify the hospital/facility infection control program, other appropriate facility staff, and the state and local public health agencies that a patient has been identified with relevant exposure AND signs or symptoms compatible with EVD; discuss level of risk, clinical and epidemiologic factors, alternative diagnoses, and plan for EVD testing and further care. Patients who are deemed to have low likelihood of EVD on the basis of clinical and epidemiologic factors and have mild illness, but who nonetheless require EVD testing, may, in some circumstances, remain at the frontline healthcare facility while testing is conducted.
- Frontline healthcare facilities, in accordance with the state’s plan, should consider immediately transferring patients who have a higher probability of EVD or are more severely ill to either an Ebola assessment hospital or to an Ebola treatment center that can provide Ebola testing and care for the higher risk patients until an EVD diagnosis is either confirmed or ruled out. The state plan may include plans to transfer the patient out of state based on the patient’s risk and severity of illness and the geographic location of Ebola assessment hospitals and Ebola treatment centers. Such plans should ensure that transport providers are aware of the patient’s status and have appropriate training and PPE to safely transport a patient to a treatment center.
Ebola Assessment Hospitals
Ebola assessment hospitals are facilities prepared to receive and isolate PUIs and care for the patient until a diagnosis of EVD can be confirmed or ruled out and until discharge or transfer is completed. All states, particularly those not planning to designate Ebola treatment centers, should strongly consider identifying Ebola assessment hospitals to ensure that people with symptoms and exposure history consistent with EVD can be cared for until the diagnosis of EVD is confirmed or ruled out. States should consider selecting enough hospitals to provide adequate geographic coverage across the state and avoid extended transport times of more than 1 to 2 hours from areas in which there are large populations of returning travelers, if possible.
Coordinated public health systems are in place to monitor people potentially exposed to EVD (i.e., active and direct active monitoring). Public health authorities may identify people under monitoring who need testing for EVD if they develop compatible signs or symptoms, and may refer them to Ebola assessment hospitals. These people are likely to have been previously identified as at some level of risk for EVD through airport screening [PDF – 2 pages] and will be actively monitored by public health authorities during the 21 days following travel to an affected country or other potential EVD exposure. Therefore, patients at high risk for EVD should be referred primarily to Ebola assessment hospitals (or treatment centers) rather than frontline healthcare facilities. State and local public health authorities will coordinate closely with facilities when directing patients to a designated Ebola assessment hospital or Ebola treatment center.
- PUIs are likely to present for evaluation with mild symptoms such as isolated fever. Therefore, initial isolation and evaluation of these minimally symptomatic patients can be performed using PPE according to CDC’s guidance for clinically stable persons under investigation for Ebola.
- In addition, Ebola assessment hospitals should be equipped with PPE needed for clinical care of patients with EVD with more severe symptoms and have staff trained in correct PPE use for PUIs who have vomiting, copious diarrhea, or obvious bleeding,
- Because it may take 72 hours or longer after symptom onset to definitively confirm or rule out an EVD diagnosis (with an additional 12 to 24 hours for specimen transport, testing, and identification of another facility for transfer if needed), Ebola assessment hospitals should be prepared to provide care for PUIs for up to 96 hours. Therefore, Ebola assessment hospitals should have PPE for Ebola sufficient for at least 4 to 5 days of patient care and ensure that staff members involved in or supporting patient care are appropriately trained for their roles. This includes demonstrated proficiency in donning and doffing (putting on and taking off) PPE, proper waste management, infection control practices, and specimen packaging and transport.
- In collaboration with public health officials, Ebola assessment hospitals also should be prepared to coordinate Ebola testing, which may involve transferring specimens to an LRN laboratory capable of EVD testing. Decisions about when to transport to an Ebola treament center a PUI for EVD or patient with confirmed EVD should be informed by discussions among public health authorities and the referring and receiving physicians on a case-by-case basis. When the decision has been made to transport a patient, preparations should ensure that transport providers are aware of the patient’s status and have appropriate training and PPE to safely transport a patient to a treatment center.
- Ensure there is no delay in the care of these patients by being prepared to test, manage, and treat alternative etiologies of febrile illness (e.g., malaria in travelers) as clinically indicated.
Ebola Treatment Centers
Ebola treatment centers are facilities that plan to care for and manage a patient with confirmed EVD for the duration of the patient’s illness. State and local decisions to designate Ebola treatment centers are informed by the results of a CDC site visit conducted by an interdisciplinary team of subject matter experts. Site visits assess the hospitals’ ability to meet the minimum criteria (including infection control capacity, physical infrastructure, staffing resources, PPE supplies, waste management processes, worker safety training, environmental services, and laboratory set up). Staff must be trained in and have practiced putting on and taking off (donning and doffing) PPE for Ebola, as well as providing clinical care using PPE.
Given current PPE shortages, Ebola treatment centers may not be able to procure in advance the amount of PPE needed to care for a patient with EVD. Therefore, at a minimum, to be ready to accept and care for patients with EVD, hospitals will need sufficient PPE for at least 7 days. If hospitalization is anticipated to exceed 7 days, state and local health authorities, in collaboration with CDC, may provide or facilitate the procurement of additional PPE supplies. CDC Ebola Response Teams (CERTs) are ready to deploy to any Ebola treatment center to provide technical assistance for infection control procedures, clinical care, and logistics of managing patients with EVD as soon as the health department or hospital requests assistance.
In addition, CDC is available 24/7 for consultation to hospitals and state and local health departments by calling the CDC Emergency Operations Center (EOC) at 770-488-7100 or via email at eocreport@cdc.gov.
Guidance for Ebola Treatment Centers can be found at https://www.cdc.gov/vhf/ebola/hcp/preparing-ebola-treatment-centers.html.
Download PDF version of figure [PDF – 1 page]
- Personal protective equipment (PPE).
- See https://www.cdc.gov/vhf/ebola/hcp/procedures-for-ppe.html for information on recommended PPE for all healthcare workers entering the room of a patient hospitalized with Ebola virus disease (EVD). All staff who may be required to use PPE should be trained for their roles and demonstrate proficiency in putting on (donning) and removing (doffing) of PPE.
- Follow Emergency Department Algorithm for guidance on PPE [PDF – 1 page].
- Patients should be preferentially referred to an Assessment Hospital for testing and evaluation. If severely ill and /or high clinical suspicion of EVD referral to an Ebola Treatment Center could be considered, based on the state’s plan. Patients with confirmed EVD should be transferred to an Ebola Treatment Center. Rarely, patients may be temporarily referred to frontline healthcare facilities when it is not feasible to refer to an assessment hospital or treatment center (e.g., based on distance, bed availability, or other considerations). In some cases, a hospital may be prepared to serve in more than one role.
- Patient has lived in or traveled to a country with widespread Ebola transmission or a country that has had cases in urban settings with uncertain control measures or had contact with an individual with confirmed EVD within the previous 21 days.
- Page last reviewed: August 28, 2015
- Page last updated: August 28, 2015
- Content source: