We need you! Join our contributor community and become a WikEM editor through our open and transparent promotion process.
Atrial flutter
From WikEM
Contents
Background
- Supraventricular Tachycardia
- Atrial re-entry circuit
- Defined by atrial rate of 250-350, classically 300
Clinical Features
- Asymptomatic
- Palpitations
- Fatigue
- Dyspnea
- Pre-syncope/syncope
Differential Diagnosis
- Can be difficult to distinguish from atrial fibrillation
Palpitations
- Arrhythmias:
- Atrial fibrillation
- Grouped beats on ECG (commonly misdx as A-fib)
- Atrial bigeminy and trigeminy
- Mobitz I or Mobitz II
- Atrial flutter
- SVT
- Ventricular Tachycardia
- Sick sinus syndrome
- Multifocal atrial tachycardia
- PVCs
- Wolff–Parkinson–White syndrome (WPW)
- Sinus node dysfunction
- AV Block
- Lown-Ganong-Levine Syndrome
- Accelerated idioventricular rhythm
- Non-arrhythmic cardiac causes:
- Cardiomyopathy
- CHF
- Mitral valve prolapse
- Congenital heart disease
- Pericarditis
- Valvular disease
- Pacemaker malfunction
- Acute MI
- Psychiatric causes:
- Drugs and Medications:
- Alcohol
- Caffeine
- Meds (i.e. digitalis, theophylline)
- Street drugs (i.e. cocaine)
- Tobacco
- Misc
Evaluation
- ECG
- CBC
- Chem 7
- Magnesium level
- Troponin if patient has chest pain
- Cardiac Echo - if signs of new/worsening heart failure
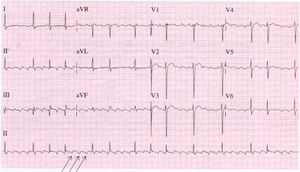

ECG
- Narrow complex tachycardia
- Atrial rate near 300
- Flutter waves (sawtooth pattern) in inferior leads
- AV nodal conduction
- 1:1 conduction can be unstable
- Suggests pre-excitation, sympathetic excess, parasympathetic withdrawal, Class 1C anti-arrhythmic use
- 2:1 conduction is most common
- Suspect atrial flutter whenever ventricular rate is 150
- conduction >2:1
- More commonly even ratio
- Suggests AV nodal blocking agents or AV node disease
- Variable block
- Difficult to distinguish from atrial fibrillation
- Look for: R-R interval that is multiple of P-P interval and mathematical relationship between R-R intervals
- A-fib is completely irregular with no relationship between intervals
- 1:1 conduction can be unstable
- Amal Mattu recommends flipping ECG 180 to easily see inverted P waves or speed machine up to 50 mm/s to stretch out ECG
Types
- Type 1 (Typical Atrial Flutter)
- Re-entry circuit of right atrium (IVC and tricuspid valve)
- Anticlockwise circuit- 90% of cases
- Inverted flutter waves in inferior leads
- Positive flutter waves in V1
- Clockwise circuit
- Positive flutter waves in inferior leads
- Inverted flutter waves in V1
- Anticlockwise circuit- 90% of cases
- Re-entry circuit of right atrium (IVC and tricuspid valve)
- Type 2 (Atypical Atrial Flutter)
- Does not meet criteria for typical atrial flutter
- Less amenable to treatment
Management
Unstable
- Synchronized cardioversion
- Atrial flutter - start at 50 J
- Atrial fibrillation - start at 200 J
- Indications: ischemic chest pain, SBP < 90, acute pulmonary edema, altered mental status
- If shock does not work:
- Verify not preexcitation
- Increase diastolic BP to perfuse the heart
- Push-dose phenylepherine
- Will maintain BP when give rate-control medications
- 50-200mcg q2-5min with goal DBP >60
- Push-dose phenylepherine
- Amiodarone 150mg over 10min (preferably through central venous access) OR diltiazem 2.5mg/min until HR<100 or max 50mg
Stable and Asymptomatic
- If mild or no symptoms and pulse only mildly elevated (<110bpm) ok to manage with PO meds
- Less reactive to PO medication than atrial fibrillation
- Cardioversion is preferred and treats 96-97% of atrial flutter[1]
Stable and Symptomatic
- Goal <110bpm
- Make sure you are not slowing down a normal physiologic response (e.g. fever, hypoxia, etc)
- RACE-II trial demonstrated that lenient control (goal HR < 110bpm) was noninferior to strict control (HR < 80 bpm) in preventing the primary outcome[2]
Cardioversion
- Consider for:[3]
- Symptoms <48hr
- New diagnosis
- No history of similar episodes
- No LV dysfunction
- No mitral valve disease
- No prior thromboembolic event
- Already Anticoagulated
- If cardioversion is considered, pretreatment with rate or rhythm control medications can reduce effectiveness[4]
- 90% effective, 60% effective with pretreatment
Anticoagulation Prior to Cardioversion
- Anticoagulation with Heparin or LMWH should be considered before cardioversion if time permits, otherwise immediately after cardioversion. (unless you are sure it has been <48 hours since onset of afib) [5][6] [7]
- Generally cardioversion while anti-coagulated is believed to be safe with a 1.3% risk of thromboembolism if on aspirin or other anticoagulant[8] However the risk may be as great as 2% risk after 48 hours and preference should be given to anticoagulation prior to cardioversion in longer cases[9]
Evidence of preexcitation
- Avoid AV nodal agents
- Unstable:
- Unsynchronized cardioversion (200J)
- Procainamide (if cardioversion unsuccessful)
- 20-50mg/min until arrhythmia is controlled, hypotension occurs, QRS complex widens by 50% of original width, or total of 17mg/kg is given; followed by continuous infusion of 1-4mg/min
- Stable:
- Try to avoid cardioversion without adequate anticoagulation
Disposition
See Also
External Links
References
- ↑ Gallagher MM, Guo XH, Poloniecki JD, et al. Initial energy setting, outcome and efficiency in direct current cardioversion of atrial fibrillation and flutter. J Am Coll Cardiol 2001; 38:1498.
- ↑ Van Gelder IC et al. Lenient versus strict rate control in patients with atrial fibrillation. N Engl J Med. 2010 Apr 15;362(15):1363-73. full text
- ↑ Ottowa Aggressive Protocol
- ↑ Blecher GE, et al. Use of rate control medication before cardioversion of recent-onset atrial fibrillation or flutter in the emergency department is associated with reduced success rates. CJEM. 2012;14(3):169-177.
- ↑ You JJ, Singer DE, Howard PA, Lane DA, Eckman MH, Fang MC, Hylek EM, Schulman S, Go AS, Hughes M, Spencer FA, Manning WJ, Halperin JL, Lip GY. Antithrombotic therapy for atrial fibrillation: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012 Feb;141(2 Suppl):e531S-75S
- ↑ FusterV et al;American Collegeof Cardiology/ American Heart Association Task Force on Practice Guidelines; European Society of Cardiology Committee for Practice Guidelines; European Heart Rhythm Association; Heart Rhythm Society. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114(7):e257-e354.
- ↑ Camm AJ, Kirchhof P, Lip GY, et al; European Heart Rhythm Association; European Association for Cardio-Thoracic Surgery. Guidelines for the management of atrial fibrillation: the task force for the management of atrial fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31(19):2369-2429.
- ↑ 48hr Cardioversion for A.fib.
- ↑ Nuotio I. et al. Time to cardioversion for acute atrial fibrillation and thromboembolic complications. JAMA. 2014 Aug 13;312(6):647-9
Authors
Colin Hoff, Kevin Lu, Ross Donaldson, Daniel Eggeman, Claire, Neil Young, Daniel Ostermayer