We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Acetaminophen toxicity
From WikEM
(Redirected from Acetaminophen Overdose)
Contents
Background
- Includes Tylenol and numerous brands and products including acetaminophen
Maximal acetaminophen daily doses
- Adults: 4g/day
- Peds: 75mg/kg/day
Toxic dose
- >10 gm or >200mg/kg as single ingestion or over 24hr period OR
- >6 gm or >150mg/kg per 24hr period x 2days
- 200mg/kg in healthy children 1-6 years of age
The 150 Rule
- Toxic dose is 150mg/kg
- Give NAC if level is >150 mcg/mL four hours post-ingestion
- Initial loading dose of NAC is 150mg/kg IV (140mg/kg PO)
Mechanism of action
- Poorly understood
- Possibly through inhibition of Cyclooxygenase-3 (COX-3)
- Decreases synthesis of prostaglandins
- Antipyresis through inhibition of hypothalamic heat center
Pharmacokinetics
- A - Rapid and near complete absorption
- D - Vd = 0.95 L/kg
- M - T 1/2 = 1.5-2hrs
- 40-60% - Glucuronidation
- 20-40% - Sulfuronidation
- 5-10% - Metabolism through CYP450 (Forms NAPQI)[1]
- E - Conjugated and unconjugated excreted through kidneys
Toxicologic Pathophysiology
- APAP toxic metabolite NAPQI usually quickly detoxified by glutathione stores in liver
- In overdose, glutathione runs out, NAPQI accumulates → liver injury
- NAC increases availability of glutathione
- NAC is a precursor
Clinical Features
Stage 1 (first 24hr)
- Mild nausea and vomiting/malaise
- Hypokalemia (associated with high 4-hr level)
- Massive Ingestion (>500mg/kg) may present with acidemia, coma, hemodynamic changes shortly after ingestion and prior to hepatic necrosis [2] [3]
Stage 2 (days 2-3)
- Improvement in symptoms
- RUQ abdominal pain
- Elevated transaminases
- Elevated bilirubin, PT (if severe)
Stage 3 (days 3-4)
- Recurrence of nausea and vomiting
- Acute liver necrosis → liver failure
- Jaundice
- Coagulopathy
- Encephalopathy (esp with massive ingestions)
- Acute renal failure (1-2%; usually after hepatic failure is evident)
- Pancreatitis (rare)
Stage 4 (after day 5, up to 2 weeks)
- Clinical improvement and recovery (7-8d) OR
- Deterioration to multi-organ failure and death OR
- Continued deterioration
Differential Diagnosis
Acute hepatitis
- Viral hepatitis
- Acute alcoholic hepatitis
- Acetaminophen toxicity
- Mushroom toxicity
- Ischemic hepatitis
Evaluation
Work-Up
- Acetaminophen (APAP) level
- Obtain 4hrs post-ingestion
- Obtaining <4hrs level or "arrival level" is of no diagnostic value
- Obtaining multiple levels is rarely indicated in the absence of hepatotoxicity
- Chemistry
- Metabolic acidosis seen with extremely large ingestion
- LFT
- PT/PTT/INR
- Aspirin levels and other co-ingestants
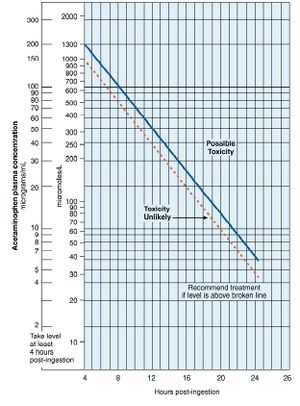
Rumack-Matthew Nomogram
- Only indicated for single, acute ingestion occurring <24hr prior to presentation
- Not useful for chronic ingestion (patients who take supratherapeutic doses for several days) or if time of ingestion is unknown
- Make sure you use the correct units!
- Dotted line should be used for those at higher-risk of liver toxicity (eg alcoholics, those on enzyme-inducing drugs)
- Co-ingestion of drugs that reduce GI motility should prompt repeating acetaminophen level at 8 hrs:
- Opiates
- Anticholinergics (diphenhydramine, etc.)
Management
- Very important to identify time of ingestion. The Rumack-Mathew Nomogram is only for acute acetaminophen ingestions and not useful for chronic ingestions
<4hr after ingestion
- GI decontamination
- Activated Charcoal if <3 hr post-ingestion (no role for multidose activated charcoal)
- Gastric Lavage if high-morbidity coingestants and <1 hr post-ingestion
- Send 4hr APAP level
- Toxic level: Give NAC
- Nontoxic level: No treatment necessary
Between 4-24hr after ingestion
- Send APAP level
- If level will be available within 8hr post-ingestion: wait for level before treating
- If level will not be available within 8hr post-ingestion: do not wait for level before treating
- Discontinue treatment if level returns non-toxic
Unknown or >24hr after ingestion
- Consider GI decontamination for unknown ingestion time
- Give 1st dose of NAC
- Send APAP level, LFT, coags
- APAP level >10 OR elevated transaminases? If yes then continue NAC
- pH <7.3 or PT >100 or creatinine >3.3 or altered mental status? If yes refer to liver transplant unit
- APAP level and LFT both normal? If yes then stop NAC (treatment not indicated)
- APAP level >10 OR elevated transaminases? If yes then continue NAC
Chronic Ingestion
- Initiate NAC in any patient with evidence of ongoing hepatotoxicity (lft abnormalities) OR 'positive' tylenol level (>20 mcg/mL)
- If patient has normal LFT and 'negative' tylenol level (<20 mcg/mL), NAC treatment NOT required
Overdose in Pregnancy
- Both IV or oral NAC may be used in pregnant patients with Acetaminophen toxicity. [4]
- IV formulation may be preferred to increase fetal NAC concentrations
Extended release overdose
- Extended-release acetaminophen (Tylenol ER) consists of acetaminophen 325mg in immediate release (IR) form surrounding a matrix of acetaminophen 325mg
- Several studies show that the elimination of ER and IR APAP preparations is nearly identical after 4 hours. However, some case reports have documented APAP levels that are above the potential toxicity and treatment line on the nomogram as late as 11-14 hours after the ingestion of the ER preparation.
- Recommended management includes the measurement of 4-, 6-, and 8-hour APAP concentrations. Begin NAC therapy if any level crosses above the nomogram treatment line. If the 6-hour level is greater than the 4-hour level, begin NAC therapy.
Massive Ingestion
- >500mg/kg
- May have early acidemia, coma, hemodynamic changes (does not necessarily indicate hepatic damage)
- Supportive care (IVF, pressors, intubation PRN)
- Early consultation with poison control, prior to 4 hour level
- May consider early or increased NAC dosage, dialysis in extreme cases [5]
NAC Treatment
Should begin if:
- The patient's history suggests:acetaminophen ingestion of ≥ 150mg/kg in children or 7.5 g in adults and the results of blood tests will not be available within 8 hours of the ingestion or
- Serum acetaminophen concentration falls on or above the Rumack-Matthew nomogram treatment line or
- While waiting for AST/ALT levels of a patient with a chronic overdose
- Serum levels may not reach peak until up to 4 hours post-ingestion
Adult N-Acetylcysteine Dosing
See above guidelines for when to dose NAC
PO
- 140mg/kg PO load
- 70mg/kg PO q4hr x17 doses additional; dilute to 5% soln
IV
- Loading dose: 150mg/kg in 100 mL D5W over 60min
- Second (maintenance) dose: 50mg/kg in 250 mL D5W over 4hr
- Third dose: 100mg/kg in 500 mL D5W over 16hr
Comments
- Almost 100% effective if given <8 hr post-ingestion; less effective if 16-24 hr post-ingestion
- May still be useful >24 hr post-ingestion, even with fulminant hepatic failure. Give NAC until LFTs improve (not until APAP level is 0) [6] [7]
- Be aware NAC treatment may affect PT. May see a dose-dependent increase in PT following NAC in patients without hepatotoxicity. [8]
Pediatric N-Acetylcysteine Dosing
For children there is a diluent added to the NAC so that there is no electrolyte and volume complications.
PO
- 140 mg/kg body weight, orally, once as a loading dose
- Maintenance Dose: 70 mg/kg body weight, orally, 4 hours after the loading dose and every 4 hours for 17 total doses, unless repeated acetaminophen assays reveal nontoxic levels
100 to 109 kg:
- Loading dose: 15 g (75 mL) in 225 mL diluent; total volume: 300 mL
- Maintenance Dose: 7.5 g (37 mL) in 113 mL diluent; total volume: 150 mL
90 to 99 kg:
- Loading dose: 14 g (70 mL) in 210 mL diluent; total volume: 280 mL
- Maintenance Dose: 7 g (35 mL) in 105 mL diluent; total volume: 140 mL
80 to 89 kg
- Loading dose: 13 g (65 mL) in 195 mL diluent; total volume: 260 mL
- Maintenance Dose: 6.5 g (33 mL) in 97 mL diluent; total volume: 130 mL
70 to 79 kg
- Loading dose: 11 g (55 mL) in 165 mL in diluent; total volume: 220 mL
- Maintenance Dose: 5.5 g (28 mL) in 82 mL diluent; total volume: 110 mL
60 to 69 kg
- Loading dose: 10 g (50 mL) in 150 mL diluent; total volume: 200 mL
- Maintenance Dose: 5 g (25 mL) in 75 mL diluent; total volume: 100 mL
50 to 59 kg
- Loading dose: 8 g (40 mL) in 120 mL diluent; total volume: 160 mL
- Maintenance Dose: 4 g (20 mL) in 60 mL diluent; total volume: 80 mL
40 to 49 kg
- Loading dose: 7 g (35 mL) in 105 mL diluent; total volume: 140 mL
- Maintenance Dose: 3.5 g (18 mL) in 52 mL diluent; total volume: 70 mL
30 to 39 kg
- Loading dose: 6 g (30 mL) in 90 mL diluent; total volume: 120 mL
- Maintenance Dose: 3 g (15 mL) in 45 mL diluent; total volume: 60 mL
20 to 29 kg
- Loading dose: 4 g (20 mL) in 60 mL diluent; total volume: 80 mL
- Maintenance Dose: 2 g (10 mL) in 30 mL diluent; total volume: 40 mL
Less than 20 kg
- Add 3 mL of diluent to each 1 mL (200 mg) of 20% acetylcysteine solution
- Loading dose: 140 g/kg
- Maintenance Dose: 70 g/kg
IV
for pediatrics (0-18) the addition of a dilution of NAC should be followed to avoid electrolyte and fluid problems
5 to 20 kg:
- Loading Dose: 150 mg/kg in 3 mL/kg diluent, infused over 1 hour
- Second Dose: 50 mg/kg in 7 mL/kg diluent, infused over 4 hours
- Third Dose: 100 mg/kg in 14 mL/kg diluent, infused over 16 hours
21 to 40 kg:
- Loading Dose: 150 mg/kg in 100 mL diluent, infused over 1 hour
- Second Dose: 50 mg/kg in 250 mL diluent, infused over 4 hours
- Third Dose: 100 mg/kg in 500 mL diluent, infused over 16 hours
Over 100 kg:
- Loading Dose: 15,000 mg in 200 mL diluent, infused over 1 hour
- Second Dose: 5,000 mg in 500 mL diluent, infused over 4 hours
- Third Dose: 10,000 mg in 1,000 mL diluent, infused over 16 hours
Disposition
- Consider discharge for asymptomatic patients who do not require NAC
- Admission if requiring NAC or other ingestions, injuries
- Transfer to transplant center based on above criteria
- Psych consult if patient has suicidal ideation
- In subacute toxicity, AST/ALT ratio of < 0.4 has sen of 99% for resolving hepatic injury[9]
King's College Criteria
- Criteria for predicting fulminant hepatic failure, and thus referral to transplant center[10]
- PPV 70-90% and sensitivity 69%
- Includes:
- pH<7.3 or lactate>3 at 12hrs after full fluid resuscitation, OR all of the following:
- Cr>3.4
- INR>6.5
- grade 3 or 4 Hepatic Encephalopathy
- Other predictors of APAP-induced hepatic failure include:
- lactate >3.5 4hrs after fluid resusciation
- phos >3.8 at 48hrs, OR
- APACHE II >15
External Links
- MDCalc - Acetaminophen Overdose & NAC Dosing
- MDCalc - King's College Criteria for Acetaminophen Toxicity
Video
References
- ↑ Hendrickson RG, Bizovi KE. Acetaminophen. In: Flomenbaum NE, Goldfrank LR, Hoffman RS, et al, eds. Goldfrank’s Toxicologic Emergencies. 8th ed. New York: McGraw-Hill; 2002:523-543. (Textbook chapter)
- ↑ Roth B, Woo O, Blanc P. Early Metabolic Acidosis and Coma After Acetaminophen Ingestion. Ann Emerg Med. 1999;33(4):452-456.
- ↑ Zein JG, et al. Early anion gap metabolic acidosis in acetaminophen overdose. Am J Emerg Med. 2010;28:798-802.
- ↑ Heard KJ. Acetylcysteine for acetaminophen poisoning. N Eng J Med. 2008;359(3):285-292. (Review)
- ↑ Gosselin S, et al. Extracorporeal treatment for acetaminophen poisoning: Recommendations from the EXTRIP workgroup. Clin Tox. 2014;52:856-867.
- ↑ Keays R, Harrison PM, Wendon JA, et al. Intravenous acetylcysteine in paracetamol-induced fulminant hepatic failure: a prospective controlled trial. BMJ. 1991;303(6809):1026-1029. (Prospective randomized controlled trial; 50 patients)
- ↑ Harrison PM, Keays R, Bray GP, et al. Improved outcome of paracetamol-induced fulminant hepatic failure by late administration of N-acetylcysteine. Lancet. 1990;335(8705):1572- 1573. (Retrospective analysis; 100 patients)
- ↑ Wasserman GS, Garg U. Intravenous administration of Nacetylcysteine: interference with coagulopathy testing. Ann Emerg Med. 2004;44(5):546-547. (Letter)
- ↑ Mcgovern AJ, et al. Can AST/ALT ratio indicate recovery after acute paracetamol poisoning? Clin Toxciol. 2015; 53:164-167.
- ↑ Bailey B, et al. Fulminant hepatic failure secondary to acetaminophen poisoning: a systematic review and meta-analysis of prognostic criteria determining the need for liver transplantation. Crit Care Med. 2003; 31(1):299-305.